Keywords
Clinical Trials, Phase I as Topic; Drug Therapy; Pancreatic Neoplasms; Radioimmunotherapy
Abbreviations
FOLFIRINOX, Folinic Acid, Fluorouracil, Irinotecan, Oxaliplatin; FOLFOX-A, Folinic Acid, Fluorouracil, Oxaliplatin, Abraxane
What Did We Know Before ASCO 2014?
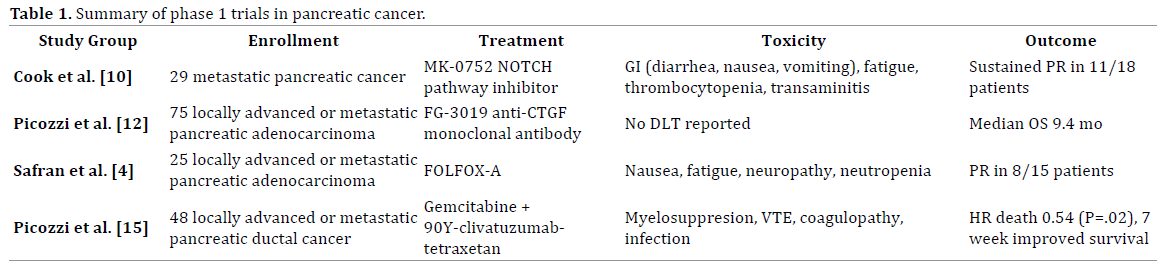
In the United States, pancreatic cancer remains the fourth leading cause of cancer death [1]. While surgery remains the only method of cure, the majority of patients present with unresectable or metastatic disease and a median survival of 8-14 months [2]. Given the low efficacy of current treatments today, investigation of novel therapeutic approaches is warranted. Here we discuss and summarize the results (Table 1) from four selected Phase I trials as presented at the 2014 Annual Meeting of American Society of Clinical Oncology (ASCO).
What Did We Learn at ASCO 2014?
Advances in Chemotherapy
Currently, most patients with locally advanced, unresectable or metastatic pancreatic cancer will receive gemcitabine-based chemotherapy or FOLFIRINOX. While FOLFIRINOX was superior to gemcitabine with longer overall survival, the regimen causes significant hematologic, GI, and neuropathic toxicity [3]. To mitigate these adverse effects which were largely attributed to irinotecan, Safran et al. conducted a phase I trial with 25 patients with locally advanced or metastatic pancreatic cancer where patients received up to 12 cycles of FOLFOX-A with increasing doses of nab-paclitaxel (Abraxane).After 6 cycles, patients without metastatic progression could have locoregional treatment [4]. Protein-bound paclitaxel previously showed improved survival in combination with gemcitabine monotherapy for pancreatic cancer [5], but its efficacy with FOLFOX is unclear. With FOLFOX-A, dose limiting toxicity included nausea and fatigue in 2 of 3 patients at 175mg/m2, and 90% of patients receiving ≥10 cycles of FOLFOX-A experienced grade 2-3 neuropathy. They identified a maximum tolerated dose of 150mg/m2 every 2 weeks with FOLFOX and report that a promising 53% of patients saw a partial response to this combination therapy [4].
Advances in Targeted Therapy
Successes such as imatinib and erlotinib in chronic myelogenous leukemia (CML) and non-small cell lung cancer respectively are prime examples of the enormous therapeutic potential of targeting molecular pathways in cancer. However, translating the current understanding of pathogenesis in pancreatic cancer into effective therapies continues to challenge investigators. Mutations in KRAS, p53, p16, and SMAD-4 drive carcinogenesis in pancreatic ductal cancer [6], but alternate aberrant pathways in pancreatic cancer may present additional drug targets. In addition, resistance to chemotherapy can occur by usurping pro-survival pathways [7-9]. Pancreatic cancer cells that develop resistance to gemcitabine have been found to be more “stem cell-like” with an increased activation of the NOTCH pathway [9]. This pathway can protect cancer cells from chemotherapy by inhibiting the apoptosis [7].
Cook et al. assessed the safety and tolerability of a gamma secretase inhibitor, MK-0752, that blocks the NOTCH pathway in 29 patients with metastatic pancreatic cancer. Patients were treated with concurrent gemcitabine and escalating doses of MK-0752 and evaluated for toxicities and tumor response. Patients tolerated the drug with acceptable GI toxicity including diarrhea, nausea, vomiting, in addition to fatigue, thrombocytopenia, and transaminitis. The investigators were able to reach the full single-agent doses for both gemcitabine and MK-0752 when given in combination without observing dose-limiting toxicity. In an evaluable 18 patients, 11 patients saw partial response at 12 weeks that was sustained to 38 weeks [10]. This is an intriguing result that warrants further investigation, particularly in the setting patients who initially respond to and tolerate gemcitabine well, but develop resistant disease.
FG-3019 is a human monoclonal antibody that has been promising in mouse models of pancreatic cancer by suppressing connective tissue growth factor (CTGF) which is activated in pancreatic adenocarcinoma [11]. Picozzi et al. conducted a phase I study of FG-3019 with gemcitabine and erlotinib in 75 patients with untreated Stage III-IV pancreatic cancer, assessing safety and clinical response. 52% of patients achieved stable disease with a partial response or complete responsein 14% of patients. The best survival was seen in patients with higher measurable plasma concentrations of circulating FG-3019 antibodies and with low baseline CTGF levels with a median OS 11.2 months with a 1-year OS of 42% [12]. This study cannot determine whether the correlation of CTGF levels and outcome are prognostic or predictive, however, it supports ongoing translational investigation of this novel growth factor.
Advances in Radioimmunotherapy
Exploitation of molecular targets also showed effect in preclinical studies using radioimmunotherapy (RAIT) for metastatic pancreatic cancer. Clivatizumab is a humanized monoclonal antibody specific to mucin produced by pancreatic ductal cancer that can be used to guide delivery of radioactive Yttrium-90 (90Y) specifically to pancreatic tumors and thereby induce tumor death. In animal models, gemcitabine enhanced treatment response when combined with RAIT [13]. Previously Ocean et al. demonstrated the tolerability of combined weekly gemcitabine with clivatizumab in a Phase 1 trial with 38 patients with Stage III-IV treatment-naïve pancreatic cancer in which median survival was 7.7 months [14]. In this Phase Ib study, Picozzi et al. randomized 48 patients with locally advanced or metastatic chemotherapy-refractory pancreatic cancer to receive weekly low radio sensitizing doses gemcitabine with 90Y-clivatuzumab-tetraxetan or 90Y-clivatuzumabtetraxetan alone. Transient myelosuppression limited dose escalation due to Grade 3-4 thrombocytopenia, neutropenia, and anemia. Patients also experienced venous thromboembolism, coagulopathy and infection.
Patients receiving combination therapy saw improved median OS (119 vs. 84 days, HR 0.54, CI 0.27-0.87, P=0.02). Observation is ongoing in 3 patients treated in the experimental arm now at 11-17 months [15].
The array of other targeted therapies being tested in ongoing Phase I trials in combination with existing chemotherapies include dasatinib, a BCR-ABL and SRC family tyrosine kinase inhibitor active in AML, CPI-613, an inhibitor of α-ketoglutarate dehydrogenase, and PF- 04136309, an immune-modulator.
Conclusions
These novel pursuits along with perpetual refinement of existing treatments may offer additional hope of prolonged survival with improved toxicity and quality of life for patients with pancreatic cancer.
Conflict of Interest
The authors have no potential conflicts of interest.
References
- Siegel R, Naishadham D, Jemal A. Cancer statistics. CA Cancer J Clin. 2012; 62(1): 10-29. [PMID:22237781]
- Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg. 1993; 165(1): 68-72; discussion 72-3. [PMID:8380315]
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, et al., FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011; 364(19): 1817-25. [PMID:21561347]
- Safran H, Charpentier K, Perez K, Mantripragada K, Austin TC, Nadeem O, Lombardo A, et al. Nab-paclitaxel (nab-P) combined with FOLFOX for advanced pancreatic cancer: A phase I study. J ClinOncol., 2014; 32:5s (suppl; abstr 4123).
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, Seayet T, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013; 369(18): 1691-703.
- Reid MD, Saka B, Balci S, Goldblum AS, Adsay NV. Molecular genetics of pancreatic neoplasms and their morphologic correlates: an update on recent advances and potential diagnostic applications. Am J ClinPathol. 2014; 141(2): 168-80. [PMID:24436263]
- Du X, Zhao YP, Zhang TP, Zhou L, Chen G, Wang TX, You L, et al., Alteration of the intrinsic apoptosis pathway is involved in Notch-induced chemoresistance to gemcitabine in pancreatic cancer. Arch Med Res. 2014; 45(1): 15-20. [PMID:24316112]
- Vaccaro V, Melisi D, Bria E, Cuppone F, Ciuffreda L, Pino MS, Gelibter A, et al., Emerging pathways and future targets for the molecular therapy of pancreatic cancer. Expert OpinTher Targets. 2011; 15(10): 1183-96. [PMID:21819318]
- Wang Z, Li Y, Kong D, Banerjee S, Ahmad A, Azmi AS, Ali S, et al. Acquisition of epithelial-mesenchymal transition phenotype of gemcitabine-resistant pancreatic cancer cells is linked with activation of the notch signaling pathway. Cancer Res. 2009; 69(6): 2400-7. [PMID:19276344]
- Cook N, Basu B, Smith DM, Gopinathan A, Evans TJ, Steward WP, Hagemannet T, et al. A phase I trial of the γ-secretase inhibitor (GSI) MK- 0752 in combination with gemcitabine in patients with pancreatic ductal adenocarcinoma (PDAC). J ClinOncol. 2014; 32:5s (suppl; abstr 4116).
- Aikawa T, Gunn J, Spong SM, Klaus SJ, Korc M, et al., Connective tissue growth factor-specific antibody attenuates tumor growth, metastasis, and angiogenesis in an orthotopic mouse model of pancreatic cancer. Mol Cancer Ther. 2006; 5(5): 1108-16. [PMID:16731742]
- Picozzi,VJ, Pipas JM, Koong A, Giaccia A, Bahary N, Krishnamurthi SS, Lopez CD, et al. FG-3019, a human monoclonal antibody to connective tissue growth factor (CTGF), with gemcitabine/erlotinib (G/E) in patients with locally advanced or metastatic pancreatic ductal adenocarcinoma (PDAC). J ClinOncol. 2014; 32:5s (suppl; abstr 4138).
- Gulec SA, Cohen SJ, Pennington KL, Zuckier LS, Hauke RJ, Horne H, Wegener WA, et al., Treatment of advanced pancreatic carcinoma with 90Y-Clivatuzumab Tetraxetan: a phase I single-dose escalation trial. Clin Cancer Res. 2011; 17(12): 4091-100. [PMID:21527562]
- Ocean AJ, Pennington KL, Guarino MJ, Sheikh A, Bekaii-Saab T, Serafini AN, Lee D, et al. Fractionated radioimmunotherapy with (90) Y-clivatuzumabtetraxetan and low-dose gemcitabine is active in advanced pancreatic cancer: A phase 1 trial. Cancer. 2012; 118(22): 5497-506.
- Picozzi VJ, Ramanathan RK, Lowery MA, Ocean AJ, Mitchell EP, O'Neil BH, Guarino MJ, et al. Feasibility and results of a randomized phase Ιb study of fractionated 90Υ-clivatuzumab tetraxetan in patients with metastatic pancreatic cancer having two or more prior therapies. J ClinOncol. 2014; 32: 5s (suppl; abstr 4026).

