Haydeh Vafa1, Marianna Arvanitakis1, Celso Matos2, Pieter Demetter3, Pierre Eisendrath1, Emmanuel Toussaint4, Axel-Benoit Hittelet5, Jacques Deviere1 and Myriam Delhaye1
Departments of 1Gastroenterology, Oncology and Hepatology, 2Radiology, and 3Pathology, Erasme Hospital, “Université Libre de Bruxelles” (ULB); 4Department of Gastroenterology and Oncology, Institut Bordet. Brussels, Belgium.
5Ambroise Paré Hospital. Mons, Belgium
- *Corresponding Author:
- Haydeh Vafa
Department of Gastroenterology
Hopital Erasme; 808 Route de Lennik
1070 Brussels; Belgium
Phone: +32-2.555.3712
Fax: +32-2.555.46.97
E-mail: haydeh.vafazanjani@erasme.ulb.ac.be
Received January 2nd, 2013 – Accepted March 23rd, 2013
Keywords
Biopsy, Fine-Needle; Endosonography; Pancreas; Tuberculosis
INTRODUCTION
Tuberculosis is a common disease in the developing world and its incidence is slowly increasing in developed countries subsequently to migration and AIDS epidemic. Approximately one eighth of all patients with tuberculosis have extra-pulmonary tuberculosis, with abdominal tuberculosis accounting for 11% to 16% of patients with extra-pulmonary tuberculosis [1].
Pancreatic tuberculosis is a rare entity; it is most often associated with miliary tuberculosis or occurs in the immuno-compromised patients, mostly in endemic regions [2, 3]. It can present with a wide spectrum of symptoms such as abdominal pain, obstructive jaundice, iron deficiency anemia, pancreatic abscess, acute/chronic pancreatitis, splenic vein thrombosis and a pancreatic mass mimicking malignancy [4, 5]. However, diagnosis of pancreatic/para-pancreatic tuberculosis is a clinical challenge, with most cases diagnosed only after surgical exploration, for presumed pancreatic cancer. Here we report five cases of pancreatic tuberculosis each time with a different clinical presentation, in an occidental country setting where the diagnosis was made by EUS-FNA.
CASE REPORT
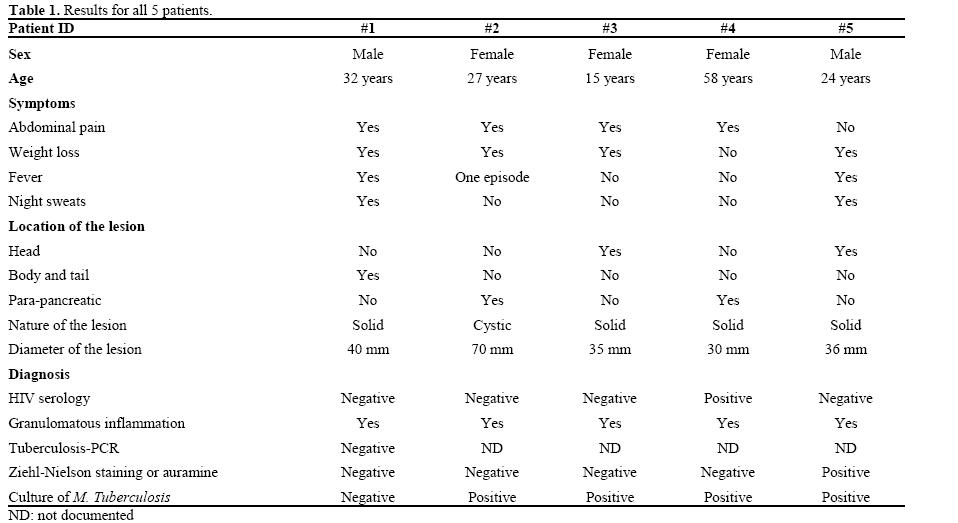
Between January 1st, 2003 and December 31st, 2011, 2,855 new patients with pancreatic disease were admitted in our institution among which 5 were diagnosed with pancreatic/para-pancreatic tuberculosis (Table 1).
EUS-FNA was performed using a linear array echoendoscope (GF-UCT 140; Olympus, Tokyo, Japan), under general anesthesia and antibiotics (a single dose of amoxicillin-clavulanate) [6]. A puncture was made by using a 19- or 22-gauge needle (Wilson Cook Endoscopy, Winston-Salem, NC, USA) guided by real time EUS imaging. The aspirated material was smeared onto glass slides fixed immediately in 95% absolute alcohol for rapid on-site cytopathological examination and placed in a formalin solution for pathologic examination (hematoxylin and eosin staining). According to the index of clinical suspicion, bacteriological cultures for Mycobacterium Tuberculosis (M. Tuberculosis) of aspirated material, tuberculosis-specific polymerase chain reaction (PCR) and acid-fast bacilli staining were performed.
Patient #1
A 32-year-old African man was admitted for right upper quadrant abdominal pain. Two weeks earlier he presented with fever, night sweats and coughing. His last trip to Africa was 8 years earlier. Chest CT scan showed bilateral pleural effusion with normal mediastinal lymph nodes. Abdominal ultrasound showed perihepatic ascites, enlarged lymph nodes within liver hilum and a solid pancreatic mass. Abdominal CT san and magnetic resonance imaging (MRI) showed a heterogeneous solid mass located in and adjacent to the pancreas (Figure 1). EUS confirmed a heterogeneous mass adjacent and involving pancreatic parenchyma at the genu. FNA revealed granulomatous necrotic lesions compatible with tuberculosis. The patient was put on quadritherapy (rifampicin, isoniazid, ethambutol and pyrazinamide) with a rapid clinical improvement.
Figure 1. Abdominal MRI: ascites (short arrow) and a heterogenous
solid mass located in and adjacent to the pancreas (long arrow)
(Patient #1).
Patient #2
A 27-year-old Maroccan born female, living in Belgium, was admitted for fever of unknown origin. Other symptoms included weight loss, continuous epigastric and right upper quadrant pain for three months. Upon admission, abdominal ultrasound showed a large cystic lesion around the liver hilum associated with a portal cavernoma. Abdominal CT scan followed by abdominal MRI confirmed the presence of a heterogeneous polycystic mass adjacent to the pancreas within the lesser sac without dilatation of the main pancreatic duct (Figure 2). The patient underwent EUS-FNA, which allowed the aspiration of a yellowish purulent liquid, a sterile exudates rich in neutrophils upon analysis. Surgical resection of the cyst was scheduled based on the suspected diagnosis of an infected mucinous cystadenoma; the day before the surgery a positive result for M. Tuberculosis culture from the cyst fluid was received. Chest CT scan was normal. The patient was put on anti-tuberculin therapy, her symptoms resolved quickly. Control CT showed a significant decrease of para-pancreatic lesion.
Figure 2. Contrast enhanced MDCT coronal reformat shows a large
multicystic, septated lesion located in the lesser sac (long arrow).
Associated cavernous transformation of the portal vein is seen (short
arrow) (Patient #2).
Patient #3
A 15-year-old girl originating from Burundi and living in Belgium since the age of 5, consulted for intermittent heart burn, epigastric pain and weight loss. Abdominal ultrasound and MRI revealed a pancreatic mass associated with common bile duct obstruction and lack of main pancreatic duct dilatation (Figure 3ab). EUS confirmed a heterogeneous, poorly vascularized mass within the pancreatic head, compressing the CBD. FNA showed granulomas with necrotic areas suggesting tuberculosis. Cultures for M. Tuberculosis were positive. She was treated successfully with antituberculin therapy. The control MRI three months later showed a complete resolution of the pancreatic mass (Figure 3cd).
Figure 3. a. MRCP shows distal common bile duct obstruction (short arrow). Main pancreatic duct is not dilated. b. Coloured map of T2-weighted
and Diffusion-weighted sections through the head of the pancreas displaying a space-occupying lesion with cellular proliferation (long arrow).
Control MRI shows almost complete resolution of bile duct obstruction (c.) and a normal pancreatic head (d.). (Patient #3).
Patient #4
A 58-year-old HIV positive African woman presented with recent right upper quadrant pain. HIV infection was well controlled under treatment with efavirenz and a combination of abacavir and lamivudine. An abdominal CT scan showed a heterogeneous mass adjacent to the pancreatic head, suspicious of malignancy. MRI showed an extra-pancreatic retroperitoneal mass corresponding to necrotic lymph nodes. FDG PET CT was performed showing multiple retroperitoneal lymph nodes with high suspicion of malignancy (MRI-PET fusion). The patient underwent EUS-FNA, which confirmed the presence of several necrotic lymph nodes within liver hilum as well as ascites. Cultures for M. Tuberculosis of the necrotic material sampled by FNA were positive. The patient was put on quadritherapy with a good clinical outcome. Control FDG PET CT six months later showed complete regression of the retroperitoneal lymph nodes.
Patient #5
A 24-year-old Belgian heroin addict man was admitted for productive cough, temperature and weight loss of 10 kg. Pulmonary tuberculosis was right away diagnosed based on chest X-ray and positive expectorations. He was put on quadritherapy. Despite the treatment he continued to present fever 2 months later. An abdominal ultrasound followed by abdominal CT scan showed a heterogeneous solid mass within the pancreatic head causing common bile duct dilatation. An EUS-FNA sample showed a granulomatous necrotic material with positive culture for M. Tuberculosis. The quadritherapy was prolonged for a total of 9 months, the treatment is still ongoing and the patient is followed regularly.
DISCUSSION
Tuberculosis incidence in Belgium is 10.3 for 100,000 inhabitants and abdominal tuberculosis, which includes pancreatic and para-pancreatic tuberculosis, represents 0.6% [7]. Pancreatic tuberculosis remains a rarity even in endemic regions. In India, Bhansali found no pancreatic tuberculosis in 300 patients with abdominal tuberculosis [8]. Auerbach reported on 1,656 autopsies with tuberculosis: 297 (17.9%) had acute generalized tuberculosis, but only 14 (4.7%) of them had pancreatic involvement [2]. Paraf et al. identified only 11 (2.1%) cases with pancreatic or peri-pancreatic involvement in 526 miliary tuberculosis cases between 1891 and 1961 [3]. Pancreatic tuberculosis is even rarer in Western countries and only case reports or short case series (3 cases) exist so far [9]. In our experience, during a 9- year period, we have identified only 5 cases of pancreatic/para-pancreatic tuberculosis, which represents a frequency of 0.17% of all pancreatic diseases requiring hospital admission.
Pancreatic and para-pancreatic tuberculosis can present with a variable spectrum of symptoms, commonly reported symptoms are abdominal pain, nausea, vomiting, weight loss and fever [10, 11, 12]. Patients may present with an obstructive jaundice and a pancreatic mass, which is indistinguishable from pancreatic neoplasia. All of our patients presented with weight loss but only two of them presented the typical picture of fever and night sweats. Physicians should have in mind pancreatic tuberculosis while assessing non specific abdominal pain in patients with high risk factors such as patients from endemic areas, HIV patients, prisoners and urban poor.
As illustrated in this report imaging findings in pancreatic tuberculosis are also variable and challenging, pancreatic tuberculosis can present as a cystic or solid pancreatic mass mimicking pancreatic cancer [9, 10, 11, 12].
In our series CT and/or MRI had reported pancreatic/para-pancreatic tuberculosis as a potential differential diagnosis only for two patients (Patient #1 and #4). EUS-FNA allowed a correct diagnosis in all of our cases. The diagnostic accuracy of EUS-FNA in pancreatic tuberculosis is difficult to determine due to the rarity of this entity [13]. The largest series published so far is a retrospective Korean series of 21 cases of pancreatic and para-pancreatic tuberculosis. In this study 13 patients (62%) showed granulomatous inflammation, 10 of 15 patients (67%) were positive on a tuberculosis PCR assay, Ziehl-Neelsen staining was positive in 4 out of 15 patients (27%), and 3 of 8 patients (38%) had positive cultures for M. Tuberculosis. EUS-FNA correctly diagnosed pancreatic/para-pancreatic tuberculosis in 16 patients (76%), avoiding unnecessary surgery [14].
The presence of granulomas in a pancreatic FNA specimen is highly suspicious of pancreatic tuberculosis; this was observed in all our patients. Moreover, the diagnosis needs to be confirmed either by Ziehl-Neelsen staining or a positive culture. The sensitivity of histochemical staining of Koch bacillus is as low as 20% to 40%. Culture results are positive only in 77% of cases. This procedure can take several weeks due to the recovery period of the organism [15]. Ziehl- Neelsen staining was positive in only one patient and tuberculosis culture was positive in four.
PCR assay is increasingly used to rapidly detect M. Tuberculosis. This technique has a sensitivity of 64% [15]. However, since drug susceptibility cannot be determined by PCR assay, standard cultures also need to be performed.
In conclusion, pancreatic/para-pancreatic tuberculosis is an extremely rare entity especially in non endemic regions, with clinical and radiological findings mimicking pancreatic malignancy. EUS-FNA is a good tool to confirm tuberculosis diagnosis determining therapeutic management.
Conflict of interest
The authors have no potential conflict of interest
References
- Khan R, Abid S, Jafri W et al. Diagnostic dilemma of abdominal tuberculosis in non-HIV patients: an ongoing challenge for physicians. World J Gastroenterol 2006; 12: 6371-6375.
- Auerbach O. Acute generalized miliary tuberculosis. Am J Pathol 1944; 20:121-136.
- Paraf A, Menager J, Texier J. Tuberculosis of the pancreas and tuberculosis of the lymph nodes of the upper region of the abdomen. Rev Med Chir Mal Foie 1966; 41: 101-126.
- Crowson MC, Perry M, Burden E. Tuberculosis of the pancreas: a rare cause of obstructive jaundice. Br J Surg 1984; 71: 239.
- Stapmbler JB, Klibaner MI, Bliss CM et al. Tuberculous abscess of the pancreas. Endoscopy 1981; 13: 178-80.
- Adler D, Jacobson BC, Davila RE et al. ASGE guidelines: complications of EUS .Gastrointest Endosc. 2005; 61: 8-12.
- Fonds des Affections Respiratoires - FARES asbl. Bruxelles, Belgique. https://www.fares.be/content/view/175/239/
- Bhansali S. Abdominal tuberculosis; Experience with 300 cases. Am J Gastroenterol 1977; 67: 324- 337.
- Suvadip C, Matthias LS, Anderson K et al. Tuberculosis of the pancreas: A diagnostic Challenge solved by Endoscopic Ultrasound, a case series. J Gastrointes Liver Dis 2012;21 ,105-107.
- Chaudhary A, Negi SS, Sachdev AK et al. Pancreatic tuberculosis: still a histopathological diagnosis. Dig Surg 2002, 19; 389-392.
- Schneider A, von Birgelen C, Duhrsen U et al. Two cases of pancreatic tuberculosis in nonimmunocompromised patients; a diagnostic challenge and a rare case of portal hypertension. Pancreatology 2002, 2; 69-73.
- Weiss ES, Klein WM, Yeo CJ. Peripancreatic tuberculosis mimicking pancreatic neoplasia. J Gastrointest Surg 2005, 9; 254- 262.
- Cheng R, Grieco VS, Shuhart MC, Rulyak SJ. EUS-guided FNA diagnosis of pancreatic tuberculosis.Gastrointest Endosc 2006; 64: 660-663.
- Song TJ, Lee SS, Park DH et al. Yield of EUS-guided FNA on the diagnosis of pancreatic /peripancreatic tuberculosis. Gastrointest Endosc 2009; 69: 484-491.
- Woodfield JC, Windsor JA, Godfrey CC et al. Diagnosis and management of isolated pancreatic tuberculosis: recent experience and literature review. J Surg 2004; 74: 368-371.




