Key words
Eating disorders; Medical history; Prevalence; Culture; Guideline
Text
Anorexia nervosa (AN) is an important cause of physical and psychosocial morbidity in adolescent and young female [1]. Patients with AN evaluate their shape and weight exaggeratedly and have a pathological fear of its increase [2]. A sustained and determined pursuit of weight loss consequently has developed starvation and psychiatric deviation including body image distortion or comorbidity [1, 2]. This has been one of the serious problems on mental health in Westernized societies [1, 2].
Recently, Pike et al. [3] reported a comprehensive review about the emergence of eating disorders (ED) in Asia, and emphasized an understanding of the diversity and distinctiveness of the individual countries and cultures. Additionally, they suggested that ED were not culture-bound or culture-specific, but rather culture-reactive. Pike et al. [4] also summarized the rise in ED in Japan and concluded that increasing industrialization, urbanization, and the fraying of traditional family forms correlated with their increases. On the other hands, beauty ideals and the role of weight and shape concerns could not be associated with etiology substantially, so they suggested limitations to the model of "Westernization". In these significant reviews, Pike and colleagues [3, 4] mentioned that unique subtypes and recent differences among AN may be more multi-layered than was previously thought that conventional case has historically been the norm.
In the present article, to complement previous discussion and to detect more culturally sensitive explanation, the author reviewed historical descriptions of AN in Japan and summarized prevalence of AN introducing domestic research data. This paper also described current medical situation for treatment of AN in Japan, and the author commented future perspective to neurocognitive research of AN.
Early history of anorexia nervosa in medicine
A description of anorexia nervosa (AN) can be found as early as the 18th century in Japan. Shyutoku Kagawa (1683-1755), a physician in the Edo Period, reported ?????? “Fusyoku no Syou (anorexia condition)” in the ???????? “Ippondokoyoigen” (1788) [5], which is an old medical textbook with 22 chapters (chapter 5 is about psychiatric illnesses). To summarize this important and interesting description, “Fusyoku no Syou is a very rare illness and this condition has not yet been reported. I have seen over 30 such cases until now—many of them have been women, as well as two or three males. These patients did not eat the usual rice (staple), and deviated to have wheat or bran. They did not seem to be starved in spite of anorexia, and they were not hungry all day long. The patients did not have other physical diseases or illnesses. The course of illness spanned several years in most cases. If someone forced them to eat food or take medications (crude or herb drugs), they vomited invariably. The patients’ families called doctors, performed purification, or had a traditional ceremony; however, these efforts led to worse consequences. Many doctors did not know this condition, so their efforts to compensate for it made patients resist or purge even more. It might be a better strategy to try not to treat these conditions aggressively.” He described probable AN cases approximately 100 years before Gull’s momentous paper [6, 7]. It is impressive that AN was included as a psychiatric illness, and in particular, it is incredible that therapeutic approaches for family or relatives were considered. His recommendation for prudent intervention and warning against over-interference may still correspond with current core treatments for AN.
According to increases in AN prevalence in Western societies in the 19th century, some Japanese researchers reported having founded clinical studies of AN in psychiatry and psychosomatic medicine from the 1950s through 1970s, including Kaziyama (1959), Ishikawa (1960), Shimosaka (1961-1978), Ikemi (1966), and Aoki (1976). Kaziyama [8] introduced 20 cases with AN, and he followed up on these patients for 15 years. He pointed out the specific characteristic—ignorance of own physical situation— and he considered this to be a potential defense mechanism against frustration. Shimosaka’s reports on AN were monumental benchmarks for eating disorder (ED) studies in Japan [9-11]. He described that adolescent patients with AN mainly demonstrated fear of obesity and desire for thinness, and were characterized by aversion or denial of maturity, envy of infancy or childhood, subliminal pessimism, asceticism, and intellectualism. Individual behavioral and psychological problems were considered to be based on the specific psychopathology, and the psychiatric phenomenon of AN consisted of two components: one was comprehensive regarding their character, conflicts with family members, or interactions among them psychologically; and the other was physiological-based pathology due to starving and malnutrition. This is very similar to our modern hypothesis that psychological and behavioral problems of AN are derived from bio-psycho-social interactions. Aoki et al. [12] classified AN into three types of cases based on age and psychosomatic adaptability: young competitive type, narcissistic puberty type, and maladjusted chronic adolescent type. According to these reports, before the drastic increase in EDs in Japan, some insightful studies were accomplished by medical pioneers.
Prevalence of AN in Japan
After the early medical reports of AN in Japan, the first official Research Committee for AN (including atypical EDs) by the Ministry of Health, Labour and Welfare (MHLW, formerly MHW) was developed in 1981. In 1980–81, 1985, 1992, and 1998, annual surveys were conducted for clinical samples targeting only representative hospitals in Japan. Regarding the summary reviews [13-15], these surveys targeted all university hospitals and larger hospitals over 300 beds (1,030, 5,283, 5,057, and 23,041 respectively), and questionnaire-based AN criteria were used for detection. In the first two surveys, the original criteria for AN were developed according to the Feighner’s criteria [16] because the DSM-III was considered unsuitable for Japanese situations. This criteria consisted of the following: 1. Over 20% emaciation 2. Over 3 month’s duration 3. Under 30 years old 4. Female 5. Amenorrhea 6. Eating abnormality 7. Desire for thinness 8. Hyperactivity 9. Ignorance of disorders and 10. Differentiated diagnosis. In 1989, these criteria were revised such that cases with 1, 3, 5, 6, 7 and 10 were diagnosed with AN. In 1998, the DSM-IV was applied. Consequently, the surveys found 980, 2,391, 2,068 and 5,417 patients in each respective annual report. Regarding differences in response rate (33.0%, 64.3%, 37.4% and 61.0% respectively), the research committee expected the estimated number of patients (annual prevalence per 100,000 populations) to be as follows: 2.2–2.75 in 1980–81, 2.9–3.7 in 1985, 3.6 in 1992 and 8.3–11.9 in 1998. For an all-female sample of individuals 10–29 years old, the actual rates were 14.4–18.0 in 1980–81, 20.4–25.3 in 1985, 21.8 in 1992 and 51.6–73.6 in 1998. There were more cases among teens, and over 90% were female. The estimated prevalence of AN in Japanese hospitals increased approximately 5 times over about recent 20 years [17], after earlier double rises of total number of patients with AN in 1981 comparing those in 1976 [18].
Additionally, one epidemiological study reported on the point prevalence of AN in Japan. Nakamura et al. [19] asked doctors in all of the relevant medical facilities (130 hospitals and 1,326 clinics) in a local prefecture to report patients with DSM-IVdiagnosed EDs who appeared or were admitted October 20–24, 1997 (response rate, 94.4%). The estimated point prevalence of AN was 4.79 per 100,000 females. Specifically, for the 15–29-year age group, the prevalence of AN was 17.1. This was lower than that for European Caucasian populations. After these projects, few epidemiological reports have been made using a large clinical sample for EDs in Japan. However, Nakai et al. [17, 20] followed 532 patients with ED discharged from hospitals and clinics in the Kyoto area in 2007. It was found that 55% finally came to clinics, but not hospitals. Therefore, the real prevalence might be approximately double that reported by national surveys targeting only hospitals.
Other epidemiological surveys on non-clinical samples were conducted in 1983 and 1993 by the Research Committee [21]. Similar questionnaire-based investigations for student samples (12–18-year-old junior high or high school females) were also reported from 1983 to 2002 [13,14,15,22,23]. Many used the national survey’s original self-rating or interview, the DSMIV based interview, or the EAT-26. Sample sizes ranged from 456 to 21,153, and the findings indicated that AN prevalence is higher based on interviews as compared to questionnaires [15]. According to the data, we determined possible AN in 0.04–1.4% of Japanese students, showing a gradual increase (almost 4 times over 10 years according to Nakai’s studies in the Kyoto area) [20]. Only one study used interviews of 1,130 females by nursing teachers among 13 high schools in Japan, and the highest prevalence was reported (2.03% in 2002)[24]. The most recent survey has been published by Hotta et al. [25] using a questionnaire to elementary, junior high, and senior high schools in seven prefectures. The point prevalence of AN for girls, including strongly suspected cases, in the three grades of junior high school and three grades of senior high school were 0-0.17 %, 0-0.21 %, 0.17-0.40 %, 0.05-0.56 %, 0.17-0.42 % and 0.09-0.43 % respectively. They also alarmed that approximately 30-50% of diagnosed and strongly suspected students with AN had not received medical consultation or treatment.
In 2004, Makino et al. [26] compared prevalence rates of ED between Western and non-Western countries. In Western countries, population-based and patient-based rates of AN ranged from 0.1% to 5.7% in female subjects, while in non-Western cultures (Japan, Hong-Kong, Iran and Singapore), estimates ranged from 0.002% to 0.9%. Buhrich [27] reported that 0.05% of the psychiatric patient sample in Malaysia was diagnosed with AN. On the other hand, the percentage of disturbed attitudes accounting for EAT-26 total scores in non-Western countries ranged from 0.8% [28] to 39.5% [29] compared to 8.3% [30] to 26% [31] in Western countries among females. Thus, Makino et al. concluded that questionnaire-based abnormal eating attitudes have been gradually increasing in non-Western countries.
Regarding another review by Chisuwa and O’Dea [32], Englishwritten epidemiological studies and clinical reports show AN prevalence from 0.025% to 0.2% in Japan, and patients with ED’s have increased significantly over the past two decades. On the other hand, they concluded that the prevalence in Japan remains lower compared to that in Western countries. However, this paper did not cover the Japanese national surveys mentioned previously; thus, this comment was considered controversial [9]. Recently, many Japanese researchers have pointed out the chronicity and spread of age of onset (from youth to middle age) [33], and so it is important to support AN patients across the lifespan.
Socio-cultural concerns
Beginning in the 1980s, the number of patients with EDs has increased dramatically in Japan. According to acute inflation of AN in particular, several hypotheses from various fields, even the mass media, have emerged. Psychological, anecdotal, and social concerns have included “anorexegenic mothers,” mother/daughter connectivity over maternal culture in Japan,” “Westernization of lifestyle,” “satiation or engorgement,” “feminist perspective such as male-dominated distortions,” and “societal pressure for girls to be thin from fashion magazines, TV stars, idols, celebrities, etc.”
The narratives, such as societal pressures according to the Westernization of Japan, including eating attitudes, continue to be popular [34]. Engorgement seems to play a key role in AN development, but Westernized eating styles in Japan started from the 1950s after World War II. Actually, the average height of 20-year-old Japanese individuals has not changed since 1980, following growth from 1950 to 1980 due to improved nutrition [35]. Thus, it is impossible to place over-satiation as a top AN etiology based on those phenomena [36]. In contrast, there are so many convenience stores nationwide, at which we can buy and eat food anytime and anywhere. At the very least, this might be one factor related with increases in ED’s [37].
Following the economic growth in Japan around 1990, societal pressure to be thin became exaggerated in the media and among peers. In addition, advances in social standing for women were coincident with suspicious trends to consider thinness or appearance of women or girls as an indicator of ability or validity. In the 1990’s, the prevalence of AN increased in Singapore and some researchers emphasized the influences of Japanese TV stars or idols that became popular in this time [37]. Still, the growth of AN in Asian country could be associated with male-dominant society or media literacy.
We proposed a social hypothesis that might explain ED increases in Japan, which includes diversification of role and advances of information [36]. In traditional Japanese society, there is a tendency to accept a fixed course of future occupation or career according to living area or family to some extent. Nowadays, the higher education continuance rate is rising, and there are many alternatives for future lifestyles. On the other hand, the norm for conformity has become ambiguous. We can access a significant amount of information through the internet from all over the world easily and promptly, and it sometimes brings confusion or ambivalence. A traditional way of life has been reviewed, and young people must choose for themselves from many options in this diversified society. In addition, moratorium periods have been shortened because of this information-driven society (i.e., ‘mouse years’). This means that it is easy for adolescents to feel at a loss in society while they try to construct an identity. They seek to have a cornerstone, and some may find one curious value, namely, “control of shape and desire for thinness.” When they begin to feel anxiety or distress, some of them may find that an easy way to express their disgust as a coping mechanism is binging or purging. According to Erikson’s theory, confusion of social role is the main theme for adolescents, but nowadays, this issue can be relevant for every stage of the lifespan, including middle and older age in an information-driven society. In fact, prolongation of the age at which AN might be developed might be predicted by this hypothesis, as many there may be links with AN across the lifespan, including interpersonal relationships, marriage, career, retirement, and solitude in old age.
Neurocognitive findings
It is known that AN can impact on some cognitive processes, such as executive functions [38], attention [39] and social cognition [40]. Recent international neuroimaging studies have demonstrated several possibilities in research of AN, such as perceiving kindness may be a trait of AN whereas recognizing malevolence may be linked to recovery [41]. A fMRI study using graph-theoretical measures indicated wide disturbances in information flow across brain networks in acute AN, which may explain abnormal representations of body size and hunger [42]. Ehrich et al. explored unaltered neural responses in ventral limbic reward networks but increased recruitment of and connectivity with lateral-frontal circuitry in recovered AN, and suggested an imbalance between an elevated degree of selfregulatory processes and responses to rewarding stimuli as a trait maker [43]. A study of set-shifting and central coherence consistent with an inflexible thinking and overly detailed processing showed that context-appropriate responses supported by prefrontal cortex may benefit from cognitive therapy and sustain inhibition of an unwanted response, subserved by the anterior middle frontal gyrus, might be a predictor of favorable outcome to cognitive treatment in AN [44].
In a next future, it could be believed that a further study of neurocognitive mechanisms in AN could provide important insights for both diagnosis and treatment even in Japan, for instances, as the Attention Bias Modification Treatment showed promise as a novel treatment for anxiety [45].
The National Centre Initiative in Japan
As we have seen above, significant increases in AN have been shown in Japan, and its extreme damage to the individual is remarkable. Considerable effort and burden for patients and families as well as professionals is required to cope with AN physically, psychologically, and socially. In particular, under universal health care, the Japanese system of nationwide public health insurance cannot provide intensive treatment for complicated disorders such as AN, which requires a multidisciplinary approach. Therefore, time and costs associated with treating AN have not been required for management by medical organizations or clinics. Until 2010, there has been no official support from a centralized health system for treatment or prevention of AN in Japan. However, now, in the Japanese Medical Payment System, the management care fee for inpatients with AN was included, though several limitations remain. It includes 2,000 JPY per day within 30 days and 1,000 JPY within 60 days to inpatient intensive care, but only for cases with a BMI of less than 15. Aside from this point, the total social cost for health and welfare in Japan continues to grow rapidly, owing to the fastest aging society worldwide. Accordingly, it might be more difficult to maintain the current public insurance system due to a shortage of resources.
Consequently, some clinicians, patients, families, and related individuals have moved to develop a national institute or center to systematically and rationally cope with this difficult disorder. They collaborated for a signature campaign nationwide, conducted press conference, and initiated a big movement to support ED’s. Finally, the MHLW decided to present a preliminary initiative for an ED care system in Japan [45]. As seen in Figure 1, the MHLW envisages one centralized institute to develop a novel treatment and integrate findings nationwide. This central institute supervises the other local sites (around 10 local centers), which interact with each other. These local centers in represented areas received acute phase patients with ED, and advice and consultation from local clinics or hospitals. However, a final proposal discouraged those involved because it was insufficient with regard to total amount of the budget allocated for local supporting sites. The MHLW does not seem to play a leading role in initiating this system and constituting a brand-new centralized institution have been given up. It is only receiving voluntary applications from some candidates (hospitals anywhere in Japan) coming forward for this project. Unfortunately, as of now, only a few hospitals or institutes have applied for this grant.
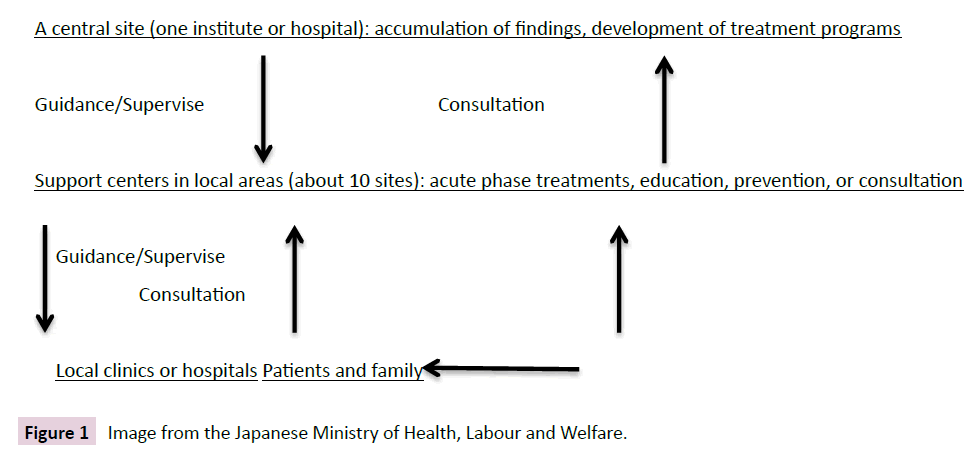
Figure 1: Image from the Japanese Ministry of Health, Labour and Welfare.
Treatments or interventions based on the new Japanese guideline
Individual research groups or pediatric professionals in Japan proposed respective original guidelines for AN, but the official consensus did not achieve bridging between psychiatry and psychosomatic medicine. In 1997, the Japanese Meeting for Eating Disorders was established among several professionals, and this developed into the Japanese Society for Eating Disorders (JSED) in 2005. The society planned a committee to construct guidelines for improvement of diagnosis and treatment of ED in Japan, and the first Japanese guideline according to the Japanese evidence was agreed upon by the JSED in 2012. In this guideline [46], several therapeutic approaches are included and explained by leading professionals as follows: individual psychotherapy, behavioral therapy, cognitive behavioral therapy, psychodynamic psychotherapy, interpersonal psychotherapy, family therapy and psychoeducation, physical and nutritional management, group therapy, art therapy, reparenting therapy (originally developed in Japan by Yamaoka [47]), mutual support group, and medication.
To overview existing interventions for AN in this guideline, we find detailed chapters about assessments and case formulation in the first step. Next, chapters including introduction and selection of treatment are made, and emergency matters are described. In the body of this guideline, we have detailed explanations of respective treatment and therapy individually. As for inpatient treatments, there are four sections such as in a general medical unit, for the behavioral approach using limit setting, in a psychiatric ward, and for a brief or a long-term treatment. The guideline contains some chapters about strategies to case with psychiatric comorbidity, physical complications, and team approach. Prevention, outcome and medical administration are mentioned in the final section. It recommends appropriate applications in a typical clinical setting based on evidence, and it also recommends social approaches such as rehabilitation and local networking. Now, Japanese professionals have to practice according to this guideline, and should accumulate more accurate data and experience to support, prevent, and manage AN in Japan.
References
- Fairburn CG, Harrison PJ (2003) Eating disorders. Lancet361: 407-416.
- Treasure J, Claudino AM, Zucker N (2010) Eating disorders. Lancet375: 583-593.
- Pike KM, Dunne PE (2015)The rise of eating disorders in Asia: a review. Journal of Eating Disorders 3: 33.
- Pike KM, Borovoy A (2004)The rise of eating disorders in Japan, issues of culture and limitations of the model of "westernization". Cult Med Psychiatry28: 493-531.
- Kagawa S. Fusyokunoshyo (1788) In: Ippondokoyoigen, chapter5, Suharaya/Akitaya/Kawachiya, Edo/Osaka 40.
- Gull WW (1874) Anorexia nervosa. Transactions of the clinical society of London7: 22-28.
- Gull WW (1997) V.-Anorexia Nervosa (ApepsiaHysterica, Anorexia Hysterica). Obesity research 5: 498-502.
- Kaziyama S (1959) Clinical study of Anorexia Nervosa. PsychiatriaetNeurologia Japonica 61:82-98.
- Shimosaka K (1961) Psychiatric study of adolescent anorexia nervosa. PsychiatriaetNeurologia Japonica63: 1041-1081.
- Shimosaka K (1963) Psychiatric problems of anorexia nervosa. Clinical Psychiatry (SeishinIgaku) 5: 259-274.
- ShimosakaK (1978) Treatment of anorexia nervosa, Jap J Clinical Psychiatry (RinshyoSeishinigaku) 7: 1273-1283.
- Aoki H, Suematsu H, Esaki M, Kurokawa N et al. (1976) Psychosomatic research of etiological mechanism in anorexia nervosa. Jap J Psychosomatic Med (ShinshinIgaku) 16: 30-38.
- Nakai Y (2005) Epidemiology of eating disorders. Psychosomatic Int Med (ShinryoNaika) 9: 299-305.
- Nakai Y, Nin K, Suzuki K (2015) Epidemiology of eating disorders. Brain 21 (Nou21) 18: 153-157.
- Nakai Y (2012) Epidemiology of eating disorders. J Clinical Experimental Med(Igaku no Ayumi) 241: 671-675.
- Feighner JP, Robins E, Guze SB, Woodruff RA Jr, et al. (1972) Diagnostic criteria for use in psychiatric research. Arch Gen Psychiatry 26:57-63.
- Nakai Y, Hamagaki S, Noma S, et al. (2009) Survey of eating disorders among medical facilities in Kyoto City. Clinical Psychiatry (SeishinIgaku) 51: 681-683.
- Suematsu H, Ishikawa H, Kuboki T, Ito T (1985) Statistical studies on anorexia nervosa in Japan: detailed clinical data on 1,011 patients. PsychotherPsychosom43: 96-103.
- Nakamura K, Yamamoto M, Yamazaki O, Kawashima Y, et al. (2000) Prevalence of anorexia nervosa and bulimia nervosa in a geographically defined area in Japan. Int J Eat Disord 28:173-180.
- Nakai Y (2010) Change of Prevalence of Eating Disorders and Eating Disorder Symptoms. Clinical Psychiatry (SeishinIgaku) 52: 379-383.
- Inaba Y (1994) The Annual report of the Research Committee of anorexia nervosa by the Ministry of Health and Welfare in 1995: 45-47.
- Kuboki T, Nomura S, Ide M, Suematsu H, et al. (1996) Epidemiological data on anorexia nervosa in Japan. Psychiatry Res 62:11-16.
- Nakai Y, Naruo T, Suzuki K et al. (2004) Outcome of Eating Disorders in Japan. Clinical Psychiatry (SeishinIgaku)46: 481-486.
- Watanabe H (2000) Investigation for epidemiology and support of adolescent anorexia nervosa. The final report of the Scientific Research by the Ministry of Health, Labor and Welfare grants in 2002. 2: 212-216.
- Hotta M, Horikawa R, Mabe H, et al. (2015) Epidemiology of anorexia nervosa in Japanese adolescents. BioPsychoSocial Medicine 9: 17.
- Makino M, Tsuboi K, Dennerstein L (2004) Prevalence of eating disorders: a comparison of Western and non-Western countries. MedGenMed 27: 6-49.
- Buhrich N (1981) Frequency of presentation of anorexia nervosa in Malaysia. Aust N Z J Psychiatry 15:153-155.
- Nakamura K, Hoshino Y, Watanabe A, et al. (1999) Eating problems in female Japanese high school students: a prevalence study. Int J Eat Disord26:91-95.
- Babar N, Alam M, Ali SS, Ansari A, et al. (2002) Anorexic behaviour and attitudes among female medical and nursing students at a private university hospital. J Pak Med Assoc52:272-276.
- Neumarker KJ, Bettle N, Bettle O, Dudeck U, et al. (1998) The Eating Attitudes Test: comparative analysis of female and male students at the Public Ballet School of Berlin. European Child and Adolescent Psychiatry7:19-23.
- Graber JA, Tyrka AR, Brooks-Gunn J (2003)How similar are correlates of different subclinical eating problems and bulimia nervosa? J Child Psychol Psychiatry44:262-273.
- Chisuwa N, O’Dea JA (2010) Body image and eating disorders amongst Japanese adolescents. A review of the literature. Appetite 54: 5–15.
- Naruo T (2013) Eating disorders in the middle-aged generation. Jap J Clinical Psychiatry (RinshyoSeishinigaku) 42: 553-559.
- Nishizono-Maher A (1998) Eating disorders in Japan: finding the right context. Psychiatry ClinNeurosci 52:S320-323.
- Database of the National Health and Nutrition Survey Japan. The National Institute of Health and Nutrition.
- Sato H, Uehara T (2015) History of eating disorders. Clinical Journal of Psychiatric Service 15: 275-281.
- Uehara T (2004)A princess obsessed by eating. Seiwa Publisher, Tokyo.
- Caglar-Nazali HP, Corfield F, Cardi V, Ambwani S, et al. (2014) A systematic review and meta-analysis of 'Systems for Social Processes' in eating disorders. Neuroscience &Biobehavioral Reviews 42: 55-92.
- Dalmaso M, Castelli L, Franchetti L, Carli L, et al. (2015) Altered orienting of attention in anorexia nervosa. Psychiatry Research 229: 318-325.
- Roberts ME, TchanturiaK, Stahl D, Southgate L, et al. (2007) A systematic review and meta-analysis of set-shifting ability in eating disorders. Psychological Medicine 37: 1075-1084.
- McAdams CJ, Lohrenz T, Montague PR (2015) Neural responses to kindness and malevolence differ in illness and recovery in women with anorexia nervosa.Hum Brain Mapp29.
- Geisler D, Borchardt V, Lord AR, Boehm I, et al. (2015) Abnormal functional global and local brain connectivity in female patients with anorexia nervosa. J Psychiatry Neurosci 11: 40.
- Garrett AS, Lock J, Datta N, Beenhaker J, et al. (2014) Predicting clinical outcome using brain activation associated with set-shifting and central coherence skills in Anorexia Nervosa. J Psychiatr Res 57: 26-33.
- Hakamata Y, Lissek S, Bar-Haim Y, Britton JC, et al. (2010) Attention bias modification treatment: a meta-analysis toward the establishment of novel treatment for anxiety. Biological Psychiatry 68: 982-990.
- The Ministry of Health, Labor, and Welfare Japan.
- Japanese Society for Eating Disorders: Treatment guideline for eating disorders (2012) The Committee of developing treatment guideline in Japan Edt. IgakuShyoin Publishers, Tokyo.
- Yamaoka M (2012)Reparenting therapy. In Treatment guideline for eating disorders. (The Japanese Society for Eating Disorders: The Committee of developing treatment guideline in Japan edt.), IgakuShyoin Publishers, Tokyo 138-144.

