Keywords
Anastomosis ; Surgical; Gastrostomy; Jejunostomy; Pancreatic Fistula; Pancreatectomy
Abbreviations
CP central pancreatectomy; POPF postoperative pancreatic fistula; PG pancreatico-gastrostomy; PJ pancreaticojejunostomy
INTRODUCTION
Pancreatic tumors have been traditionally treated either by pancreaticoduodenectomy (PD) or distal pancreatectomy.
Development of cross sectional and functional imaging has improved the diagnosis of small low-grade pancreatic tumors, and their discrimination from potentially malignant tumors. Benign and low-grade tumors often occur in young patients with high life expectancy, leading to the development of parenchyma sparing techniques to preserve long-term endocrine and exocrine pancreatic function.
Central pancreatectomy (CP) and enucleation are alternatives to more extensive surgeries for benign or low-grade malignancy tumors in pancreatic isthmus management [1]. CP allows the resection of tumors up to 5 cm while enucleation is limited to small lesions far from the main pancreatic duct [2].
Though CP is performed on less severe patients than PD, CP is associated with a similar or even higher morbidity rate, and with a non-nil mortality rate [3, 4].
These outcomes are mainly related to a high postoperative pancreatic fistula (POPF) incidence after CP. The most common explanation is the presence of two pancreatic remnants, mainly the distal remnant [3].
Surgical and perioperative features have been extensively studied in PD in order to decrease POPF risk. In this context, the role of the pancreatico-enteric anastomosis is still debated [5, 6, 7, 8].
In a previous study, Venara et al. showed that pancreatico-gastrostomy (PG) was associated with a significantly higher POPF rate than pancreaticojejunostomy (PJ) after CP, but failed to show a clinically relevant difference in severity of outcomes between the two techniques [9].
In order to confirm these results, this study was designed (i) to confirm that PJ was associated with a significant decrease of POPF incidence than PG, and (ii) to determine if PJ resulted in a reduced high-grade fistula rate and severity of outcomes after CP.
METHODS
Study Design
A retrospective study was performed with four French referral centers from January 1988 to December 2011.
Twenty-five patients from Nantes and Angers were the population analyzed in an initial study from Venara et al. [9]. In order to empower the study, we included patients from University Hospitals of La Timone (Marseille) and Rennes (Figure 1).
The study included all patients with a proven or suspected to be benign or low-grade malignancy tumor located in the middle part of the pancreas, and who underwent a CP with the realization of PJ or PG.
Exclusion criteria were age under 18 and preoperative suspicion of malignant tumor.
Intervention
Experienced surgeons performed all procedures according to a standard technique described by Sastre et al. [10]. The PJ was a trans-mesocolic single plan endto- side anastomosis. The PG was a single layer end-toside anastomosis. Both anastomoses were performed with single-sutures; the number of which was left to the surgeon’s opinion. No double omental flap was performed to protect the anastomosis.
There was no use of preoperative prophylactic somatostatin analogues.
Systematic external drainage was at the side of the pancreatico-enteric anastomosis. Internal main pancreatic duct stenting could be used depending upon the surgeon’s practice.
Postoperatively, systematic measurement of amylase in drains was carried out on the third or fifth day, or more frequently if there was a proven fistula.
Outcomes
POPF diagnosis was done in cases with amylase in the external drains that increased more than three fold from the amylase serum value on postoperative day 3 or 5 (according to ISGPF definition) [11]. Anastomotic leak severity was classified both according to the scoring system of Bassi et al. [11] and to the classification proposed by Dindo et al. [12].
Delayed gastric emptying was assessed in cases of inability to return to standard diet one week after surgery, including prolonged nasogastric intubation of the patient according to IGSPS definition [13].
Postoperative pancreatic endocrine insufficiency was defined as fasting plasma glucose level at least 7.0 mmol/L and the need for diet modification, oral medication or insulin, or the need of extra-medication in case of preexistent diabetes.
Postoperative pancreatic exocrine insufficiency was defined as persistent symptoms (eg, steatorrhea) requiring pancreatic enzymes supplementation.
Sample Size Estimation and Statistical Analysis
This study was powered as a superiority trial; the design based on the previous results from Venara et al. [9]. The null hypothesis was that PJ and PG were associated with similar POPF rates after CP. The alternative hypothesis was that PJ was superior to PG with regard to POPF incidence reduction. POPF rates were respectively taken to be 20% in PJ group and 70% in the PG group considering the previous results of 18.1% and 71.4% [9]. Group sample sizes were taken to be 19 in each group to detect a significant difference between the groups with a significant level of 0.05 and a 90% power.
Data on patient co-morbidities, operative features, and postoperative course were prospectively collected, retrospectively collated in a Microsoft Excel® spreadsheet and statistically analyzed using SPSS® software (version 22). Qualitative data are expressed in percentages and quantitative data in mean ± SD. The Chi2 test was used for categorical variables and the Mann Whitney or Kruskal Wallis test were used for quantitative variables. The difference was considered statistically significant when the p-value was less than 0.05 (p<0.05).
RESULTS
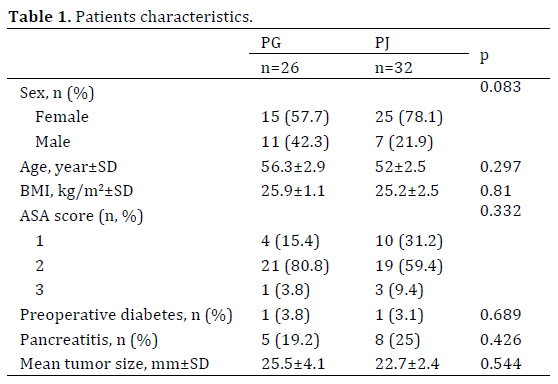
Fifty-eight patients, 40 women and 18 men were analyzed. The mean age was 53.9±1.9 years and the mean follow up after hospital discharge was 36.2±3.9 months. Twenty-five patients (44.8%) had PG and 32 patients (55.2%) had PJ.
Preoperative staging included computed tomography in 84.7% of cases, endoscopic ultrasonography in 88.1% of cases, and magnetic resonance imaging in 64.4% of cases.
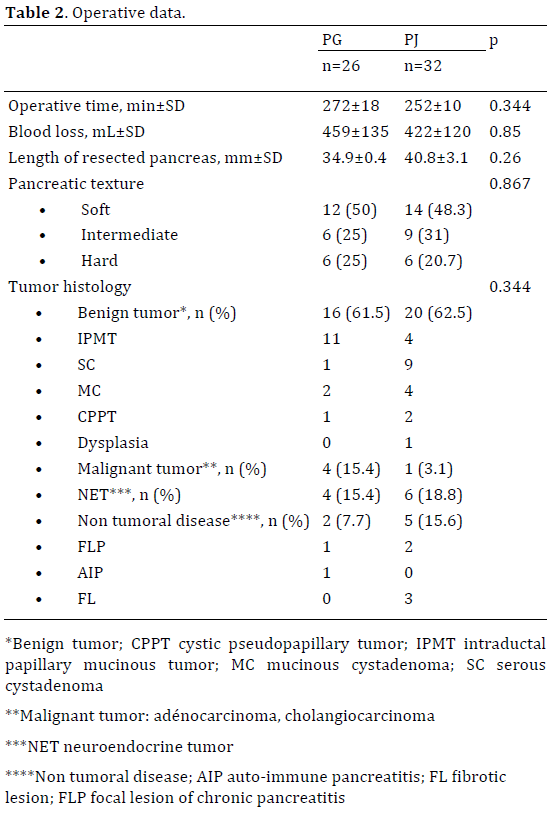
There was no difference between the two groups with regard to medical history (Table 1) or operative data (Table 2). Histological diagnoses of pancreatic tumors were similar in the two groups.
The postoperative complications are reported in Table 3.
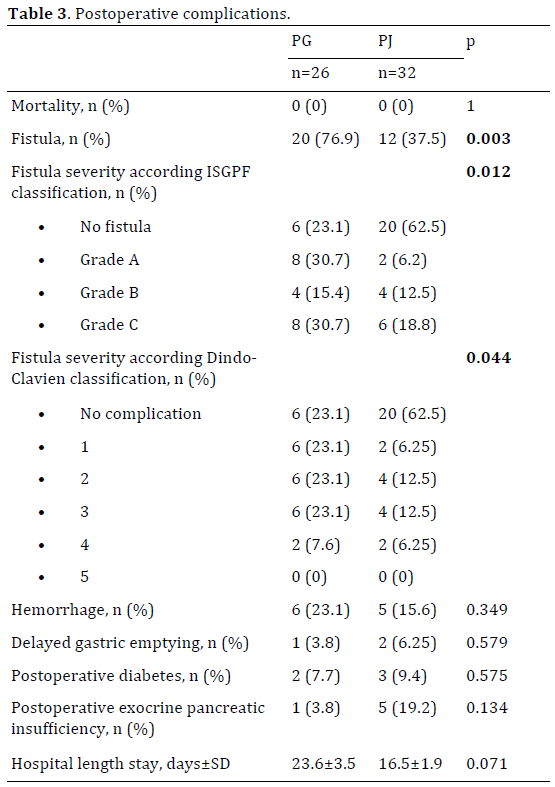
POPF incidence was significantly increased after PG (76.9% vs. 37.5%, p=0.003).
PG was associated with significantly higher grade of fistula, both when graded with ISGPF classification (p=0.012) and Clavien-Dindo classification (p=0.044).
There was no death related to POPF in this series. A 54-year-old woman who underwent CP with PJ for a 24 mm mucinous cystadenoma died because of massive pulmonary embolism on postoperative day 1, and thus excluded from analysis.
Postoperative hemorrhage complication did not differ after PG and PJ (23.1% vs. 15.6%, p=0.349).
Surgical re-intervention was necessary in 8 cases (13.8%). Severe complications due to POPF, which did not required surgery, were radiologically managed, either with radio-embolization in case of bleeding, or radiologicallyguided punction in cases of intra-abdominal collections.
Hospital length stay was increased after PG (23.6±3.5 days vs. 16.5±1.9 days, p=0.071).
Pancreatic exocrine insufficiency was more frequent after PJ (3.8% vs. 19.2%%, p=0.134).
Pancreatic endocrine insufficiency incidence was similar between the two groups (7.7% vs. 9.4%%, p=0.575). Two cases of endocrine pancreatic insufficiency after PJ were worse in preexistent diabetes.
DISCUSSION
This study confirmed the previous results showing a significant decrease of POPF incidence in CP performed with a PJ. POPF rate was more than twice as high in the PG group as in the PJ group. We also displayed a significant reduction of POPF severity with PJ.
CP allows healthy parenchyma sparing in benign pancreatic isthmus or low-grade malignancy tumor resection.
CP is a known as a safe procedure despite a high postoperative morbidity rate, mainly due to a high POPF incidence. Moreover, POPF was the most frequent shortterm complication after CP (40.9%) in a recent review [14].
Nearly half of these fistulas were severe fistulas (grade B and/or C). CP should be reserved for selected patients who are able to sustain severe postoperative complications, and who would benefit from long-term endocrine and exocrine function preservation [4]. The main challenge in CP, in order to decrease the severity of postoperative outcomes, is to decrease POPF rate.
The most commonly identified risk factors of POPF are a soft fatty non-calcified non-fibrotic pancreas, and a main pancreatic duct diameter of less than or equal to 3 mm [15]. Other associated risk factors are generally missing in patients who underwent CP: reoperation, emergency surgery, jaundice, kidney failure, cirrhosis, cardiovascular disease, and malnutrition.
Although PJ seems to be the most common way to perform pancreatico-enteric anastomosis after CP, PG were more frequent in the largest series [4, 14, 16, 17]. Some of these studies concerning mainly PG reported very low POPF rates but did not routinely place intraoperative drains or check amylase levels, leading to an underestimation of POPF rate [16, 17]. We report POPF rates of a 76.9% and 37.5% after PG and PJ, testing for POPF with systematic drainage and amylase assay. These results are consistent with the studies of Goudard et al. and Crippa et al. who respectively focused on PG and PJ after CP, and assessed POPF incidence to be 65% after PG and 44% after PJ [4, 18].
The Influence of pancreatico-enteric reconstruction has been extensively studied in PD. Although the superiority of one of the two techniques is still under debate, recent controlled studies and meta-analyses advocate the use of PG in order to decrease POPF rate [7, 8, 19, 20]. The first argument for the benefit of PG is that acidity and lack of enterokinases in the gastric lumen should prevent pancreatic enzymes from being activated; avoiding local deleterious effects on anastomotic tissues. Secondly, the rich blood supply in the stomach wall compared to jejunal wall promotes anastomotic healing. Finally, use of upper endoscopy could help to assess PG avoiding more invasive exploration. PJ is technically more demanding and requires additional time to fix a Roux-en-Y jejunal loop. However, in our experience we did not observe an increase in operative time when performing PJ.
We argue that PJ allows decreased tension on pancreatico-enteric anastomosis, even if anatomical proximity of the stomach would suggest the opposite. Moreover, it would allow to keep the distal pancreatic remnant away from the splenic vessels, and to avoid severe postoperative bleeding.
Peri-pancreatic drainage did not allow us to determine whether the pancreatic stump or the pancreatico-enteric anastomosis was responsible for POPF occurrence. Right pancreatic stump is suspected to be involved in most POPF occurrences [4]. However, there was no difference in right pancreatic remnant closure when performing by either PG or PJ, leading us to impute our findings to the type of pancreatico-enteric anastomosis. Most severe POPF seem to occur from the distal remnant, making the choice of anastomosis all the more important to avoid severe consequences of anastomotic leakage [4].
We observed a significant decrease of POPF severity after PJ. Use of Clavien-Dindo classification in addition to ISGPF classification allowed us to highlight the most severe POPF among clinically relevant fistulas that required invasive management. Indeed, ISGPF classification assesses as grade C fistulas when either a surgical or a radiological management is needed [11]. Bleeding complications were responsible for the most severe outcomes, and often led to re-intervention. Radio-embolization was an alternative to surgical treatment in case of hemorrhage. There was no significant difference of postoperative hemorrhage between the two groups. In case of abdominal collection, radiologically guided puncture was preferentially used. It was associated with less severe clinical outcomes, and was noted as a grade C fistula, or grade 3 of Clavien-Dindo classification.
We reported one death in the PJ group, due to a massive pulmonary embolism on the first postoperative day. The main reported causes of death after CP was pancreaticoenteric anastomosis leakage, multiple organ failure, hemorrhage, and pulmonary embolism [3, 4, 14]. Although the deadly outcome in our series was unrelated to POPF, it still illustrates the potential severity of outcomes after CP.
The clinical relevance of both POPF incidence and severity reduction in PJ group results in a hospital length stay decrease. Although, this difference remained not significant, it still resulted in a one-week-long reduction of hospital length stay after PJ.
CP has been developed as a parenchyma and longterm function sparing technique in opposite to traditional extensive pancreatic surgery. Exocrine and endocrine failures occur in about 10% and 5% of the cases [14]. CP allows a significant reduction of endocrine insufficiency compared to distal pancreatectomy [14, 16, 18]. CP also showed a less pronounced effect on exocrine failure reduction [14, 18]. Long-term outcomes did not differ significantly from PJ and PG in this study. We still observed a higher exocrine failure incidence after PJ, which is similar to the trend reported by Iacono et al. [14]. On the contrary, PJ had been associated with reduction of exocrine failure after PD [21]. Pancreatico-enteric anastomosis seems to have no effect on postoperative endocrine function [22].
We report one of the largest series of patients managed with CP, comparing PJ with PG. However, our results need to be qualified by the heterogeneity of pancreatico-enteric reconstruction managements. Our study suffers from this bias because it is a retrospective study, including patients from four different centers. Thus, there was no prior standardization of the anastomosis technique.
Each surgeon had his own technical specificities to perform PJ or PG. Over the four University Hospitals participating in this study, two managed CP with only one technique of pancreatico-enteric anastomosis. Single plan anastomosis was the only reported technique, but type of wire and number of single sutures was left to the surgeon’s opinion. Use of another anastomosis technique, especially duct-to-mucosa or binding PJ or PG, or use of double omental flap, could have changed our results [23, 24].
We used routine peri-operative external drainage to allow us to test for POPF via systematic assays. Very few anastomoses were performed with internal main pancreatic duct stenting in one of the centers (either in PJ or PJ). The role of stenting is still debated. External stenting of pancreatico-enteric anastomosis seems to decrease POPF rate [25, 26]. Internal stenting did not result in a significant decrease of POPF incidence [25].
The possible preventive injection of somatostatin analogues should also be considered. Use of somatostatin analogues has been proved to reduce both POPF rate and complications, with no significant effect on mortality rate [27]. We did not use prophylactic somatostatine analogues in this study. Somatostatin analogues could be used in cases of proven POPF.
We conclude a lower risk of POPF and less severe complications with PJ in CP. These results need to be examined for long-term exocrine pancreatic function impairment after PJ. Significant decrease of POPF incidence and severity after PJ leads us to recommend PJ in CP rather than PG, especially in the oldest and frailest patients. Further prospective studies on CP, performed with a standardized technique, are necessary to confirm our results.
Aknowledgments
The authors thank Lucie Planche for her fantastic help to complete the statistical analysis.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Bassi C. Middle segment pancreatectomy: a useful tool in the management of pancreatic neoplasms. J Gastrointest Surg 2007; 11:421–424. [PMID: 17436124]
- Sperti C, Beltrame V, Milanetto AC, Moro M, Pedrazzoli S. Parenchyma-sparing pancreatectomies for benign or border-line tumors of the pancreas. World J Gastrointest Oncol 2010; 2:272–281. [PMID: 21160640]
- Sauvanet A, Partensky C, Sastre B, Gigot JF, Fagniez PL, Tuech JJ, Millat B, et al. Medial pancreatectomy: a multi-institutional retrospective study of 53 patients by the French Pancreas Club. Surgery 2002; 132:836–843. [PMID: 12464868]
- Goudard Y, Gaujoux S, Dokmak S, Cros J, Couvelard A, Palazzo M, Ronot M, et al. Reappraisal of central pancreatectomy: A 12-year singlecenter experience. JAMA Surg 2014; 149:356. [PMID: 24740703]
- Fernández-Cruz L, Belli A, Acosta M, Chavarria EJ, Adelsdorfer W, López-Boado MA, Ferrer J. Which is the best technique for pancreaticoenteric reconstruction after pancreaticoduodenectomy? A critical analysis. Surg Today 2011; 41:761–766. [PMID: 21626319]
- Wente MN, Shrikhande SV, Müller MW, Diener MK, Seiler CM, Friess H, Büchler MW. Pancreaticojejunostomy versus pancreaticogastrostomy: systematic review and meta-analysis. Am J Surg 2007; 193:171–183. [PMID: 17236843]
- He T, Zhao Y, Chen Q, Wang X, Lin H, Han W. Pancreaticojejunostomy versus pancreaticogastrostomy after pancreaticoduodenectomy: A systematic review and meta-analysis. Dig Surg 2013; 30:56–69. [PMID: 23689124]
- Clerveus M, Morandeira-Rivas A, Picazo-Yeste J, Moreno-Sanz C. Pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy: A systematic review and meta-analysis of randomized controlled trials. J Gastrointest Surg 2014; 18:1693–1704. [PMID: 24903847]
- Venara A, de Franco V, Mucci S, Frampas E, Lermite E, Regenet N, Hamy A. Central pancreatectomy: comparison of results according to the type of anastomosis. J Visc Surg 2012; 149:e153–158. [PMID: 22317930]
- Sastre B, Ouaissi M, Pirro N, Chaix JB, Sielezneff I. Medial pancreatectomy. J Chir (Paris) 2009; 146:175–178. [PMID: 19584007]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8–13. [PMID: 16003309]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205–213. [PMID: 15273542]
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, et al. Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007; 142:761–768. [PMID: 17981197]
- Iacono C, Verlato G, Ruzzenente A, Campagnaro T, Bacchelli C, Valdegamberi A, Bortolasi L, et al. Systematic review of central pancreatectomy and meta-analysis of central versus distal pancreatectomy. Br J Surg 2013; 100:873–885. [PMID: 23640664]
- Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol WJG 2005; 11:2456–2461. [PMID: 15832417]
- DiNorcia J, Ahmed L, Lee MK, Reavey PL, Yakaitis EA, Lee JA, Schrope BA, et al. Better preservation of endocrine function after central versus distal pancreatectomy for mid-gland lesions. Surgery 2010; 148:1247–1254. [PMID: 21134558]
- Adham M, Giunippero A, Hervieu V, Courbière M, Partensky C. Central pancreatectomy: single-center experience of 50 cases. Arch Surg Chic 2008; 143:175–180. [PMID: 18283143]
- Crippa S, Bassi C, Warshaw AL, Falconi M, Partelli S, Thayer SP, Pederzoli P, et al. Middle pancreatectomy: indications, short- and longterm operative outcomes. Ann Surg 2007; 246:69–76. [PMID: 17592293]
- Topal B, Fieuws S, Aerts R, Weerts J, Feryn T, Roeyen G, Bertrand C, et al. Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction after pancreaticoduodenectomy for pancreatic or periampullary tumours: a multicentre randomised trial. Lancet Oncol 2013; 14:655–662. [PMID: 23643139]
- Xiong JJ, Tan CL, Szatmary P, Huang W, Ke NW, Hu WM, Nunes QM, et al. Meta-analysis of pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy. Br J Surg 2014; 101:1196–1208. [PMID: 25042895]
- Rault A, SaCunha A, Klopfenstein D, Larroudé D, Epoy FN, Collet D, Masson B, et al. Pancreaticojejunal anastomosis is preferable to pancreaticogastrostomy after pancreaticoduodenectomy for longterm outcomes of pancreatic exocrine function. J Am Coll Surg 2005; 201:239–244. [PMID: 16038822]
- Ishikawa O, Ohigashi H, Eguchi H, Yokoyama S, Yamada T, Takachi K, Miyashiro I, et al. Long-term follow-up of glucose tolerance function after pancreaticoduodenectomy: comparison between pancreaticogastrostomy and pancreaticojejunostomy. Surgery 2004; 136:617–623. [PMID: 15349110]
- Rosso E, Lopez P, Roedlisch MN, Narita M, Oussoultzoglou E, Bachellier P. Double omental flap reduced perianastomotic collections and relaparotomy rates after pancreaticoduodenectomy with pancreaticogastrostomy. World J Surg 2012; 36:1672–1678. [PMID: 22411089]
- Hashimoto D, Chikamoto A, Ohmuraya M, Hirota M, Baba H. Pancreaticodigestive anastomosis and the postoperative management strategies to prevent postoperative pancreatic fistula formation after pancreaticoduodenectomy. Surg Today 2013. [PMID: 23842691]
- Dong Z, Xu J, Wang Z, Petrov MS. Stents for the prevention of pancreatic fistula following pancreaticoduodenectomy. Cochrane Database Syst Rev 2013. [PMID: 27153248]
- Motoi F, Egawa S, Rikiyama T, Katayose Y, Unno M. Randomized clinical trial of external stent drainage of the pancreatic duct to reduce postoperative pancreatic fistula after pancreaticojejunostomy. Br J Surg 2012; 99:524–531. [PMID: 22497024]
- Gurusamy KS, Koti R, Fusai G, Davidson BR. Somatostatin analogues for pancreatic surgery. Cochrane Database Syst Rev 2013. [PMID: 23633353]


