Keywords
Congenital heart disease; Patent ductus arteriosus; Device closure; Cardiac cath complications
Introduction
Worldwide the ductus arteriosus remains patent (PDA) in 0.87 per 1,000 live births [1]. The clinical and laboratory findings of PDA vary considerably with the volume of pulmonary blood flow, the status of pulmonary vasculature, and the presence of coexistent cardiac anomalies [2]. The presence and size of the PDA can be confirmed using echocardiography before measures are undertaken to close the defect. Doppler techniques are used to estimate the pulmonary artery pressure [3,4]. All PDAs that are apparent by physical examination should be closed. Whether to close very small PDAs that are detected serendipitously by echocardiography in the absence of typical physical findings is controversial [5]. PDA can be closed with a variety of devices at the time of cardiac catheterization. Catheter directed therapy for PDA has gradually evolved since its introduction in 1967 [5]. In 2003, the AMPLATZER duct Occluder was the first FDAapproved device for PDA closure [6]. The strategy for PDA closure by coil varies from operator to operator and includes both ante grade and retrograde approaches. For PDA device closure, venous access must be obtained for device Delivery. Arterial access is used to obtain angiograms during device delivery [6].
Angiography may be obtained from the venous side by passing a wire ante grade across the duct and exchanging the catheter for appropriate catheter. PDA device closure can be performed without an arterial access. We are presenting our experience in closing the PDA with and without arterial access.
Patients and Methods
Our study is a combined prospective as well as retrospective one. From February 2012 till August 2014, a retrospective review of all patients underwent transcatheter PDA closure were included. Since 2013 we are intending to close the PDA without arterial access which were prospectively reviewed. Device closure was performed for any hemodynamically significant PDA. Detailed Echocardiographic evaluation of the heart including assessment of the PDA size, PDA type, presence and size of PDA ampulla, assessment of branch pulmonary arteries and main pulmonary artery, as well as careful assessment of the aortic arch. Hemodynamic doppler assessment is performed to assess the PDA shunt as well as the PA pressure.
Since 2013 our protocol is to do PDA device closure without an arterial access except in selected patients when arterial access was considered necessary and was obtained for the following group of patients:
(1) Inadequate echocardiographic definition of the PDA and aortic arch.
(2) Large ducts with echocardiographic signs of pulmonary hypertension for which full diagnostic hemodynamic is essential prior to attempted PDA device closure.
(3) Small infants with large ducts requiring bigger devices which can potentially cause descending aortic obstruction.
(4) Patients with additional lesions requiring hemodynamic assessment and/or intervention.
(5) Accidental arterial puncture while trying to obtain venous access (Vaygon canula inserted in the arterial line).
Informed consent was obtained. All procedures were performed under general anaesthesia. For those without arterial access blood pressure was monitored noninvasively. Heparin 50 unit/ kg bolus was administered after vascular access (100 unit/kg if arterial access was obtained). This study was approved by the hospital research committee.
Angiographic definition of the PDA
In those with arterial sheath, a 4 Fr pigtail catheter was used to do descending aortogram at the area of the PDA. (Figure 1) During the procedure, the vital signs and peripheral oxygen saturations were monitored. In those with no arterial line, angiography was performed by a 5 Fr multipurpose catheter with side holes (MPA2 catheter) passed antegradely from the PA to the aorta through the PDA. Angiography was performed by placing the tip of the catheter at the junction of the PDA with the aorta. Angiography was performed by either hand injection in small patients or by injector using a low PSI (Pounds per square inch) (200 PSI to 300 PSI) (1 atmosphere is approximately 14.7 PSI) to avoid catheter recoil. The retrograde blood flow into the pulmonary artery from the proximal descending thoracic aorta allows definition of the PDA. The ductal size was measured and was compared with the echocardiographic measurement. The device was selected according to the angiographic and echocardiographic measurements as well as the presence and size of the PDA ampulla and aortic arch size. The PDA classifications were made according to Kirchenko classification [7].
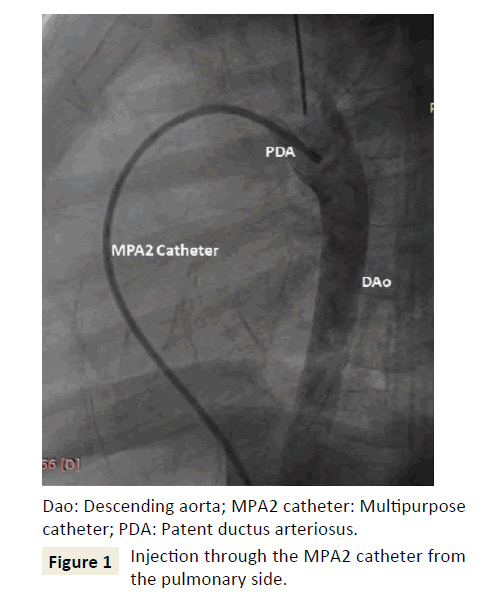
Figure 1: Injection through the MPA2 catheter from the pulmonary side.
Device size selected was 2 mm larger than the narrowest PDA diameter. Device was deployed according to the described standard technique [6]. After deploying the device and before device release angiography was performed through the side port of the long sheath leading to opacification of the MPA and visualization of the PA end of the device within the PDA–PA junction. The aortic arch can be seen in the levophase, which allows the exclusion of any arch obstruction by the device (Figure 2).
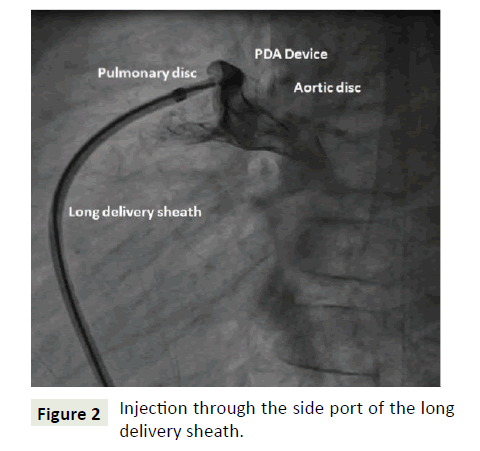
Figure 2: Injection through the side port of the long delivery sheath.
Echocardiography was performed 2 hrs to 4 hrs in the same day of the procedure. Device placement was assessed by 2D echocardiography in the parasternal, ductal, and suprasternal views. Colour flow mapping was done to check for residual flow through the ductus as well as turbulence at left pulmonary artery origin or in the descending aorta.
Patients were discharged either in the same day 8 hrs after the procedure for those with no arterial sheath or 24 hrs after the procedure. All patients had echocardiographic evaluation 24 hrs after the procedure. All patients had 1 month follow up after the procedure, then after 3 months, 6 months and then annually. Follow up variables include clinical condition, ECG, and detailed echocardiography concentrating on assessing the device position, presence of residual shunt, assessment of branch pulmonary arteries and aortic arch patency as well as assessing cardiac function and excluding the presence of pericardial effusion. Statistical analyses were performed using IBM SPSS statistics software. Independent samples test was used for continuous variables and chi-squared test was used for categorical variables to compare between the two groups (those with and without arterial access). Values are expressed as frequencies and percentages or mean and standard deviations and range as appropriate.
Results
During the period 45 patients underwent PDA device closure at PSCC-Qassim. The mean age was 27 +/- 25 months (range 6 months to 6 years). The mean weight was 11 kg ± 5 kg (range 6 to 27 kg) (Table 1). Females constitute 67% (30 patients). Eight patients (18%) have Down syndrome. Thirteen patients (29%) have additional cardiac problems (Table 2).
| For all patients |
Mean |
Std. deviation |
Minimum |
Maximum |
| Height (cm) |
85.2 |
17.4 |
65 |
131 |
| Weight (Kg) |
11.2 |
5.2 |
6 |
27 |
| Age (months) |
27.4 |
25.3 |
6 |
120 |
| Contrast (ml) |
18.7 |
11.8 |
10 |
80 |
| Flouro (time) |
6.1 |
4.7 |
2.2 |
23 |
| Procedure (time) |
38.2 |
19.4 |
15 |
110 |
Table 1: Patient demographics as well as the amount of contrast used and total procedure time and fluoroscopic time for all patients.
| Anomaly |
Frequency |
Percent |
| Congenital CHB, S/P PPM |
1 |
2.2 |
| History of pulmonary hypertension |
1 |
2.2 |
| Long QT interval (c QT 480 |
1 |
2.2 |
| Mild MVP, Mild MR |
1 |
2.2 |
| No |
32 |
71.1 |
| Persistent left superior vena cava |
2 |
4.4 |
| Small ASD |
2 |
4.4 |
| Small muscular VSD |
2 |
4.4 |
| Small sub aortic membrane |
3 |
6.7 |
| Total |
45 |
100.0 |
Table 2: Associated cardiac problems.
All had detailed pre-intervention echocardiographic assessment. All have venous access. Fourteen patients (31%) have additional arterial access by a 4 French sheath and 4 patients (9%) have arterial line using a Vaygon 20 canula. Since 2013 our protocol is to do PDA device closure without an arterial access except in selected patients when arterial access was considered necessary.
Angiogram was performed through the venous route in 32 patients (71%), and by the arterial accessed catheter in 13 patients (29%). PDA types are outlined in Table 3. PDA was closed by Amplatzer Duct Occluder type 1 (ADO1) device in 25 patients (56%), Oculotech PDA device in 18 patients (40%), and by coils in 2 patients (4.4%). Size and type of PDA devices used is outlined in Tables 4 and 5.
| |
Frequency |
Percent |
| A |
26 |
57.8 |
| B |
5 |
11.1 |
| C |
3 |
6.7 |
| E |
11 |
24.4 |
| Total |
45 |
100.0 |
Table 3: PDA types.
| Device size |
Frequency |
Percent |
| 10/8 mm |
3 |
6.7 |
| 3.5/5 mm |
1 |
2.2 |
| 3/6 mm |
1 |
2.2 |
| 4/2 mm |
1 |
2.2 |
| 4/5 mm |
1 |
2.2 |
| 4/6 mm |
5 |
11.1 |
| 5/3.5 mm |
1 |
2.2 |
| 5/4 mm |
1 |
2.2 |
| 5/7 mm |
1 |
2.2 |
| 6/4 mm |
17 |
37.8 |
| 6/8 L mm |
2 |
4.4 |
| 6/8 mm |
2 |
4.4 |
| 7/5 mm |
2 |
4.4 |
| 8/6 mm |
5 |
11.1 |
| PDA coil |
2 |
4.4 |
| Total |
45 |
100.0 |
Table 4: Size of PDA devices used.
| Device type |
Frequency |
Percent |
| ADO 1 |
25 |
55.6 |
| Coil |
2 |
4.4 |
| Oculotech |
18 |
40.0 |
| Total |
45 |
100.0 |
Table 5: Types of PDA devices used.
For the whole cohort, the mean procedure time was 38 min ± 19 min, the mean fluoroscopic time was 6 min ± 5 min and the mean contrast given was 18 ml ± 11 ml (Table 1). Two patients had immediate complications (significant bradycardia in one and mild pericardial effusion 24 hrs after the procedure which regressed over 48 hrs of close follow up in another) (Table 6).
| Early and late complications |
Age (months) |
Wt |
PDA type |
Device used |
| Transient Bradycardia |
6. |
6 kg |
A |
6/4 mm Oculotech |
| Depressed function |
6 |
6 kg |
A |
6/4 mm Oculotech |
| Pericardial effusion |
9 |
8 kg |
B |
6/4 ADO 1 |
| LPA stenosis |
23 |
9 kg |
E |
5/3.5 Oculotech |
| LPA stenosis |
9 |
7 kg |
B |
6/8 Oculotech |
Table 6: Immediate, early and late complications post PDA device.
Comparing the differences between those without arterial line (group one) and with arterial access (group two) revealed that the procedure time, the fluoroscopic time as well as the amount of contrast given were less in those with no arterial access (Table 7). On follow up one patient developed significantly depressed LV function detected one month after the procedure which improves over a period of 9 months. No patient had residual shunt and no patient had arch obstruction. Two patients developed mild turbulence in LPA with a gradient of 15 mmHg in both. No patient required reintervention (Table 6).
| |
Venous ± arterial access |
N |
Mean |
Std. deviation |
P value |
| Height (cm) |
Group 1 |
27 |
78.92 |
14.01 |
0.003 |
| Group 2 |
18 |
94.17 |
18.28 |
| Weight (Kg) |
Group 1 |
27 |
8.87 |
3.47 |
0.001 |
| Group 2 |
18 |
14.54 |
5.45 |
| Age (months) |
Group 1 |
27 |
19.46 |
22.00 |
0.015 |
| Group 2 |
18 |
38.78 |
26.09 |
| Contrast (ml) |
Group 1 |
27 |
15.31 |
4.88 |
0.05 |
| Group 2 |
18 |
23.67 |
16.46 |
| Flouro time |
Group 1 |
27 |
4.36 |
1.86 |
0.011 |
| Group 2 |
18 |
8.69 |
6.30 |
| Procedure time |
Group 1 |
27 |
78.92 |
14.01 |
0.038 |
| Group 2 |
18 |
94.17 |
18.28 |
Table 7: Comparison between those with and without arterial access (group 1=venous access only, group 2=venous and arterial access).
Discussion
Closure of the PDA through interventional cardiac catheterization is a well-established way of management [8-10]. Different devices are used for PDA device closure; the most common used device is the Amplatzer Ductal Occluder (ADO-I; AGA Medical Corporation) [11]. Oculotech PDA occluder (Oculotech International AB) is a PDA occluder device which is available in the market and is approved for use in Europe, but still under clinical investigation in USA [12,13].
Echocardiography is an excellent tool for diagnosis of most congenital heart disorders. Echocardiography alone is an accurate tool for preoperative diagnosis of major congenital heart defects in most children undergoing primary complete repair. Most of patients nowadays are taken to the operating theatre for cardiac surgery based on echocardiographic diagnosis and evaluation [14,15].
Echocardiography can be used for diagnosis of the PDA, delineation of the detailed anatomic characteristics of the PDA as well as the hemodynamic consequences of the PDA. Using a venous line only will be based on the echocardiographic assessment of the PDA, for example: if the PDA is so small, it cannot be crossed from the venous side and a retrograde approach should be used. If it is too large an arterial line will be essential to make sure that using a large device will not compromise the aortic arch. Also in small infants with a ductus with small or no ampulla, or with some isthmus hypoplasia, putting a device might cause arch obstruction, so arterial line will be essential in such cases.
Doing detailed hemodynamic assessment in the path lab for patients with PDA depends up on the echo findings. For those with no evidence of significant PHT there is no need for detailed hemodynamic assessment which might prolong the timing of the procedure. PDA is closed through the venous side. The arterial line is used for continuous monitoring of the blood pressure, doing arterial blood gas as needed, as well as doing aortogram pre-and post PDA device closure. Avoiding arterial line (sheath) may prevent the possible complications of arterial puncture including thrombosis, bleeding, longer catheterization and fluoroscopic time and probably prolonged hospital stay. Complications such as arterial disruption, or acute occlusion, may be limb-threatening. PDA closure using a venous access alone is possible and safe in experienced hands, provided that there is appropriate echocardiographic assessment, careful PDA definition by angiogram at the PDA ampulla or proximal descending aorta. The advantages of avoiding arterial access include, reducing the heparinization dose, and elimination of the inherent risks of arterial puncture (bleeding, femoral artery thrombosis). The procedure time, as well as the fluoroscopic time is shorter and many patients can potentially be discharged early.
It is important to have a good positioning of the catheter at the PDA ampulla-proximal descending aorta using either hand injection or pump injection with low PSI for angiographic PDA assessment. Angiograms can also be performed through the long delivery sheath. Arterial access may be required in some patients especially small infants, patients with large ductus, those who need careful assessment of the aortic arch and isthmus as well as those requiring detailed hemodynamic assessment, depending up on the interventionist decision and plan of intervention during the pre-intervention assessment.
Conclusion
PDA device closure without an arterial access can be performed safely and effectively with experienced hands. Patient selection and appropriate pre-intervention detailed echocardiography and procedure planning are essential for accomplishing device closure of PDA with or without arterial access. The procedure is simplified considerably and many patients can be discharged on the day of the procedure.
Conflict of Interest
None
Ethical Standards
Patient/family consent was taken for the procedure including explanation of the details of the procedure, vascular access as well as the possible complications.
References
- Van Der Linde D, Konings EE, Slager MA, et al. (2011) Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J Am Coll Cardio 58: 2241-2247.
- Webb GD, Smallhorn FJ, Terrien J, Redington AN (2008) Congenital heart disease. In: Braunwalds' Heart Disease, (8th edn), Libby P, Bonow RO, Mann DL, Zipes DP (eds), Philadelphia, USA. p. 1561.
- Condò M, Evans N, Bellù R, Kluckow M (2012) Echocardiographic assessment of ductal significance: Retrospective comparison of two methods. Arch Dis Child Fetal Neonatal Ed 97: F35-F38.
- Serwer GA, Armstrong BE, Anderson PA (1980) Noninvasive detection of retrograde descending aortic flow in infants using continuous wave doppler ultrasonography Implications for diagnosis of aortic run-off lesions. Pediatr 97: 394-400.
- Giroud JM, Jacobs JP (2007) Evolution of strategies for management of the patent arterial duct. Cardiol Young 2: 68-74.
- Robert HP, Ziyad H, Daphne TH, Veronica L, William E, et al. (2004) Multicenter USA amplatzer patent ductus arteriosus occlusion device trial: Initial and one-year results. J Am CollCardiol 44: 513-519.
- Kirchenko A, Benson LN, Burrows P, Möes CA, McLaughlin PA, et al. (1989) Angiographic classification of the isolated, persistently patent ductus arteriosus and implications for percutaneous catheter occlusion. Am J Cardiol 63: 877-880.
- Baruteau AE, Hascoët S, Baruteau J, Boudjemline Y, Lambert V, et al. (2014) Transcatheter closure of patent ductus arteriosus: Past, present and future. Arch Cardiovasc Dis 107:122-132.
- Liddy S, Oslizlok P, Walsh KP (2013) Comparison of the results of transcatheter closure of patent ductus arteriosus with newer Amplatzer devices. Catheter Cardiovasc Interv 82: 253-259.
- Ghasemi A, Pandya S, Reddy SV, Turner DR, Du W, et al. (2010) Trans-catheter closure of patent ductus arteriosus-what is the best device? Catheter Cardiovasc Interv 76: 687-695.
- Boehm W, Emmel M, Sreeram N (2007) The amplatzer duct occluder for patent ductus arteriosus closure: Indications, technique of implantation and clinical outcome. Images Paediatr Cardiol 9: 16-26.
- https://www.occlutech.com/index.php/en/patients/occlutech-devices
- https://clinicaltrials.gov/ct2/show/NCT01479218.
- Tworetzky W, McElhinney DB, Brook MM, Reddy VM, Hanley FL, et al. (1999) Echocardiographic diagnosis alone for the complete repair of major congenital heart defects. J Am Coll Cardiol 33: 228-233.
- Han BK, Lesser AM, Vezmar M, Rosenthal K, Rutten RS, et al. (2013) Cardiovascular imaging trends in congenital heart disease: A single centre experience. J Cardiovasc Comput Tomogr 7: 361-366.

