Ryan Shields1* and S A Erzurum1,2
1Northeast Ohio Medical University, Rootstown, Ohio
2Eye Care Associates, Youngstown, Ohio
*Corresponding Author:
Ryan Shields
Northeast Ohio Medical University, Rootstown, Ohio 3440 Olde Winter Trl, Poland, OH, 44514
E-mail: rshields@neomed.edu
Citation: Shields R,Erzurum SA (2016) Pediatric Cataract Extraction Utilizing the LenSx® Femtosecond Laser. J Eye Cataract Surg 1:4. doi: 10.21767/2471-8300.100004
Copyright: © 2016 Shields R, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Pediatric cataracts are a relatively common (1 to 15 per 10,000 children), but treatable worldwide morbidity [1]. Unfortunately, surgical intervention in children is often more difficult and associated with more complications than in adult patients. The surgical difficulty of pediatric cataract extraction can be attributed to the increased elasticity of the lens capsule as well as decreased scleral rigidity [2,3]. The advantages of the femtosecond laser including improved capsulotomy, better lens centration, and decreased posterior subscapular cataract formation, play to all of the disadvantages of pediatric cataract surgery [4-7]. There have only been five cases of pediatric femtosecond laser assisted cataract extraction, yet none utilizing the LenSx® (Alcon, Inc, Fort Worth, Texas) [8,9]. We report a case of a nine year old girl with bilateral cortical cataracts successfully managed with femtosecond assisted cataract extraction.
Case Report
The patient is previously well nine-year-old African-American female who was referred to the pediatric ophthalmologist after failing the school eye exam. On initial exam, she complained of worsening visual acuity over several months. Both her father and sister had early onset cataracts. Her sister had undergone bilateral cataract extraction six years previously with intraocular lens placement. The patient’s visual acuity was 20/40 in the right eye and 20/150 in the left eye. Objective refraction of the right eye was +0.25 +0.50 at 152 degrees with the left eye being +0.75 +0.50 at 66 degrees. Pupils were equal and reactive to light without an apparent pupillary defect. Extraocular motility was intact. Slit lamp examination was normal except for 3+ cortical changes in both eyes and 3+ posterior subcapsular changes in the left eye. Fundus exam was normal with cup to disc ratio of 0.3 bilaterally.
At this point, surgical extraction was recommended. The patient underwent a-scan biometry utilizing the Zeiss IOL Master (Zeiss, Oberkochen, Germany). Because of the clinician’s proficiency with the LenSx® system in adult cataract surgery, the parents were offered the option of laser assisted cataract extraction for their child. All of the risks, benefits, and alternatives were discussed with the patient’s family; they agreed to proceed and appropriate informed consent was obtained.
The patient was brought into the operating room where both the microscope and femtosecond laser were located; a laryngeal mask airway was used to secure the airway and anesthetize the child. Once the airway was secure, the child was rolled under the LenSx® Alcon femtosecond laser. The airway was maintained by manually bagging the patient.
The interface was easily centered over the cornea and suction was applied with no need for a lateral canthotomy. OCT images of the cornea and anterior chamber were taken (Figure 1). Anterior capsulotomy parameters were set with the following parameters: diameter 3.8 mm, 6.00 μJ, with incision depth at 600 μm. Corneal incision parameters for the paracentesis and primary incision were performed with the laser as well.
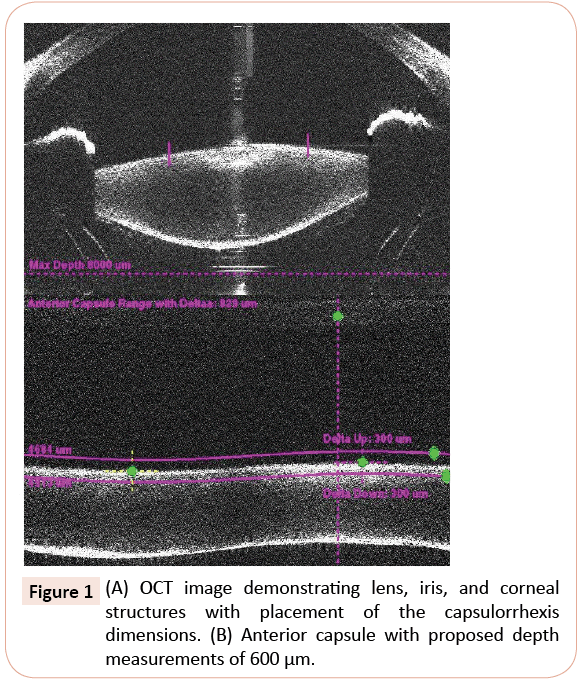
Figure 1: (A) OCT image demonstrating lens, iris, and corneal structures with placement of the capsulorrhexis dimensions. (B) Anterior capsule with proposed depth measurements of 600 μm.
The suction ring was removed and the patient's bed was rotated back under the operating room microscope to complete the manual lens removal and intraocular lens placement. Since both the microscope and the laser are in the same room, this was done relatively easily. The paracentesis and primary corneal incisions were gently opened using an Eippert spatula and viscoelastic was injected into the anterior chamber.
The anterior capsulotomy was inspected and it had expanded to approximately 5 mm in size. The edges were smooth and the capsule was free floating upon the surface of the lens, completely detached (Figure 2). The anterior capsule was removed and hydro dissection of the lens was performed with balanced salt solution. The lenticular material was aspirated with the phacoemulsification hand-piece. Remaining cortical material was removed to leave a clean capsular bag. An Alcon SN60WF, 22.5-diopter lens was injected into the capsular bag with excellent centration. One 10.0 nylon suture was used to secure the wound even though the wound did not show any leakage at the end of the surgery (Figure 3). The surgeon chose to place a suture to protect the eye from potential manipulation by the child upon awakening. Subconjunctival Kenalog (Triamcinolone Acetonide) was injected during surgery and the patient was prescribed one month of topical steroids.
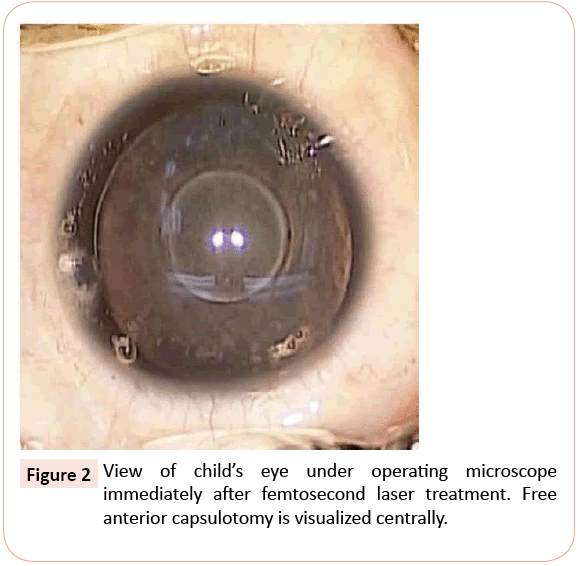
Figure 2: View of child’s eye under operating microscope immediately after femtosecond laser treatment. Free anterior capsulotomy is visualized centrally.
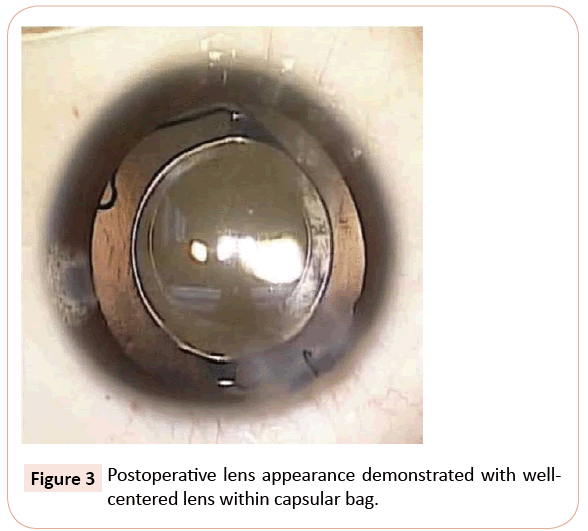
Figure 3: Postoperative lens appearance demonstrated with wellcentered lens within capsular bag./p>
The patient did extremely well and on post-operative day one presented with a quiet and clear left eye and uncorrected visual acuity of 20/25. Two months post-operatively, the eye was quiet with uncorrected visual acuity of 20/20. No posterior synechiae or iris captures were seen. The patient had no inflammation and was off topical steroids within 3 weeks of surgery.
Three months later, the cataract in the right eye had progressed with the child demonstrating difficulty with schoolwork. An identical procedure was performed on the right eye with a 23.0 diopter SN60WF lens. Postoperatively, the right eye also did well with 20/25 vision at day one uncorrected and a quiet anterior chamber. One month, postoperatively, the vision was 20/20 uncorrected in the right eye. The left eye maintained 20/20 visual acuity.
Discussion
The surgical difficulty of pediatric cataract extraction can be partially attributed to the increased elasticity of the lens [2]. The increased elasticity leads to a spiraling anteriorcapsule with an increased risk of radial tears and larger than needed capsular opening. Presently, most cases are performed utilizing the vitrector or forceps. Both methods may lead to unstable anterior capsule opening with a potential for posterior tears. This difficulty may produce unsatisfactory visual acuity and internal abberations as well as lens implant instability [3]. Although manual capsulorrhexis regardless of the method is possible and adequate, it is probably the most difficult step in a pediatric cataract procedure and critical for excellent life long excellent centration and lens stability.
Additionally, the decreased scleral rigidity leads to anterior capsular collapse and the necessity of small well executed corneal or scleral incisions [3]. Both of these factors demand greater surgical skill and produce increased risk of vitreous loss, poor lens centration or placement, postoperative inflammation, and astigmatism. Furthermore, the difficult lens centration, greater intraocular manipulation of the anterior capsule and scleral dissections in the manual technique increase the inflammatory response in children leading to high rates of posterior capsule opacification as well as immediate postoperative inflammation [3].
The advantages of the femtosecond laser play to all of the disadvantages of standard pediatric cataract surgery. The femtosecond laser can reduce internal aberrations and improve postoperative visual acuity [4]. Laser created capsulotomies have greater capsular stability and improve IOL centration compared to manual curvilinear capsulorrhexis [5]. Because pediatric cataract surgery with the LenSx® laser is an off label use, there are no parameter. The choice of the 3.8 mm opening was based solely on experience in this age group with their natural tendency to expand. The 3.8 mm capsule opening expanded significantly to make surgery and access to lens simple without allowing prolapse of lens into AC with hydrodissection. It should also be noted that lens fragmentation is not necessary since pediatric lenses are soft and aspirate easily with the phaco hand piece.
In addition, there appears to be improved corneal incisions and wound stability with the femtosecond laser [6]. Since the corneal incisions and capsulorrhexis are being created with a wellmaintained intraocular pressure and anterior chamber, collapse of the sclera or loss of control of the anterior capsular edge does not occur. The laser created corneal incisions prevents the need for scleral tunneling and allows for a controlled watertight incision, which should in turn lead to decreased risk of astigmatism and infection as indicated by this case. Lastly, the femtosecond laser assisted anterior capsulotomy has been shown to decrease the incidence of posterior capsule opacification [7]. This may be extremely beneficial in children who are more likely to develop posterior capsular opacification, which could delay further treatment with Nd:YAG laser capsulotomy until the child is older and more cooperative [10].
A few cases of pediatric femtosecond laser assisted cataract extraction have been published in Europe [8-9]. One case utilized the Catalys Precision Laser system (OpticaMedica, Acquired by Abbot Medical Optics) on a 10 year old boy with ectopia lentis due to Marfan syndrome [8]. Another case series utilized the same laser system on four infants under the age of nine months [9]. To the best of our knowledge, there have been no reported cases of pediatric cataract extraction in the United States and none with the LenSx® System.
There are a few features of our case that make it unique. First, it appears that this is the youngest case in which the LenSx® laser system was utilized. Despite the similarities between the systems, there are minor differences in imaging techniques and alogirthms [6]. Secondly, in accordance with guidelines; the posterior capsule was left intact [10]. Our patient was cooperative during examination and if opacification does occur, Nd:YAG laser could be employed [3]. Third, lateral canthotomy was not required because the LenSx interface is less rigid and more flexible than some of the other systems available and thus minimal adaptations need to be made in order to utilize this laser for pediatric cataracts.
Therefore, we believe that femtosecond lasers can and should be used in the pediatric cataract population. Given the difficulty of the manual capsulorrhexis, increased inflammation, scleral collapse and risk of posterior opacification, it seems that the pediatric cataract population would benefit greatly from this new technology. Nevertheless, benefits, intra-operative complications, and long-term complications cannot be fully analyzed until a robust clinical trial comparing femtosecond lasers with the standard care is undertaken in the pediatric population.
Acknowledgement
Special thanks to Polena Trust.
Financial Support
The authors did not receive grant or outside funding in support of their research or preparation of this manuscript. They did not receive payment or any benefits from commercial entities.
Conflicts of Interest
The authors were not compensated or funded in any way for the preparation of this manuscript. This study has not been submitted elsewhere. We understand and agree that if the manuscript is accepted for publication, copyright in the article, including the right to reproduce the article in all forms and media, shall be assigned to the publisher.
References
- Foster A, Gilbert C, Rahi J (1997) Epidemiology of cataract in childhood: a global perspective. J Cataract Refract Surg 23: 601-604.
- Wilson ME Jr (2004) Anterior lens capsule management in pediatric cataract surgery. Trans Am OphthalmolSoc 102: 391-422.
- Wilson ME, Buckley EG, Lambert SR, Plager DA, Bothun ED (2012)Cataract Surgery in Children: Trends and Controversies. 38th Annual Meeting of the American Association for Pediatric Ophthalmology and Strabismus, San Antonio, Texas.
- Miháltz K, Knorz MC, Alió JL, et al. (2011). Internal aberrations and optical quality after femtosecond laser anterior capsulotomy in cataract surgery. J Refract Surg27:711-716.
- Kránitz K, Takacs A, Miháltz K, Kovács I, Knorz MC,et al. (2011) Femtosecond laser capsulotomy and manual continuous curvilinear capsulorrhexis parameters and their effects on intraocular lens centration. J Refract Surg27:558-563.
- Nagy ZZ (2014) New technology update: femtosecond laser in cataract surgery. ClinOphthalmol 8: 1157-1167.
- Kovács I, Kránitz K, Sándor GL, Knorz MC, Donnenfeld ED, et al. (2014) The effect of femtosecond laser capsulotomy on the development of posterior capsule opacification. J Refract Surg 30: 154-158.
- Schultz T, Ezeanosike E, Dick HB (2013) Femtosecond laser-assisted cataract surgery in pediatric Marfan syndrome. J Refract Surg 29: 650-652.
- Dick HB, Schultz T (2013) Femtosecond laser-assisted cataract surgery in infants. J Cataract Refract Surg 39: 665-668.
- Vasavada AR, Praveen MR, Tassignon MJ, Shah SK, Vasavada VA, et al. (2011) Posterior capsule management in congenital cataract surgery. J Cataract Refract Surg 37: 173-193.

