Keywords
Children; Cerebral palsy; Caries prevalence; Oral health
Introduction
Special health care refers to “any physical, developmental, mental, sensory, behavioural, cognitive, or emotional impairment or limiting condition that requires medical management, health care intervention, and/or use of specialized services or programs”. The condition may be congenital, developmental, or acquired through disease, trauma, or an environmental cause and may impose limitations on performing daily self-maintenance activities or cause substantial limitations in a major life activity [1].
Cerebral palsy (CP) describes a group of permanent disorders of the development of movement and posture, causing activity limitation, attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, perception, cognition, communication, behaviour, epilepsy and secondary musculoskeletal problems [2].
The etiology and pathogenesis of cerebral palsy are still not clearly understood, lesion originating from brain injury occurs during the prenatal 80%, prenatal or postnatal period are suggested. The diagnosis is based mainly on clinical symptoms [3-5].
Cerebral palsy is classified according to severity into mild, moderate and severe, and according to the involved area of the body into monoplegic (one limb), hemiplegic (one side of the body), paraplegic (both legs), quadriplegic (all limbs equally) and diplagic (legs and arms) and it rare. Cerebral palsy also has several manifestations; intellectual disability, seizure disorders, sensory impairment, speech problems – usually dysarthia – and joint contractions due to spasticity and rigidity leading to abnormal limb posture [6,7].
Children with cerebral palsy have motor dysfunction, so normal functioning of the orofacial muscles is disturbed. Depending on the severity of the disease, individuals with CP may suffer from choking, coughing, drooling, inability to consume solid food, and difficulties in swallowing, chewing and drinking. Consequently, oral health is a significant challenge, as individuals with CP are more prone to developing caries and periodontal disease, mouth-breathers and suffer from malocclusion, skeletal class II and anterior open bite. No intraoral anomalies are unique to persons with cerebral palsy but oral conditions are more severe than the general population [3,6,7].
In 1960, McDonald discussed how pediatric medicine had changed in the previous 30 years from 90% treatment and 10% prevention to just the reverse [7]. Preventive dentistry is now the foundation on which all oral health care is built; which is depend mainly on home oral hygiene. Hence, parents with good oral health knowledge play a better role in maintaining optimal oral health for their children with CP through supervising oral hygiene and dietary habits [8].
Overall CP prevalence for the past 40 years is stable, but a modest increase in prevalence probably occurred in the last decades of the twentieth century. This increase in prevalence can be attributed to the substantial increase in the prevalence of CP per 1000 very low birth weight infants, this due to increased survival that results from new-born intensive care [9]. prevalence in children weight 1000 to 1499 g at birth was 59.18 per 1000 live births, and prevalence of CP by gestation age; before 28 weeks gestation was 111.80 per 1000 live births [10].
The estimated prevalence of cerebral palsy worldwide ranges from 0.74 to 3.6 per 1000 live births [11]. In Nigeria, the incidence was 13.1 children per year [12].
Dental caries is an infectious and communicable disease defined as localized destruction of susceptible dental hard tissues by acidic by products from bacterial fermentation of dietary carbohydrates, it is a dynamic process of demineralization and remineralization of enamel depending on salivary PH [13]. It is the most common chronic disease among children and adolescents [7].
The aims of this study were to assess the carious status and evaluate parent’s oral health knowledge of children with cerebral palsy as a response to the recent increase noted in the number children with CP seeking dental care in the pediatric clinic at the faculty of Dentistry, University of Khartoum, in order to establish a proper interceptive and preventive oral health program and improve their quality of life. To the best of our knowledge, there is no such study in Sudan.
Materials and Methods
A cross sectional hospital based study carried out at Jaafer Ibn Ouf Pediatric Teaching Hospital, Neurology Unit, Khartoum Sudan.
The inclusion criteria for the selection were; Sudanese children diagnosed from medical records as cerebral Palsy, attending Jaafer Ibn Ouf Hospital and parents or relatives of CP children attending the Hospital. Whereas, the other children; with neurological defects other than cerebral palsy, CP children with severe disabilities and uncooperative CP children were excluded from the study.
A total of 123 children aged 2 to 15 years old with a confirmed diagnosis of cerebral palsy from their medical records were included in the study. Parents’ consent was first obtained, and then face to face interviews were conducted to collect personal data and information on the knowledge, attitude and practice of the parents in the doctor’s office on the day of the referral clinic.
The parents’ oral health knowledge, attitude and practice was measured using a modified KAP questionnaire [14]. The questionnaire was designed in English, translated into Arabic and back into English. It consisted of two parts: the first for general information such as name, age, gender of the child, and the caregiver’s age and education. The second part consisted of 17 closed end questions related to knowledge, attitude and practice.
Clinical examination was conducted by the main investigator. Examination was carried out in the doctor’s office under artificial lighting, with the child sitting in an up-right position in an ordinary chair or in the child’s wheelchair placed in front of examiner, using sterilized gloves and an examination set. Caries was measured using the dmft/DMFT index for primary and permanent teeth, respectively, according to WHO criteria [15].
Ethical clearance was obtained from the research committee at the Faculty of Dentistry, University of Khartoum, and from the Khartoum State Ministry of Health Research Directorate. The research’s purpose and objectives were explained to the parents in clear simple words, and signed informed consent was obtained from the parents before starting the oral examination.
Participants had the right to withdraw at any time, as well as the right to benefit, no harm, right to privacy and confidentiality.
Patients who were found to need treatment were referred by the researcher to the University of Khartoum, Faculty of Dentistry to receive dental treatment. Parents were educated by the researcher on oral health and given instructions about the oral care of their child.
After three weeks of starting the clinical examination 10% of the sample (n=13) were re-examined for reliability, the kappa value was 0.68, 0.74 for dmft and DMFT respectively.
Statistical Analysis
A descriptive statistic in terms of frequency distribution tables; mean, standard deviation and histogram were utilized for quantitative variables.
Chi square test was applied to examine the association between categorical variables like education and hearing about fluoride, association between knowledge, attitudes and practice with caries in primary and permanent.
Analysis of Variance (ANOVA) was applied to test significant difference between age groups in dmft and DMFT.
The independent sample t-test was utilized to test if their significant difference between boys and girls in dmft and DMFT.
For all test P-value<0.05 is considered significant.
Results
A total of 123 children with cerebral palsy were included in this study, 78 boys and 45 girls. The age ranged from 2-15 years old and the mean age was 6.58 years. The majority (n=71) of children where aged 2-6. The percentage of age decrease with increase in age (Table 1).
Age
(Yrs) |
Gender |
Total |
| Boys |
Girls |
| 2 – 6 |
47 (66.2%) |
24 (33.8%) |
71 (100.0%) |
| 7 – 11 |
22 (62.9%) |
13 (37.1%) |
35 (100.0%) |
| 12 – 15 |
9 (52.9%) |
8 (47.1%) |
17 (100.0%) |
| Total |
78 (63.4%) |
45 (36.6%) |
123(100.0%) |
Table 1: Age groups of children with cerebral palsy by gender.
The majority of the parents were mothers aged 21 to 82 years old. Most parents had a secondary education (n=50) 40.7% (Table 2).
| Education |
Child Care |
Total |
| Mother |
Father |
Relatives |
| Illiterate |
13 (11.7%) |
1 (20.0%) |
4 (57.1%) |
18(14.6%) |
| Basic |
26 (23.4%) |
1 (20.0%) |
1 (14.3%) |
28(22.8%) |
| Secondary |
48 (43.2%) |
2 (40.0%) |
0 (0.0%) |
50(40.7%) |
| University and above |
24 (21.6%) |
1 (20.0%) |
2 (28.6%) |
27(22.0%) |
| Total |
111(100.0%) |
5 (100.0%) |
7(100.0%) |
123(100.0%) |
Table 2: Education of caregivers of children with cerebral palsy.
The frequency distribution of Age by taking the mean and calculate the standard deviation showed in the above Figure 1.
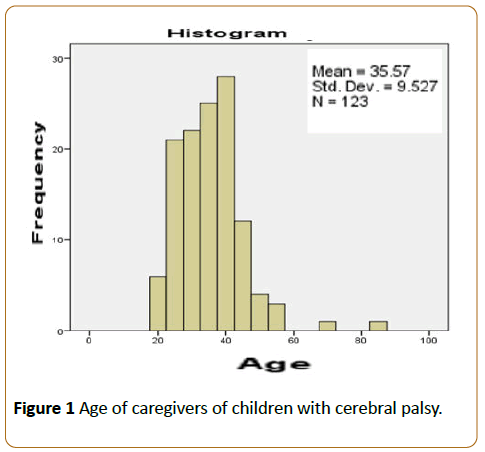
Figure 1: Age of caregivers of children with cerebral palsy.
In Table 3, Most children 87.8% brush their teeth and 80.5% of them brushed under supervision, while more than half 61.1% brushed once a day, 87.0% used manual tooth brush, Fewer used mouth wash 5.7%, 81.3%, of the children had never visited a dentist before, and of those who had visited a dentist (n=23) 10.6% within less than 12 months ago 8.1% more than 12 months. Almost these 95.7% had gone when there was a problem, and the main treatment they received was extraction and medications. The following are the answers of their parents mentioned in Table 3.
| Questions |
Answers |
Count (%) |
| Does your child brush his/ her teeth |
Yes |
108 (87.8%) |
| No |
15 (12.2%) |
| Don't know |
0 (0.0%) |
| If your child brush his/her teeth |
Brush alone |
20 (18.5%) |
| Brush under supervision |
88 (81.5%) |
| Other |
0 (0.0%) |
| Frequency of brushing |
Twice or more times per day |
41 (38.0%) |
| Once per day |
66 (61.1%) |
| Other |
1(.9%) |
| Type of tooth brush |
Manual |
94 (87.0%) |
| Electrical |
0 (0.0%) |
| Other |
14 (13.0%) |
| Use of mouth wash |
Yes |
7 (5.7%) |
| No |
116 (94.3%) |
| Does your child rinse themouth after eating or drinking |
Yes |
98 (79.7%) |
| No |
25 (20.3%) |
| Sometimes |
0 (0.0%) |
| Don't know |
0 (0.0%) |
| History of visiting dental clinic |
Never visited |
100 (81.3%) |
| Less than 12 months |
13 (10.6%) |
| More than 12 months |
10 (8.1%) |
| Other |
0 (0.0%) |
| What is your reason for last dental visit |
There is a problem |
22 (95.7%) |
| First dental visit |
1 (4.3%) |
| Recall appointment |
0 (0.0%) |
| Other |
0 (0.0%) |
| Type of treatment perceived |
Only medication |
1 (4.3%) |
| Fluoride application |
0 (0.0%) |
| Extraction |
9 (39.3%) |
| Periodontal scaling |
0 (0.0%) |
| Tooth filling |
0 (0.0%) |
| Pulp therapy |
2 (8.7%) |
| Another |
9 (39.1%) |
| Missing |
2 (8.7%) |
Table 3: Oral health practices of parents of children with cerebral palsy.
More than half the parents 60.2% had heard about fluoride. Less than half 46% said that fluoride prevented tooth decay (Table 4).
| Questions |
Answers |
Count (%) |
| Do you hear about fluoride |
Yes |
74 (60.2%) |
| No |
49 (39.8%) |
| What is role of the fluoride |
Prevent tooth decay |
46 (62.2%) |
| Has no role |
1 (1.4%) |
| I don't know |
18 (24.3%) |
| Give freshness |
9 (12.2%) |
| remove calculus |
0 (0.0%) |
| Does the tooth paste contain fluoride |
yes |
57 (77.0%) |
| No |
2 (2.7%) |
| Don’t Know |
15 (20.3) |
| Which of the following food items can cause tooth decay |
Chocolates |
52 (42.3%) |
| Bakery products |
3 (2.4%) |
| Soft drink |
6 (4.9%) |
| all of the above |
54 (43.9%) |
| I don't know |
8 (6.5%) |
| Total |
123 (100.0%) |
Table 4: Oral health knowledge of parents of children with cerebral palsy.
Regarding cariogenic food, 42.3% answered that chocolate cause’s tooth decay and 43.9% said that chocolate, bakery products and soft drinks cause tooth decay shown in above Table 4. A significant association found between parents’ educational level and hearing about fluoride (P=0.002) (Table 5).
| Education |
Do you hear about fluoride |
Total (count) |
| Yes (count) % |
No (count) % |
| Illiterate |
6 (33.3%) |
12 (66.7%) |
18 (100.0%) |
| Basic |
13 (46.4%) |
15 (53.6%) |
28 (100.0%) |
| Secondary |
32 (64.0%) |
18 (36.0%) |
50 (100.0%) |
University
and above |
23 (85.2%) |
4 (14.8%) |
27 (100.0%) |
| Total |
74 (60.2%) |
49 (39.8%) |
123(100.0) |
Chi square 14.97, p value=0.002
Table 5: Association between educational level and hearing about fluoride.
Table 6 shows that 80.2% of parents said that milk teeth don’t require good care. 40.7% said that the media was their main source of information about oral health. About half 50.4% responded that they can maintain good dental health in their children by supervising their tooth brushing, reducing sugary food intake and making regular visits to a dentist. 90% of parents responded that dental health is important.
| Questions |
Answers |
Count (%) |
| Milk teeth don’t require good care as they are going to fall away |
Yes |
97 (78.9%) |
| No |
16 (13.0%) |
| I don't know |
10 (8.16%) |
| Is good dental health important for optimum general health |
Yes |
111 (90.2%) |
| No |
5 (4.1%) |
| I don't know |
7 (5.7%) |
| What is your main source of oral health information |
Media |
50 (40.7%) |
| Dentist |
13 (10.6%) |
| No body |
26 (21.1%) |
| another |
34 (27.6%) |
| In your opinion how can you maintain good dentalhealth of your child |
Reducing sugar |
30 (24.4%) |
| By supervising and helping in tooth brushing |
26 (21.1%) |
| By visiting dentist |
4 (3.3%) |
| All of the above |
62 (50.4%) |
| I don’t know |
1 (.8%) |
| Total |
123 (100.0%) |
Table 6: Oral health attitude of parents of children with cerebral palsy.
The total mean DMFT score was 3.6 ± 4, the highest mean DMFT being 6.3 ± 10.1 in the age group of 12-15 years old showed in Table 7. No significant association between either DMFT or different age groups (p-value=0.171) or DMFT and gender (P=0.924).
Age group
(Yrs.) |
Mean DMFT±SD |
Total |
| Boys (n=70) |
Girls (n=38) |
| 2 – 6 |
3.4±5.0 |
2.7±3.4 |
3.18±4.55 |
| 7 – 11 |
3.9±3.6 |
5.5 + 5.4 |
4.45±4.37 |
| 12 – 15 |
2.0±2.0 |
6.3±10.1 |
4.17±6.90 |
| Total |
3.14±4.44 |
3.22±4.63 |
3.6±4.64 |
P-value for gender=0.924; P-value for age=0.171
Table 7: Mean DMFT of children with cerebral palsy according to gender and age.
Age group
(Yrs.) |
Decayed
Count (%) |
Missed
Count (%) |
Filled
Count (%) |
| 2-6(n=71) |
36 (50.7%) |
6 (8.5%) |
1 (1.4%) |
| 7-11(n=35) |
22 (71.0%) |
7 (22.6%) |
0 (0.0%) |
| 12-15(n=17) |
4 (66.7%) |
0 (0.0%) |
0 (0.0%) |
| Total |
62 (57.4%) |
13 (12.0%) |
1 (0.9%) |
Table 8: Decayed missed and filled primary teeth by age group.
The most common component of DMFT (Decayed, Missing or Filled Teeth) in primary teeth was decayed and missed teeth; 57.4% and 12.0%, respectively. The filled teeth were very little 0.9% (Table 8).
Table 9 shows the total mean DMFT was 3.41 ± 3.0. A significant association between the age group and DMFT, but no significant association between gender and DMFT. The range of age group 2 to 15 years.
Age group
(Yrs.) |
Mean DMFT±SD |
Total |
| Boys (n=33) |
Girls (n=21) |
| 2 – 6 |
0±0 |
0±0 |
0±0 |
| 7 – 11 |
1.68±2.98 |
1.18±2.40 |
1.52±2.77 |
| 12 – 15 |
4.89±2.76 |
1.75±2.43 |
3.41±3.0 |
| Total |
1.04±2.39 |
10.6±1.67 |
2.0±2.90 |
P-value for age=0.000 P-value for gender=0.280
Table 9: Mean DMFT according to gender and age group.
In Table 10, the total percentage of decayed permanent teeth was 46.3%, missing were 13.0% and there were no filled teeth (Table 10). There was significant association between knowledge level and DMFT in permanent teeth (p=0.037) (Figure 2).
| Age group (Yrs.) |
Decayed Count (%) |
Missed Count (%) |
Filled Count (%) |
| 2-6 (n=71) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| 7-11 (n=71) |
12 (36.4%) |
3(9.1%) |
0 (0.0%) |
| 12-15 (n=17) |
13 (76.5%) |
4 (23.5%) |
0 (0.0%) |
| Total |
25 (46.3%) |
7 (13.0%) |
0 (0.0%) |
Table 10: Percentage of decayed, missed and filled permanent teeth by age group.
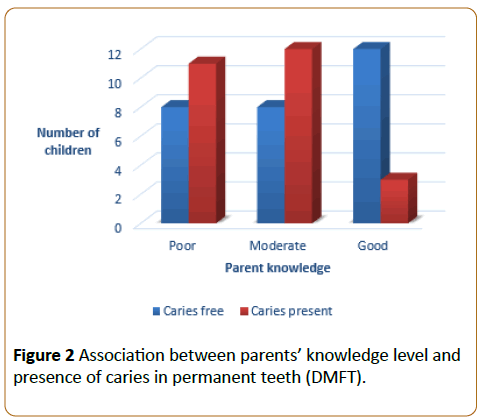
Figure 2: Association between parents’ knowledge level and presence of caries in permanent teeth (DMFT).
Discussion
This hospital-based cross-sectional study was conducted in order to assess the knowledge attitudes and practices of the parents of Sudanese children with cerebral palsy towards oral health, as well as dental caries in these children. The study was conducted among children attending Jaafer Ibn Ouf Pediatric Teaching Hospital in Khartoum, which is the only specialty paediatric teaching hospital in Sudan. The hospital receives all cases referred from different parts of the Sudan, and has many departments including the Neurology unit where this study was conducted.
This study assists in designing effective oral health educational programs for the parents of children with CP in order to improve oral health education/prevention programs, consequently resulting in better dental health for these children.
The response rate among respondents in this study was 100% (123 out of 123). Similar to previous study, the gender distribution of the children included in this study showed a high male to female ratio [16].
The most interesting finding in this study was that majority of children 81.3% never visited dentist before. This is in line with study done in Saudi Arabia in group of CP children [17], as well as other study [18]. Of those who had visited dentist half had gone only when there was a problem like study done in Saudi in disabled children [19] and another study in Scotland [18]. The main treatment received was extraction and medication. None of the children had received prevention treatment like fluoride.
Priorities and attitudes can serve as obstacles to oral care. Parental and physician lack of awareness and knowledge may hinder an individual with CP from seeking preventive dental care. Other health conditions may seem more important than dental health, especially when the relationship between oral health and general health is not well understood [20]. The AAPD guidelines recommend making a consultation dental visit within six months or of the first tooth eruption. This should be strictly followed in children with CP [20].
In terms of knowledge about fluoride and factors causing tooth decay, more than half of the parents 60.2% heard about fluoride which was less than reported by Dana Al-Bader et al. of Saudi Disabled children they found that 92.7% of parents had heard about fluoride [19]. Less than half 46% of the parents said that fluoride prevent tooth decay. As for cariogenic food 42.3% stated that chocolate causes tooth decay, this show that the mothers were aware that sugary item likes chocolates can lead to dental caries. However, there was low awareness about the different forms of sugary items, which are harmful to the teeth. This throws the light on inadequate knowledge about the relationship between the different forms of sugar consumption and dental caries and less than half 43.9% said that (chocolate, bakery products and soft drinks) cause tooth decay this showing an overall low knowledge regarding different cariogenic food items like study in normal children by Romi Jain [14].
A great number of parents thought that good dental health was important for optimum general health which in line with studies done by Amjad in Saudia [21] and Jyoti Magoo et al. in group of Autistic children [22]. Of parents who supervised teeth brushing of their children 80.5% like study done in Brazil [16] and same as study done in group of disabled children in Saudi Arabia [19] because they are partial or total reliance on the caregiver to perform daily activities, such as feeding, mobility and general and oral hygiene.
Parents should be aware that, without their supervised to oral hygiene procedures in their children with cerebral palsy they can have serious dental consequences. Dental home cane reduces the child’s risk of preventable dental/oral disease.
More than half 61.1% brush their teeth once per day like [22] which was opposite with study by Oredugba [23] and by Ferreira and their colleagues in Brazil [24]. These children will benefit from assistive devices such as electric toothbrushes and toothbrushes with large or modifying handles in this study 87.0% used manual tooth brushes for their children like [22].
Only 16 respondents 13.0% said they knew the important of the milk teeth the remaining stated that milk teeth do not require care, it fall down, which was fewer than result of Autistic children in which 71.2% of parents felts important of milk teeth [22].
Half of the responded said that they can maintain a good dental health in their children by supervising their tooth brushing, reducing sugary food intake and making regular visits to a dentist; a finding less than that reported by two study done in Saudi Arabia [19,21].
Parents or caregiver are responsible for establishing good oral hygiene at home. So dental education of parents/ caregivers is important to ensure children with CP do not jeopardize their overall health by neglecting their oral health this education mainly by dentist and mass media; newspapers, radio, television, and internet.
In our study, main source of oral health information from media like study done in normal children in India [14] this show that media influence people in their live and fewer from dentist this show that we need to incorporate oral health education in our daily clinic.
AAPD done guidelines on management of dental patients with special health care needs [20] and this should apply to Sudanese cerebral palsy children.
Caries prevalence in children with CP
The total mean dmft and DMFT in the present study was found to be 3.6 ± 4.64 and 2.0 ± 2.90 respectively. No significant association between dmft/DMFT and gender, contrary to findings reported by Nouf Al-Hammad et al. [25] and Maria Teresa et al. [26] there was significant association between DMFT and different age group (P-value=0.000); a finding similar like study by Ana Carolina et al. [16] they mentioned that these may be attributed to the fact that children with CP may experience delays in the chronology of tooth eruptions due to nutritional reasons as studied by Pope and Curzon [18].
Studies conducted in Arab countries showed higher caries indices, United Arab Emirates (UAE), [27] and in Saudi Arabia [25].
The dental caries experience in this study was found to be high, similar to results to global studies done in Brazil, [28-30] New York and China, Nigeria and South Africa respectively [31,32], a recent study done in Albania show high prevalence of caries. The mean deft and DMFT index was 3.4 ± 3.5 and 4.9 ± 4.6, respectively [33].
Some studies found no difference in the caries index between normal children and children with CP [17,18] and study done in adults by Miriam in 2008 [34].
Contrary to our findings, Nelsen in case control study in Denmark showed that the caries rate of the CP-group was significantly lower than that of control group [35] a study in Brazil, the author mentioned that the children evaluated were not representative to all children with CP, but only of those who look for treatment in a reference center and they may possess better oral health due to enhanced parental attention and/or fewer difficulties in controlling oral conditions [36].
The prevalence of dental caries in children with CP was, as expected very high. Risk factors such as present of infantile reflexes (rooting, suckle-swallow, biting and gagging) would explain this [37], as well as side effects of drugs and recurrent hospitalization [38], high salivary osmolality [39], soft diet intake [40], high frequency of carbohydrate intake, autocleaning inability; all this factor contributing to difficulty in maintaining adequate oral hygiene.
The association of dental caries with the caregiver’s educational level approves the statement that the caregiver’s low educational level increases the probability of dental caries [28] this is clarifying by Caregivers with high educational level have better health knowledge and positive attitudes towards oral health [41].
The most common components of DMFT in primary and permanent teeth was decayed teeth 57.4%, 46.3% respectively, similar to study done by Oredugba [23] and [19,20,42] missing component in primary and permanent teeth was 12.0%, 13.0% respectively and there was fewer filled teeth, this show that there is sever unmet preventive and restorative dental treatment needs and this was mentioned in literatures [43].
It is an unhappy fact of life that oral health care comes far down in the list of priorities where parents of CP children are concerned. This is possibly due to the fact the cerebral palsy condition itself is of major concern and oral health care is forgotten. Thus, the results of the present study draw attention to a portion of the population that requires special care regarding their oral health through treatment and orientation this preventing possible harm and complication and avoiding local, systemic, psychological and social complications stemming from inadequate oral health. Considering the previously mentioned carries risks, unmet dental treatment need and barriers to access to dental services in the CP individuals therefor there is a need for public oral health programs with multidisciplinary services for this population as well as for all individuals with disabilities.
Conclusion
Parents' knowledge of oral health was satisfactory in most areas. lack of knowledge about the oral health of their Cerebral Palsy children.
The most interesting finding was that most of the cerebral palsy children never visited the dentist Those who’s visited dentist half of them gone when there is a problem.
A great number of parents know the important of good dental health to optimum general health. The main source of oral health information from media minimal from dentist.
Cerebral palsy children had high caries prevalence and more prevalence of decayed teeth than other component of decayed, missing and fill teeth.
Recommendations
Children with cerebral palsy are at risk of dental caries and gingival diseases due to dietary factors, poor oral hygiene, lack of parental knowledge regarding oral hygiene and problems related to dental management (involuntary movement and lack of cooperation). Therefore, continuous dietary supervision and assistance in maintaining good oral hygiene are obligatory because these children are partially or totally reliant on their caregivers to perform daily activities [4].
References
- American Academy of Pediatric Dentistry (2012) Reference Manual Overview: Definition and scope of pediatric dentistry. Pediatr Dent. 34:2.
- Bax MGM, Rosebaum P, Leviton A, Paneth, Dan B, et al. (2006) Definition and classification of cerebral palsy. Dev Med Child Neurol. 47: 571–576.
- Al-Allaq T, DeBord TK, Liu H, Wang Y, Messadi DV (2015)Oral health status of individuals with cerebral palsy at a nationally recognized rehabilitation center. Spec Care Dentist. 35:15-21.
- Miamoto CB, Ramos-Jorge ML, Ferreira MC, Oliveira MD, Vieira-Andrade RG, et al.(2011) Dental trauma in individuals with severe cerebral palsy: Prevalence and associated factors. Braz Oral Res. 25: 319-323.
- Krigger KW (2006) Cerebral palsy: An overview. Am Fam Physician. 73: 91-100.
- Chu CH, Lo EC (2010) Oral health status of Chinese teenagers with cerebral palsy. Community Dent Health 27: 222-226.
- Weddel JAB, Jones J (2011) Dental problems of children with, disabilities. In: McDonald R AD, Dean J(eds). Dentistry Child Adol 476-477.
- Wyne AH (2007) Oral health knowledge in parents of Saudi cerebral palsy children. Neurosciences. 12: 306-311.
- WeskisonSk (2006)The descriptive epidemiology of cerebral palsy. ClinPerinatol. 33:251-267.
- OskouiMFC, Dykeman J, Jett N, Pringsheim T (2013) An update on the prevalence of cerebral palsy: A systematic review and meta-analysis. Dev Med Child Neurol 55: 509-519.
- Chang MJ (2015) Estimating the prevalence of fcerebral palsy in Taiwan: A comparison of different case definitions. Res DevDisabil 36:207–212.
- Tinuade O, Mojisola O, Olusoga O, AdebiyiP (2008) Socio-clinical issues in cerebral palsy in Sagamu, Nigeria. SAJCH. 2: 120-124.
- Skeie SM WL, Poulsen S (2009) Dental caries in children and adolescents In: Koch G, Poulsen S, (eds). Pediatricdentistry: A clinical approach (2ndedn) Copenhagen: Blackwell Publishing, USA. p. 61-68.
- Jain R, Oswal KC, Chitguppi R (2014) Knowledge, attitude and practices of mothers toward their children’s oral health: A questionnaire survey among sub-population in Mumbai (India). J Dent Res Sci Develop. 1: 40-45
- World Oral Health Orgaization (1997) Oral Health Survey Basic Method (4th edn). Geneva. 25-29.
- Carolina A, Oliveira Lemos CR, Katz T (2012)Oral health conditionsand access to dental treatment in patients with cerebral palsy treated at the reference centre in Northeastern Brazil Rev Cefac, 14:861-870.
- SumayaN, Maryam ASM, El-AshiryEA (2014) Oral health in children with cerebral palsy. OHDM. 134: 1067-1075.
- Pope JE, Curzon ME (1991) The dental status of cerebral palsied children. PediatrDent. 13: 156-162.
- Dana AL, Bader LAA, Wyne AH, ChohanAN (2006) Oral health knowledegeand sources of information in parents of Saudi disabled children. Pakistan Oral & Dent Jr. 26:101-108.
- American Academy of Pediatric Dentistry (AAPD) (2012) Guidelines on management of dental patients with special health care needs. 376: 166-171.
- Wyne AH (2007) Oral health knowledge in parents of Saudi cerebral palsy children. Neurosciences. 124: 306-311.
- Magoo J, Shetty AK, Chandra P, Anandkrishna L, Kamath PS, et al.(2015) Knowledge, attitude and practice towards oral health care among parents of autism spectrum disorder children J AdvClin Res Insights 22: 82–86.
- Oredugba FA (2011) Comparative oral health of children and adolescents with cerebral palsy and controls. J Disabil and Oral Health. 12: 81-87.
- Ferreira De-Camargo MA, Frias AC, Antunes JL (2011) The incidence of dental caries in children and adolescents who have cerebral palsy and are participating in a dental program in Brazil. Special care in dentistry: Official publication of the American Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry. 31: 210-5.
- Nouf S. Al-Hammad AHW (2015) Caries experience and oral hygiene status of cerebral palsy children in Riyadh. OST - TDJ. 31: 860-64.
- Teresa M, Rodrigues B, Santos D, Masiero D, Novo NF, et al.(2003) Oral conditions in children with cerebral palsy. J Dentistry Child. 70: 40-6.
- Allouch M,JaT (2014) Dentofacialabnormalities and oral health status in children with cerebral palsy. J Interdiscipl Med Dent Sci. 3:2-6.
- Andreia MR, Cardoso EA (2015) Dental caries and periodontal disease in Brazilian children and adolescents with cerebral palsy. Int J Environ Res Public Health 121: 335-53.
- Rodrigues Dos-Santos MTB, Bianccardi M, Celiberti P, De-Oliveira Guaré R (2009) Dental caries in cerebral palsied individuals and their caregivers’ quality of life. Child Care, Health and Dev35: 475–81.
- Guerreiro PO, Garcias-Gde L (2009) Oral health conditions diagnostic in cerebral palsy in individuals of Pelotas, Rio Grande do Sul State, Brazil. Ciencia&SaudeColetiva. 14: 1939-1946.
- Rennan YD (2010) Oral health in pre shool children with and without cerebral palsy.Int J Paediatr Dent20: 330-335.
- Nqcobo BC (2012) Caries prevalence of children attending special need school in Johannesburg, Gauteng Province, University of, Johannesburg, South Africa.
- GaceE (2014) Oral health status of children with disability living in Albania. Mater Sociomed 26: 392-394.
- Mamaghani SM, Bode H, Ehmer U (2008) Orofacialfindings in conjunction with infantile cerebral paralysis in adults of two different age groups–Across-sectional study. J OrofacOrthop/Fortschritte der Kieferorthopädie. 69:240-256.
- Nielsen LA (1989) Caries among children with cerebral palsy: Relation to CP-diagnosis, mental and motor handicap. ASDC J Dent Child. 57: 267-273.
- Roberto LL, Machado MG, Resende VL, Castilho LS, Abreu MH (2012) Factors associated with dental caries in the primary dentition of children with cerebral palsy.Braz Oral Res. 26: 471–477.
- Dos Santos MT, Nogueira ML (2005) Infantile reflexes and their effects on dental caries and oral hygiene in cerebral palsy individuals. J Oral Rehabil 32: 880-885.
- Pomarico L, Souza IP, Tura LR (2005) Weakened medicines and hospitalization caries risk factors in children with and without special needs. Eur J Paediatr Dent. 6: 197.
- Santos MT, Ferreira MC, Mendes FM, Oliveira Guaré R (2014) Assessing salivary osmolality as a caries risk indicator in cerebral palsy children. Int J Paediatr Dent. 24: 84-89.
- Santos MT, Guare RO, Celiberti P, Siqueira WL (2009) Caries experience in individuals with cerebral palsy in relation to oromotor dysfunction and dietary consistency. Spec Care Dentist 29: 198-203.
- Saied-Moallemi Z, Virtanen JI, Ghofranipour F, Murtomaa H (2008) Influence of mothers’ oral health knowledge and attitudes on their children’s dental health. Eur Arch Paediatr Dent. 9: 79-83.
- De-Camargo MA, Antunes JL (2008) Untreated dental caries in children with cerebral palsy in the Brazilian context. Int J Paediatr Dent 18: 131-138.
- Ajami BA, Shabzendedar M, Rezay YA, Asgary M (2007) Dental treatment needs of children with disabilities. J Dent Res Dent Clin Dent Prospects 1: 93.

