Keywords
Exocrine Pancreatic Insufficiency; surgery
Abrreviations
EPI exocrine pancreatic insufficiency; PERT pancreas
enzyme replacement therapy
INTRODUCTION
In patients in which pancreatic acinar cells mass is
depleted there may be inadequate enzyme secretion
to the duodenum leading to malabsorption of ingested
carbohydrates, proteins, and lipids. This state of pancreatic
dysfunction is known as exocrine pancreatic insufficiency
(EPI).
In patients undergoing surgical management of their
pancreatic disease, EPI can arise either pre- or postoperatively.
In the pre-operative setting, EPI may be due to
parenchymal damage secondary to underlying pancreatic
disease as in the case of chronic pancreatitis, or as a result
of occlusion of the pancreatic duct as is seen in the case of
periampullary cancer [1, 2]. The principle aetiopathological
factor for post-operative EPI is resection of functional
pancreas parenchyma [3]. The effects of resection are
exacerbated when the remaining parenchyma is abnormal
such as in chronic or post-obstructive pancreatitis. In
addition, pancreatic and gastrointestinal reconstruction
resulting in dysregulation and asynchrony of enzyme
secretion is another hypothesis for EPI pathophysiology
that will also play an important role in the development
of EPI [4].
Retrospective observational studies report that EPI is a
common finding in the pre-operative setting, and that the
incidence of EPI increases post-operatively [5]. Patients
with EPI are classically said to present with weight-loss,
diarrhea or steatorrhea, however, these symptoms may
take weeks or months to manifest [6]. The importance
of identification of EPI and its treatment with PERT has
been highlighted in the recommendations of the National
Comprehensive Cancer Network (NCCN) that advocate
the immediate initiation of PERT in all patients presenting
with pancreatic cancer [7]. The relatively limited literature on this topic would indicate that few surgical patients
get worked up for EPI pre-operatively and only a small
fraction are prescribed PERT [8]. As such, patients may be
left without adequate pancreatic enzyme capacity during
the critical perioperative phase when nutrition is key, and
this can potentially reflect negatively on postoperative
outcomes [9, 10].
The aim of this survey was to assess the practices of
a defined population of pancreatic surgeons and gain
an insight into perioperative perception of EPI and its
management with PERT.
METHODS
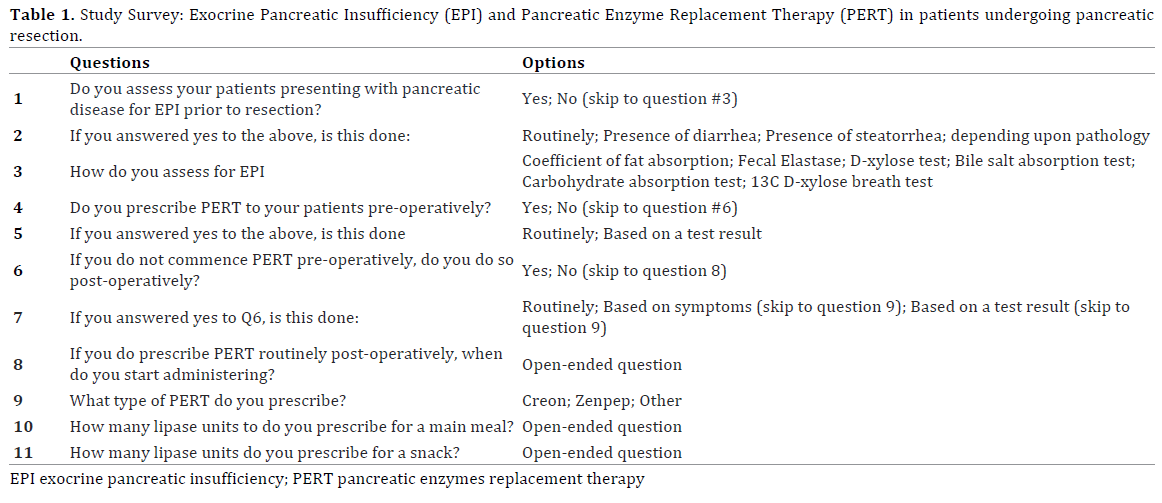
A cross-sectional online survey was created using tools
provided through “Surveymonkey.com”. The online survey
consisted of two sections evaluating surgeons’ perception
of EPI and practice of PERT prescription (Table 1).
Multiple choice and open-ended questions were used.
The questions covered perioperative aspects regarding
assessment of EPI and PERT practice: usage, dosing and
onset of prescription postoperatively.
The online survey link was sent to administrators
of “The Pancreas Club, Inc” and circulated by them to
members via their mailing-list service. The Pancreas Club
was founded in 1966 and has around 400 members. It is
an informal forum for pancreatic surgeons to exchange
their ideas and expertise in managing pancreatic disease
worldwide, with the predominance of members based in
the United States. We decided to use this venue for our
survey because it targets pancreatic surgeons interested
in pancreatic disease management.
RESULTS
A little over half of the respondents (52.5%) reported
assessing their patients for EPI preoperatively. Among
them, 48.5% did so routinely, the other 51.5% assessed
for EPI only in the presence of symptoms (diarrhea or
steatorrhea) or depending on the underlying pathology.
The preferred method of assessing for EPI was a
fecal elastase test (48%) followed by coefficient of fat
absorption (12%) then bile salt absorption test (2%).
A third of surgeons did not objectively test for EPI; they
relied on clinical symptoms to diagnose EPI.
Half of the surgeons reported having prescribed PERT
preoperatively to at least one patient previously. While
29.6% of them did that routinely, 70.4% required an
objective diagnosis through tests of their choice before
they did so. Among the other half who has never prescribed
PERT preoperatively, 92.6% considered prescribing it
postoperatively. However, only 40% routinely prescribed
PERT postoperatively; mostly to start with resumption of
per oral diet. The other 60% required either development
of clinical symptoms (52%) or an objective diagnosis of
EPI (8%) before placing patients on PERT.
Among PERT prescribers, 85.2% preferred to prescribe
Creon over the other available formulae. We did not find a
consensus on the quantity of lipase replacement units for
main meals. The replies ranged from 24,000 to 108,000
units while a few stated that they “do not know”. The
same was found with replacements prescribed for snacks,
ranging from 10,000 to 40,000 units.
DISCUSSION
This study identified that most surgeons do not assess
patients preoperatively for EPI. Review of the literature
revealed that the reported pre-operative prevalence of
EPI ranges widely; from 44% (range, 42%-47%) before
pancreatoduodenectomy (PD), to 20% (range, 16%-67%)
prior to distal pancreatectomy (DP). Post-operatively,
the incidence of EPI showed significant varaition from 74%
(range, 36%-100%) after PD to 19% to 80% after distal
pancreatectomy [3, 5]. Indeed, EPI might be markedly
under-reported in some series given the wide variation
in the published literature, and the low rates of active
assessment of patients for EPI pre-operatively that were
identified in the current study. The incidence of EPI is
widely reported to depend on underlying pathology and degree of pancreatic duct obstruction, with chronic
pancreatitis and pancreatic cancer being associated with
the highest incidences of EPI [3, 5]. More recently, Carr and
colleagues reported a high prevalence of EPI in patients
with IPMN, which is presumed to be due to viscous mucin
plugging the duct leading to an obstructive pancreatitis
[11].
Patients who go for surgery with an underlying
untreated EPI are believed to have worse outcomes;
reflected in an increase in morbidity and mortality. A
recent study by Roberts et al. in an analysis of 469 patients
undergoing PD noted that PERT was an independent
predictor of survival [12]. Of 469 patients evaluated, 202
(43.1%) had received PERT and on multivariable analysis
PERT had a Hazard ratio of 0.72 (95% CI: 0.52-0.99;
p = 0.044). Worsening malabsorption is believed to the
pivot of these inferior outcomes. [10, 13]
Whilst the practice is clearly not uniform in the
prescription evaluation of EPI and prescription of PERT,
the NCCN guidelines for the management of pancreatic
adenocarcinoma in the United States recommend all
patients be commenced of PERT regardless of symptoms
or testing [7]. Similar guidelines exist in the United
Kingdom and Australasia recommending the routine use
of PERT for malignant disease of the pancreatic head [14,
15]. It is encouraged that PERT be commenced at the time
of first diagnosis and recommenced as soon as patients
resume a solid diet post-operatively [3]. The importance
of commencing PERT immediately upon diagnosis is even
more relevant now given the trend towards neoadjuvant
therapy for both resec and borderline resec pancreatic
cancer as operations occur many months following
diagnosis, and if not treated patients will become severely
malnourished during this interval.
A large portion of responders who did consider a
pre-operative diagnosis of EPI required an objective
assessment before starting their patients on PERT. As
noted previously, for pancreatic cancer, the commonest
indication for pancreatic resection, the NCCN guidelines
state that the disease process is enough to justify treatment,
and that symptoms or a diagnostic test are not required
[7]. In terms of confirming a diagnosis, the coefficient of fat
absorption and bile salt absorption tests, although reliable
in diagnosing EPI, impose a significant burden on patients
as stool has to be collected over 3 days after being on a
high-fat diet for 5 days and are thus not routine used [5].
The fecal elastase-1 (FE-1) test is easier on patients given
that only one stool sample is required, and was the most
frequently utilised diagnostic test in this study. The major
limitation of FE-1 is that it does not detect early EPI [16].
Whilst a minority of surgeons reported using PERT
based on patient diagnosis, and others treated only based
on a diagnostic test, a significant number required the
presence of symptoms to initiate evaluation. This approach
may delay treatment for a number of patients as symptoms
such as diarrhea and steatorrhea take time to manifest in
EPI [17], and thus a window of opportunity to commence
PERT and enhance nutrition may be missed. There is also
evidence that patients may have EPI, confirmed by a low
FE-1 even prior to symptoms manifesting [18].
It is interesting to see that once surgery is performed
the hesitancy in assessing for EPI and starting patients on
PERT subsides. This can be attributed to, the now present,
tangible reason for developing EPI in the post-operative
setting, namely loss of pancreatic parenchyma. The other
explanation might be the presence of care pathways in
some practices or in an indirect way, a “grandfathered
practice in that setting”.
The choice of dosing is concerning. The responses
for quantifying main meal and snack lipase supplement
units fall within a broad range. This further backs up the
notion of uncertainty and no uniformity of practice. While
lipase supplements unit range reported by responders
spanned between 24,000 and 108,000 units for meals and
10,000 and 40,000 units for snacks, the recommended
dose is 72,000 units and 36,000, respectively [19]. Most
respondents under-dosed their patients at 24,000 for
meals. The timing of dosing in relation to meals is another
important issue that no repondent addressed in free text.
As an enzyme that depends on contact, PERT must be taken
immediately prior to meals, and when appropriately dosed,
1 capsule is taken prior to a meal and the second half way
through the meal. The inadequacy of dosing has previously
been reported by a Dutch national survey of patients with
chronic pancreatitis in which the majority of patients were
underdosed and 70% still reported steatorrhoea following
treatment [20].
Undertreating patients, by either not having them on
PERT or by under-dosing them, has been linked to early
and late postoperative complications. Early complications
through malnutrition results in poor wound healing,
diarrhea, dehydration and electrolyte imbalance.
This can prolong length of stay postoperatively and
result in readmissions. Long term complications from
malnutrition lead to weight loss and in the case of
pancreatic adenocarcinoma a poor prognosis in a
condition with an already low overall survival [12, 21,
22, 23, 24, 25].
The lack of a uniform policy would indicate that action
needs to be taken to standardize care of patients going for
pancreatic resection. There is a growing body of evidence
supporting this notion. Reviewing the literature to suggest
an optimal care pathway is beyond the scope of this
paper, however Philips et al. have proposed algorithms
for assessing EPI and managing PERT peri-operatively [3].
It is important to emphasize on the necessity of having a
team effort where patients, nurses, gastroenterologists,
pancreatic surgeons and dieticians organize themselves to
take on this issue [26, 27].
This study is limited by being a survey, and as such
the response rate would be expected to be low. Moreover,
although it is considered the optimal method for the
aim of this study, it has some inherited biases including selection and recall biases. Surgeons invited to participate
in the survey are all pancreatic surgeons, this raises a
high potential for selection bias as they are more likely
to manage pancreatic disease to the most up to date
standards available. Having said that, we find it alarming
that such high variation in practice exists even within a
highly selected group of specialized surgeons. Recall bias
can influence the results of studies based on surveys. We
do not think that it skewed our results. The nature of
the questions in our survey are independent on specific
incidences; they rather focus on patterns of practice.
The findings of this study cannot be generalized, yet, are
alarming enough for action to be taken to standardize care
and raise awareness between healthcare providers.
CONCLUSION
EPI is a manageable clinical condition that is
overlooked by healthcare providers who care for
pancreatic disease patients in the peri-operative period.
The presence of a pancreatic head neoplasm causing
ductal obstruction should guide surgeons to start PERT
empirically preoperatively as part of patient optimization
for surgery, and based on published national cancer
guidelines. For other patients undergoing resection, EPI
should be considered, with specific questioning of patients
and testing. Standardization of EPI management and PERT
is needed and can be done through collaborative efforts
through leaders and experts in pancreas disease.
An educational drive to increase peri-operative PERT
utilisation together with affirming appropriate dosing
regimens is warranted as improvements in peri-operative
nutritional may impact on both morbidity and mortality of
patients undergoing resection.
Conflict of Interest
The authors declare that they have no conflicts of interest.
References
- Nakamura H, Murakami Y, Uemura K, Hayashidani Y, Sudo T, Ohge
H, et al. Predictive factors for exocrine pancreatic insufficiency after
pancreatoduodenectomy with pancreaticogastrostomy. J Gastrointest
Surg 2009; 13:1321-7. [PMID: 19415402]
- Machicado JD, Chari ST, Timmons L, Tang G, Yadav D. A populationbased
evaluation of the natural history of chronic pancreatitis.
Pancreatology 2017. [PMID: 29221631]
- Phillips ME. Pancreatic exocrine insufficiency following pancreatic
resection. Pancreatology. 2015; 15:449-55. [PMID: 26145836]
- Sikkens EC, Cahen DL, de Wit J, Looman CW, van Eijck C, Bruno MJ. A
prospective assessment of the natural course of the exocrine pancreatic
function in patients with a pancreatic head tumor. J Clin Gastroenterol
2014; 48:e43-6. [PMID: 24717227]
- Tseng DS, Molenaar IQ, Besselink MG, van Eijck CH, Borel Rinkes
IH, van Santvoort HC. Pancreatic Exocrine Insufficiency in Patients with
Pancreatic or Periampullary Cancer: A Systematic Review. Pancreas
2016; 45:325-30. [PMID: 26495777]
- Lindkvist B. Diagnosis and treatment of pancreatic exocrine
insufficiency. World J Gastroenterol 2013; 19:7258-66. [PMID: 24259956]
- Tempero MA, Malafa MP, Al-Hawary M, Asbun H, Bain A, Behrman
SW, et al. Pancreatic Adenocarcinoma, Version 2.2017, NCCN Clinical
Practice Guidelines in Oncology. J Natl Compr Canc Netw 2017; 15:1028-
1061. [PMID: 28784865]
- Sikkens EC, Cahen DL, de Wit J, Looman CW, van Eijck C, Bruno MJ.
Prospective assessment of the influence of pancreatic cancer resection on
exocrine pancreatic function. Br J Surg 2014; 101:109-13. [PMID: 24338808]
- Crucitti F, Doglietto GB, Viola G, Frontera D, De Cosmo G, Sgadari A, et
al. Assessment of risk factors for pancreatic resection for cancer. World J
Surg 1998; 22:241-7. [PMID: 9494415]
- Kanda M, Fujii T, Kodera Y, Nagai S, Takeda S, Nakao A. Nutritional
predictors of postoperative outcome in pancreatic cancer. Br J Surg 2011;
98:268-74. [PMID: 20960457]
- Carr R, Kiel B, Roch A, Ceppa E, House M, Zyromski N, et al. Association
of pancreatic insufficiency with intraductal papillary mucions nesoplasm
dysplasia. HPB (Oxford) 2017; 19 (Suppl1):S64.
- Roberts KJ, Schrem H, Hodson J, Angelico R, Dasari BVM, Coldham
CA, et al. Pancreas exocrine replacement therapy is associated with
increased survival following pancreatoduodenectomy for periampullary
malignancy. HPB (Oxford) 2017; 19:859-867. [PMID: 28711377]
- Kyle UG, Pirlich M, Lochs H, Schuetz T, Pichard C. Increased length
of hospital stay in underweight and overweight patients at hospital
admission: a controlled population study. Clin Nutr 2005; 24:133-42.
[PMID: 15681111]
- Pancreatric Section, British Society of Gastroenterology; Pancreatic
Society of Great Britain and Ireland; Association of Upper Gastrointestinal
Surgeons of Great Britain and Ireland; Royal College of Pathologists;
Special Interest Group for Gastro-Intestinal Radiology. Guidelines for
the management of patients with pancreatic cancer periampullary and
ampullary carcinomas. Gut 2005; 54 Suppl 5:v1-16.
- Toouli J, Biankin AV, Oliver MR, Pearce CB, Wilson JS, Wray NH;
Australasian Pancreatic Club. Management of pancreatic exocrine
insufficiency: Australasian Pancreatic Club recommendations. Med J Aust
2010; 193:461-7. [PMID: 20955123]
- Leeds JS, Oppong K, Sanders DS. The role of fecal elastase-1 in
detecting exocrine pancreatic disease. Nat Rev Gastroenterol Hepatol
2011; 8:405-15. [PMID: 21629239]
- Li BR, Pan J, Du TT, Liao Z, Ye B, Zou WB, et al. Risk Factors for
Steatorrhea in Chronic Pancreatitis: A Cohort of 2,153 Patients. Sci Rep
2016; 6:21381. [PMID: 26877248]
- Hart PA, Conwell DL. Diagnosis of Exocrine Pancreatic Insufficiency.
Curr Treat Options Gastroenterol 2015; 13:347-53. [PMID: 26077487]
- Whitcomb DC, Lehman GA, Vasileva G, Malecka-Panas E, Gubergrits N,
Shen Y, et al. Pancrelipase delayed-release capsules (CREON) for exocrine
pancreatic insufficiency due to chronic pancreatitis or pancreatic surgery:
A double-blind randomized trial. Am J Gastroenterol 2010; 105:2276-86.
[PMID: 20502447]
- Sikkens EC, Cahen DL, van Eijck C, Kuipers EJ, Bruno MJ. Patients with
exocrine insufficiency due to chronic pancreatitis are undertreated: a
Dutch national survey. Pancreatology 2012; 12:71–73. [PMID: 22487479]
- Kahl S, Malfertheiner P. Exocrine and endocrine pancreatic
insufficiency after pancreatic surgery. Best Pract Res Clin Gastroenterol
2004; 18:947-55. [PMID: 15494288]
- Seiler CA, Wagner M, Bachmann T, Redaelli CA, Schmied B, Uhl W, et al.
Randomized clinical trial of pylorus-preserving duodenopancreatectomy
versus classical Whipple resection-long term results. Br J Surg 2005;
92:547-56. [PMID: 15800958]
- Crippa S, Bassi C, Warshaw AL, Falconi M, Partelli S, Thayer SP, et
al. Middle pancreatectomy: indications, short- and long-term operative
outcomes. Ann Surg 2007; 246:69-76. [PMID: 17592293]
- Chaudhary A, Negi SS, Masood S, Thombare M. Complications after
Frey's procedure for chronic pancreatitis. Am J Surg 2004; 188:277-81.
[PMID: 15450834]
- Falconi M, Mantovani W, Crippa S, Mascetta G, Salvia R, Pederzoli P.
Pancreatic insufficiency after different resections for benign tumours. Br
J Surg 2008; 95:85-91. [PMID: 18041022]
- Morrison M. Post-pancreatic resection: general overview and
unique complications. Dimens Crit Care Nurs 2010; 29:157-62.
[PMID: 20543614]
- Phillips M, Lordan JT, Menezes N, Karanjia ND. Feeding patients
following pancreaticoduodenectomy: a UK national survey. Ann R Coll
Surg Engl 2009; 91:385-8. [PMID: 19409147]

