Keywords
perception, pain, adolescent, sickle cell disease
Introduction
Sickle cell haemoglobinopathy shares the common feature of an abnormal globin chain which leads to sickling of
erythrocytes and obstruction of microcirculation (Jaussen, Garduer, Kirchhof, and Ryan, 2007). Sickle cell disease is
one of the most important haemoglobinopathies (Schnog, Duits, Muskiet, Cate, Rojer, and Brandjes, 2004) which
was first described in a Grenadian dental student in Chicago in 1910 (Serjearnt, 2005). Sickle cell disease is one of
the commonest hereditary diseases in the world. SCD have been acknowledged to have a global impact by the
World Health Organization (WHO). SCD comprises a group of inherited red blood cell conditions that result from
the synthesis of variant or mutant haemoglobin. Over 300,000 babies are born worldwide with SCD mostly in low and middle income countries, with the majority of these births in Africa. SCD originates in tropical regions as a
result of its advantage against malaria. It is predominant among people from African, Asian, Arabian and
Mediterranean countries; nonetheless it is a global health problem because of population migration. Sickle cell
disease affects millions of people throughout the world and it is particularly common in people of sub-Saharan
Africa origin (Creary, Williamson, and Kulkarni, 2007). In general about 25% of people of African origin carry the
sickle cell gene but only about 2-3% suffers from sickle cell disease. However in some parts of Africa sickle cell
disease is still often lethal in childhood. In Nigeria the prevalence of HbSS is 1-3% and it poses a severe burden on
the affected individuals and their families. Sickle cell disease commonly manifests itself as a painful crisis affecting
joints and limbs. Factors such as infection, dehydration, exhaustion and a change in temperature may precipitate this
crisis. There is a wide variation in the severity of pain, from mild transient attacks to severe pain of longer duration
with some patients requiring hospitalization. Even though life expectancy is on the rise for sickle cell disease
patients, it is still shorter than that of the general population (Schnog et al, 2004). Pain in sickle cell disease (SCD)
presents unique challenges for patients, families, and health care professionals. Pain is the most frequent problem
experienced by people with SCD. It has profound effects upon comfort and function in work, school, play and social
relationships (Shapiro, 2005). The frequency and severity of painful episodes are highly variable among patients.
Some patients have pain daily but others only occasionally. Painful episodes may start in the first year of life and
continue thereafter. The episodes last from hours to weeks followed by a return to baseline. Onset and resolution can
be sudden or gradual. Dehydration, infection, stress, fatigue, menses, and cold (including air conditioning and
swimming in cold water) can precipitate painful episodes (Serjeant et al, 2005). However, the majority of painful
episodes have no clear precipitant. Patients experience a wide variety of symptoms spanning acute and chronic pain
and assessment and management must be suitable for both. Because pain and SCD itself are lifelong problems that
have profound effects upon the quality of life, understanding of individual development and adopting a
biopsychosocial approach is crucial (Shapiro, 2004). The experience of pain varies with each developmental phase
and painful episodes are often termed "crises." Some people avoid the use of crises so that the major goal of
treatment will take the sense of catastrophe out of the crisis. However, replacing a word does not change
perceptions. The same is true for the strength, resilience, and vulnerability of each patient, as reflected in coping
skills, mood, social life, and function. Therefore this disorder is to be taking into consideration for proper prevention
and managements to reduce the effect the disease condition produce.
Purpose of study
1.To determine the perception of pain among adolescent with SCD.
2.To determine the perception on causes of pain among adolescent with SCD.
3.To determine the frequency of pain (crisis) and period in which pain occur most among adolescents with SCD
Hypotheses
1.There is no significant association between age and perception of pain among adolescents with sickle cell
diseases.
2.There is no significant association between perception and duration of pain among adolescents with sickle cell
disease.
3.There is no significant association between period of occurrence of pain and perception of pain among adolescents
with sickle cell disease.
Materials and Methods
A descriptive research design was used and the study was carried out in Sickle Cell Centre, Sir Gabriel Avenue,
Benin City, Edo State in 2010. The hospital is a tertiary institution that renders preventive, promotive-, curative and
rehabilitative health care services to clients with sickle cell disease. The target population comprised all adolescents
with genotype HbSS and HbSC who received in and out-patient care in the Sickle Cell Centre within the period of
study. Purposive sampling technique was used to select 80 adolescent with sickle cell crisis who were admitted or
seen within the period of study. Instrument for data collection was self developed questionnaire consisting of three
sections of 32-items question was used for data collection. Descriptive statistics in form of frequency and percentage
were used to summarize the data obtained; as well as inferential statistic in form of chi-square was used for testing
hypotheses generated at 5% level of significance. The purpose of the research and sections included in the
questionnaire were explained clearly in a simple language to the respondents. Anonymity and confidentiality of
individual subject was maintained. The parental or significant other consent as well as the respondents’ consents was
sought before including them in the study.
Results
Table 1 reported that respondents between the ages of 8-11years were 27.5%, 12-15years were 25.0% and 16-
19years were 47.5%. Majority were females. All the respondents were Christian and 90.0% accounted for student
while majority were in secondary school. Respondents were 25.0%, 16.3%, 22.5%, 23.8% and 12.5% with 1st, 2nd,
3rd, 4th, and others position in the family respectively.
Table 1: Demographic characteristics of respondents
Table 2 indicated that majority 67(83.8%) of the respondents opined excess exposure to cold can lead to pain while
13(16.3%) said no. Also majority of the respondent indicated that excess exposure to heat does not cause pain. The
highest number of respondents 67(83.8%) stated that pain can be caused by stress while 13(16.3%) stated otherwise.
Most 42(52.5%) agreed that prolong standing can result in pain crisis while 38(47.5%) did not. Majority 54(67.5%)
of the respondent don’t know if smoking can result in pain while 26(32.5%) said yes. The highest number of
respondents 60(75.0%) reported that poor diet can cause pain while 20 (25.0%) said no. 55(68.8%) indicated that
pain occur due to lack of drug compliance while 25 (31.3%) said no. The highest number of respondents 74(92.5%)
indicated that they have pain mostly in raining season.
Table 2: Respondents Perception On Causes Of Pain Crisis N=80
Table 3 shows majority of the respondent 35(43.8%) agreed that pain can be managed while 7(8.3%) strongly
disagreed. 38(47.5%) agree they can stay for weeks/months without pain crisis while 30(37.5%) strongly agree,
10(12.5%) disagree and 2(2.5%) strongly disagreed. Highest number of respondent 36(45.0%) agree that vigorous
exercise/stress increases pain and 24(30.0%), 10(12.5%) and 0(0.0%) strongly agreed, disagreed and strongly
disagree respectively. Majority of the respondent 48(60.0%) agreed that exposure to cold climate triggers pain crisis
while 3(3.8%) strongly disagree. 19(23.8%) of respondent both agree and strongly disagreed to pain crisis is like
having a minor injury while 16(20.0%) strongly agreed and 26(32.5%) disagreed. the highest number of respondent,
54(67.5%) agreed that pain is an emergency crisis in sickle cell disease. 17(21.3%) strongly agreed, and 9(11.3%)
disagreed
Table 3: Frequency distribution of perception of pain (crisis) n=80
Testing of Hypotheses
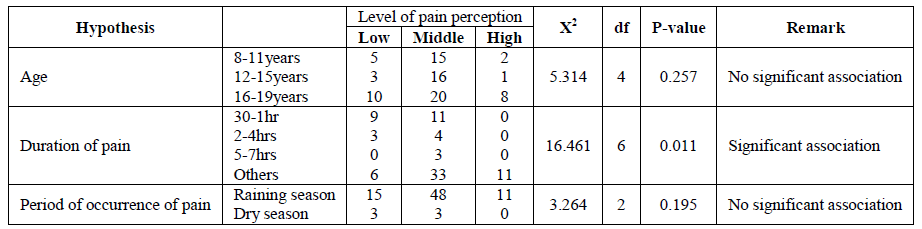
There was no significant association between age and perception of pain among adolescents with sickle cell diseases
under study with p>0.05. Also there was no significant association between period of occurrence of pain and
perception of pain among adolescents with sickle cell disease with p>0.05. However there was significant
association between duration of pain and perception of pain among adolescents with sickle cell disease under study
with p<0.05
Discussion
Majority of the respondent are female between the ages of 16-19 years and most of them were secondary school
student. Most of the respondents are either first or fourth position in the family. This study supports the fact relayed on how there is high incidence of occurrence of sickle cell disease among the children who are fourth born of the
family whose parent have a genotype AS. Most of the respondent perceived that malaria, stress, prolong standing,
poor diet lack of drug compliance and dehydration triggers pain (crisis) and strongly agreed that stress and excess
exposure to cold causes pain. This corroborates the report from Serjeant et al (2005) and Creary, et. al (2007), that
dehydration, infection, stress, fatigue, menses, cold (including air conditioning and swimming in cold water), and
malaria can precipitate painful episodes. However, Majority of the respondent don’t know if smoking can result in
pain crisis. Majority of the respondent reported that the duration of pain experienced is for over 24 hours in which
the occurrence is common in raining season than in dry season.
The study also revealed that there was no significant association between age and perception of pain among
adolescents with sickle cell diseases under study, despite the fact that there was increase perception with age. Also
there was no significant association between period of occurrence of pain and perception of pain among adolescents
with sickle cell disease with p>0.05. This implies that period of occurrence of pain does not influence pain
perception However; there was also significant association between duration of pain and perception of pain among
adolescents with sickle cell disease under study with p<0.05 and according to Serjeant et al, (2005) that the
frequency and severity of painful episodes are highly variable among patients. Some patients have pain daily but
others only occasionally. Painful episodes may start in the first year of life and continue thereafter. The episodes last
from hours to weeks followed by a return to baseline. Onset and resolution can be sudden or gradual.
Conclusion
From these finding, it is concluded that majority of the adolescent have average level of perception of pain. The
health care team should be aware that some of adolescent have low threshold to pain. Hence, Health care providers
have an important role to play in preventing, promoting, caring, counseling and health educating adolescents with
sickle cell disease especially during pain crisis.
Recommendations
Based on the findings discussed in this study, the following recommendations were made:
• The health care team should educate adolescents with sickle cell appropriately on prevention of pain with
emphasis on the prevention without the use of drugs.
• A program should be organized or it should be included when giving a health talk to sickle cell patient and
relatives on prevention of sickle cell crisis and encouragement should be given to them on the ways of promoting
health status.
• Emphasis should be paid on quick management of pain before it becomes a chronic pain which can cause
complication like organ dysfunction (kidney, brain) and ulceration of the leg.
References
- Ballas, S. Sickle Cell Pain: Progress in pain research and management. Seattle, Wash: IASP Press. 2004
- Creary, M., Williamson, D., and Kulkarni, R., J Womens Health (Larchmt) 2007, 16[5]:575-82
- Jaussen, A. M., Garduer, T. W., Kirchhof, B., and Ryan, S. J., Sickle cell retinopathy and haemoglobinopathies. Retinal vascular disease Springer Berlin Heidelberg 2007, 700-734.
- Makani, J., Williams, T. N., and Marsh, K., Ann Trop Med Parasitol 2007, 101[1]:3-14.
- McHugh, G., Thomas, G. Living with chronic pain: the patient's perspective. Nursing Standard 2001, 15: 52, 33-37.
- Schnog, J.B., Duits, A.J., Muskiet, F.A.J., and Cate, H.T. The Journal of Medicine 2004, 62[10]:364-374.
- Serjeant, G. R., Curr Opin Hematol 2005, 2:103-8.
- Shapiro, B., Dinges, D., Orne, E. Pain 2005, 61: 139-144.
- Smeltzer, S. C., Bare, B. G., Hinkle, J. L., Cheever, H. K., Brunner and Suddarth’s Textbook of Medical-Surgical Nursing [eleventh edition] Wolters Kluwer Health, Lippincott Williams and Wilkins [2008]
- Smith, J., Wethers, D. Health care maintenance. In: Embury, S., Hebbel, R., Mohandes, N., Steinberg, M. Sickle Cell Disease: Basic principles and clinical practice. New York, NY: Raven Press. 2004