Keywords
aprepitant; Cholangiopancreatography, Endoscopic Retrograde; Pancreatitis; Receptors, Neurokinin-1
INTRODUCTION
Acute pancreatitis can occur as a complication of endoscopic retrograde cholangiopancreatography (ERCP) in up to 40% of high risk patients [1, 2, 3, 4]. Established risk factors for acute pancreatitis include those that are patient related (e.g., young age, female gender, and sphincter of Oddi dysfunction) and those that are procedure related (e.g., difficult cannulation, pancreatic duct overinjection, and sphincterotomy). Potential mechanisms include sphincter of Oddi spasm and papillary edema from mechanical trauma, hydrostatic injury from saline or contrast, enzymatic injury, bacterial infection, and chemical injury from contrast medium [5, 6, 7, 8]. Although clinical trials have demonstrated the efficacy of prophylactic pancreatic duct stents at reducing the risk of post- ERCP pancreatitis, the absolute risk reduction is only about 10-15%. Furthermore, pancreatic duct stent placement itself is associated with complications such as migration, obstruction, bleeding, infection, perforation, and cholangitis [9, 10, 11].
A number of pharmacologic agents have been investigated for their potential to reduce the incidence of post-ERCP pancreatitis. Randomized trials have not consistently demonstrated the efficacy of pharmacologic prophylaxis and many of these agents are not available in the United States [12, 13, 14, 15, 16, 17, 18, 19, 20, 21]. Thus, there is a continued need for an agent that is both safe and effective at preventing post-ERCP pancreatitis, particularly in high risk patients.
Experimental models have supported the role of neurogenic inflammation (pathologic activation of sensory neurons) in the pathogenesis of acute pancreatitis. Activation of the capsaicin receptor (TRPV1) on sensory C and Aδ fibers induces the release of substance P, which is associated with pancreatic vasodilation, edema, and cellular infiltration [22, 23]. Substance P binds to the neurokinin-1 receptor in the pancreas to produce these features of neurogenic inflammation [24, 25]. In a rat model of post-ERCP pancreatitis, intra-ductal administration of a neurokin1 antagonist reduced the severity of inflammation [26].
Aprepitant is a selective neurokinin-1 receptor antagonist that is currently approved by the United States Food and Drug Administration (FDA) for prevention of chemotherapy-induced and postoperative nausea and vomiting [27, 28]. Aprepitant binds to neurokinin-1 receptors and would be expected to antagonize the actions of substance P throughout the body, including the pancreas [29].
We conducted a randomized, double-blind placebo controlled trial to investigate the efficacy of aprepitant at reducing the incidence of post-ERCP pancreatitis in high risk patients using the FDA approved dosage for management of chemotherapy induced nausea.
MATERIALS AND METHODS
Subject Selection
Eligible subjects were adults who were scheduled to undergo an ERCP procedure at Duke University Medical Center with risk factors that increased their probability of developing post-ERCP pancreatitis. Risk factors were specified a priori, and included age less than 60 years, female gender, prior history of post- ERCP pancreatitis, suspected sphincter of Oddi dysfunction, and patients expected to undergo a sphincterotomy. Exclusion criteria were patients with known adverse reaction to aprepitant, active pancreatitis at the time of the study, initiation of a drug known to cause pancreatitis within one month of enrollment, and inability to provide informed consent. Since aprepitant is categorized as a class B drug during pregnancy, we also excluded women who were pregnant, breastfeeding, or of child-bearing potential but not employing contraception.
Protocol
Simple randomization (parallel design) was used to separate subjects into treatment (aprepitant) and placebo arms. Subjects assigned to the treatment arm received oral aprepitant at the FDA approved dose based on phase III trials for chemotherapy induced nausea (125 mg oral aprepitant 4 hours prior to ERCP, 80 mg 24 hours after the first dose, and then 80 mg 24 hours after the second dose). Patients assigned to the placebo arm received biologically inactive pills that appeared identical to the study drug at the same intervals. Both treatment and placebo were stored in sequentially numbered bottles in order to ensure that patients, study personnel, and endoscopists were blinded to the group assigned. In order to allow for generalizability to clinical practice, the individual endoscopist was allowed to decide whether or not to place a prophylactic pancreatic duct stent.
After recovery from sedation immediately after the procedure, all patients were queried about symptoms of abdominal pain, nausea, or vomiting, as is standard practice at our institution. Serum amylase and lipase levels were obtained in patients with suggestive signs or symptoms. Among outpatients who developed symptoms immediately following the procedure, the decision to admit to the hospital versus discharge home were based on standardized protocols developed at our institution.
A study coordinator contacted all patients at 48 hours post-procedure, and 7 days post-procedure via telephone. The coordinator queried patients to determine if they developed any symptoms of pancreatitis at any time after the procedure and whether clinical care was sought for these symptoms. In symptomatic patients who sought medical attention, medical records were reviewed for all care rendered until discharge from the emergency department or hospital.
Definitions
Post ERCP pancreatitis was defined based on consensus criteria as abdominal pain that lasted at least 24 hours after the procedure, required inpatient admission, and was associated with amylase or lipase 3 or more times the upper limit of reference [1]. Severity of pancreatitis was also graded based on consensus criteria as mild (less than 4-day hospitalization), moderate (4-10-day hospitalization), or severe (more than 10-day hospitalization, intensive care unit admission, or complication requiring intervention such as pseudocyst, hemorrhage, or necrosis) [30].
ETHICS
The study was approved by the internal review board (IRB) at Duke University Medical Center, which requires studies to conform to the principles outlined by the Declaration of Helsinki. All subjects provided written consent prior to enrollment in the trial.
STATISTICS
All statistical analyses were performed using SAS Enterprise Guide (version 4.3; Cary, NC, USA). Baseline characteristics between the aprepitant and placebo group were compared using Fisher’s exact test for dichotomous, the Pearson chi-square for categorical variables, and the unpaired Student t-test for continuous variables. The primary end-point was presence or absence of pancreatitis up to 7 days postprocedure in the treatment and control arms, measured by Fisher’s exact test using an intention to treat analysis. Two-tailed P values less than 0.05 were considered significant.
RESULTS
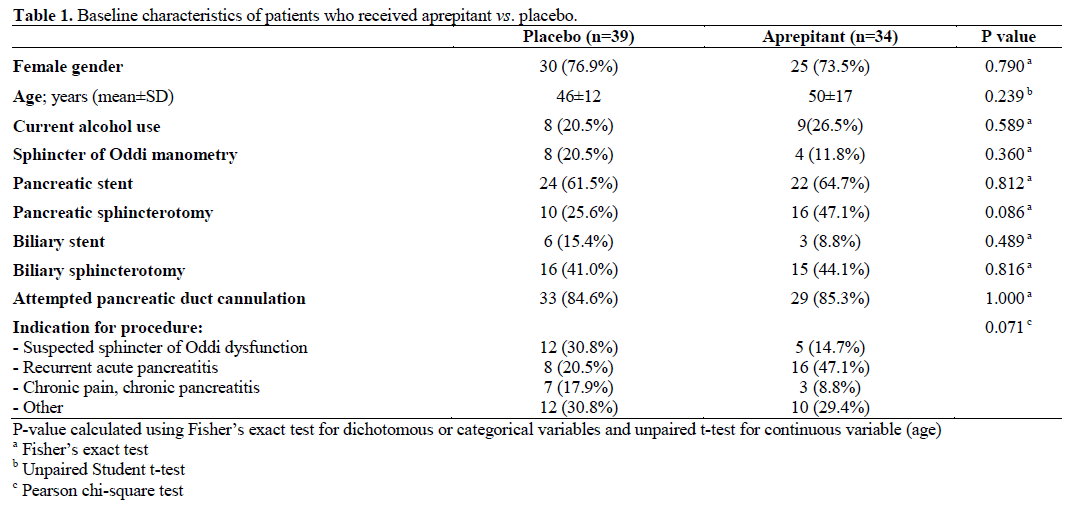
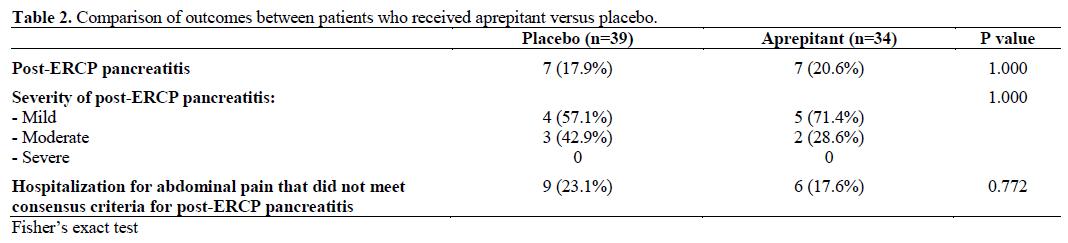
Patients were enrolled between August 2007 and October 2009. Among the 73 enrolled patients, 34 were assigned to the aprepitant arm and 39 patients were assigned to receive placebo (Figure 1). Baseline characteristics did not differ significantly between the two groups (Table 1), although there was a trend towards increased pancreatic sphincterotomy in the aprepitant group compared to the placebo group (16, 47.1% versus 10, 25.6%, respectively). Incidence of post-ERCP pancreatitis was 7 patients in the aprepitant group (20.6%) and 7 patients in the placebo group (17.9%). Incidence of hospitalization for abdominal pain that did not meet criteria for pancreatitis within 7 days post-procedure was 6 patients in the aprepitant arm (17.6%) and 9 patients in the placebo arm (23.1%). Neither of these outcomes differed significantly between the two groups (Table 2). No drug related toxicity was noted in the aprepitant group.
Figure 1. Patient enrollment and randomization.
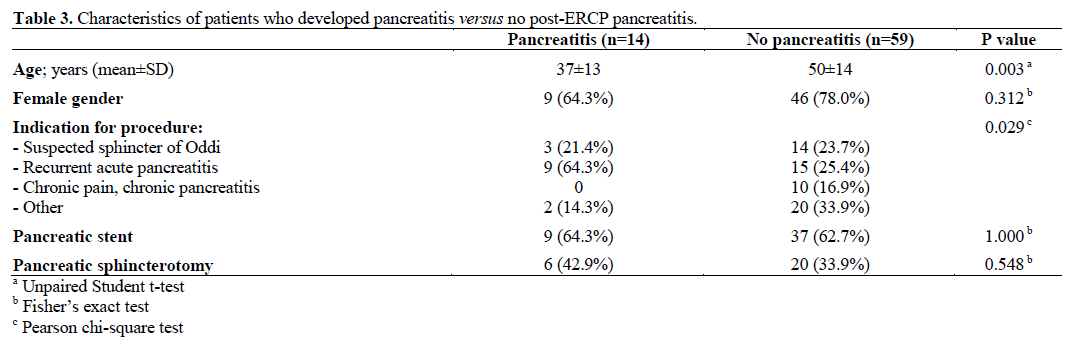
Given the lack of difference in outcomes between the aprepitant and placebo groups, we assessed for characteristics within our cohort that were associated with an increased probability of pancreatitis post hoc (Table 3). Mean age among patients who developed post-ERCP pancreatitis was 13 years younger than patients who did not develop post-ERCP pancreatitis. Indication for the procedure was recurrent acute pancreatitis in 64.3% of patients who developed post- ERCP pancreatitis but only 25.4% among patients who did not develop post-ERCP pancreatitis.
DISCUSSION
In our sample of high risk patients, overall odds of developing post-ERCP pancreatitis were 1 in 5, even in a high volume center (more than 1,000 procedures/year) and with routine placement of a prophylactic pancreatic stent in selected cases. These findings highlight the need to identify an agent that is both safe and effective at preventing post-ERCP pancreatitis. In this pilot study, aprepitant did not demonstrate efficacy at reducing the primary end point, which was the incidence of post-ERCP pancreatitis. None of the patients in our study developed severe post-ERCP pancreatitis, so the efficacy of aprepitant at reducing pancreatitis severity could not be assessed.
Substantial evidence from animal studies informed our decision to test a neurokinin-1 antagonist in human patients for prevention of post-ERCP pancreatitis [22, 23, 24]. An increase in both substance P and neurokinin-1 receptor expression has been demonstrated in experimentally induced necrotizing pancreatitis [24]. Pharmacological blockade of substance P receptor protected animals against pancreatitis [22, 23, 24], and genetic deletion of neurokinin-1 reduced severity of pancreatitis in knockout mice [31]. As evidence that neurogenic inflammation participates in ERCP-induced pancreatitis, Noble et al. demonstrated that addition of a TRPV1 blocker to contrast media reduced biochemical and histological features of pancreatitis produced by injection of contrast into the pancreatic duct in rats [32]. In human specimens, neurokinin-1 receptor expression has been shown to be up-regulated in nerves of patients with chronic pancreatitis [33].
To our knowledge, this study is the first to test the efficacy of a neurokinin-1 antagonist (aprepitant) at reducing incidence of post-ERCP pancreatitis in humans. The strengths of the study are the well-defined patient population and the randomized, double blind, placebo controlled design. However, these findings must be interpreted in context of the small sample size, which increases the likelihood of incorrectly accepting the null hypothesis of no difference. We estimate a larger trial would need to enroll 199 patients in each arm to provide a power of 80% at a two-sided significance level of 0.05 to detect a 10% absolute risk reduction in the incidence of post-ERCP pancreatitis from 20% to 10%. We elected to randomize patients using parallel rather than stratified allocation in this pilot trial so one of the baseline variables (pancreatic sphincterotomy) was more frequent in the aprepitant group, although this difference was not statistically significant. Given the small, sample size, we elected not to stratify patients based on specific risk factors or number of risk factors. The dose of aprepitant chosen for testing was based on that used clinically to treat nausea. However, we do not know if neurokinin-1 receptors on the pancreas were effectively blocked at this dose since we did not test higher doses of aprepitant.
One logistical challenge to patient enrollment was the requirement to administer the first oral dose 4 hours before the procedure. Since the time our study was initiated, the FDA has approved an intravenous formulation of aprepitant called fosaprepitant, which would be expected to achieve therapeutic blood levels when given within one hour of the procedure. Not only might this method of drug delivery offer more favorable pharmacokinetics, it also would be more convenient for drug administration in the endoscopy unit setting. It is likely that intravenous administration would facilitate enrollment of more patients.
In summary, aprepitant did not reduce the incidence of post-ERCP pancreatitis in this preliminary human trial. However, larger studies potentially using different doses of fosaprepitant and stratified allocation are required to conclusively assess the efficacy of neurokin-1 inhibition at preventing post-ERCP pancreatitis in humans.
Contributors
Merck Pharmaceuticals (Whitehouse Station, NJ, USA): materials and financial support; National Institutes of Health: T32 grant 5T32DK007568-21
Conflict of interests
The Authors have no potential conflict of interests
References
- Mallery, J.S., et al., Complications of ERCP. GastrointestEndosc, 2003. 57(6): p. 633-8.
- Freeman, M.L., et al., Complications of endoscopic biliary sphincterotomy. N Engl J Med, 1996. 335(13): p. 909-18.
- Loperfido, S., et al., Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. GastrointestEndosc, 1998. 48(1): p. 1-10.
- Andriulli, A., et al., Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol, 2007. 102(8): p. 1781-8.
- Akashi, R., et al., Mechanism of pancreatitis caused by ERCP. GastrointestEndosc, 2002. 55(1): p. 50-4.
- Cheon, Y.K., et al., Frequency and severity of post-ERCP pancreatitis correlated with extent of pancreatic ductal opacification. GastrointestEndosc, 2007. 65(3): p. 385-93.
- Pezzilli, R., et al., Mechanisms involved in the onset of post- ERCP pancreatitis. JOP, 2002. 3(6): p. 162-8.
- Raty, S., et al., Post-ERCP pancreatitis: reduction by routine antibiotics. J GastrointestSurg, 2001. 5(4): p. 339-45; discussion 345.
- Mazaki, T., H. Masuda, and T. Takayama, Prophylactic pancreatic stent placement and post-ERCP pancreatitis: a systematic review and meta-analysis. Endoscopy, 2010. 42(10): p. 842-53.
- Singh, P., et al., Does prophylactic pancreatic stent placement reduce the risk of post-ERCP acute pancreatitis? A meta-analysis of controlled trials. GastrointestEndosc, 2004. 60(4): p. 544-50.
- Sofuni, A., et al., Prophylaxis of post-endoscopic retrograde cholangiopancreatography pancreatitis by an endoscopic pancreatic spontaneous dislodgement stent. ClinGastroenterolHepatol, 2007. 5(11): p. 1339-46.
- Zheng, M., et al., Meta-analysis of prophylactic allopurinol use in post-endoscopic retrograde cholangiopancreatography pancreatitis. Pancreas, 2008. 37(3): p. 247-53.
- Rabenstein, T., et al., Low-molecular-weight heparin does not prevent acute post-ERCP pancreatitis. GastrointestEndosc, 2004. 59(6): p. 606-13.
- Kapetanos, D., et al., A randomized controlled trial of pentoxifylline for the prevention of post-ERCP pancreatitis. GastrointestEndosc, 2007. 66(3): p. 513-8.
- Bang, U.C., et al., Meta-analysis: Nitroglycerin for prevention of post-ERCP pancreatitis. Aliment PharmacolTher, 2009. 29(10): p. 1078-85.
- Chen, B., T. Fan, and C.H. Wang, A meta-analysis for the effect of prophylactic GTN on the incidence of post-ERCP pancreatitis and on the successful rate of cannulation of bile ducts. BMC Gastroenterol, 2010. 10: p. 85.
- Elmunzer, B.J., et al., A meta-analysis of rectal NSAIDs in the prevention of post-ERCP pancreatitis. Gut, 2008. 57(9): p. 1262-7.
- Dai, H.F., X.W. Wang, and K. Zhao, Role of nonsteroidalantiinflammatory drugs in the prevention of post-ERCP pancreatitis: a meta-analysis. HepatobiliaryPancreat Dis Int, 2009. 8(1): p. 11-6.
- Tsujino, T., T. Kawabe, and M. Omata, Antiproteases in preventing post-ERCP acute pancreatitis. JOP, 2007. 8(4 Suppl): p. 509-17.
- Jowell, P.S., et al., Intravenous synthetic secretin reduces the incidence of pancreatitis induced by endoscopic retrograde cholangiopancreatography. Pancreas, 2011. 40(4): p. 533-9.
- Andriulli, A., et al., Prophylactic administration of somatostatin or gabexate does not prevent pancreatitis after ERCP: an updated meta-analysis. GastrointestEndosc, 2007. 65(4): p. 624-32.
- Nathan, J.D., et al., Capsaicin vanilloid receptor-1 mediates substance P release in experimental pancreatitis. Am J PhysiolGastrointest Liver Physiol, 2001. 281(5): p. G1322-8.
- Nathan, J.D., et al., Primary sensory neurons: a common final pathway for inflammation in experimental pancreatitis in rats. Am J PhysiolGastrointest Liver Physiol, 2002. 283(4): p. G938-46.
- Bhatia, M., et al., Role of substance P and the neurokinin 1 receptor in acute pancreatitis and pancreatitis-associated lung injury. ProcNatlAcadSci U S A, 1998. 95(8): p. 4760-5.
- Baluk, P., et al., NK1 receptors mediate leukocyte adhesion in neurogenic inflammation in the rat trachea. Am J Physiol, 1995. 268(2 Pt 1): p. L263-9.
- He, Z.J., et al., Intraductal administration of an NK1 receptor antagonist attenuates the inflammatory response to retrograde infusion of radiological contrast in rats: implications for the pathogenesis and prevention of ERCP-induced pancreatitis. Pancreas, 2003. 27(1): p. e13-7.
- Jin, Y., et al., Efficacy and safety of aprepitant in the prevention of chemotherapy-induced nausea and vomiting: a pooled analysis. Support Care Cancer, 2011.
- Basch, E., et al., Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline Update. J ClinOncol, 2011.
- Hargreaves, R., et al., Development of aprepitant, the first neurokinin-1 receptor antagonist for the prevention of chemotherapyinduced nausea and vomiting. Ann N Y AcadSci, 2011. 1222: p. 40- 8.
- Cotton, P.B., et al., Endoscopic sphincterotomy complications and their management: an attempt at consensus. GastrointestEndosc, 1991. 37(3): p. 383-93.
- Liddle, R.A. and J.D. Nathan, Neurogenic inflammation and pancreatitis. Pancreatology, 2004. 4(6): p. 551-9; discussion 559-60.
- Noble, M.D., et al., A pH-sensitive, neurogenic pathway mediates disease severity in a model of post-ERCP pancreatitis. Gut, 2008. 57(11): p. 1566-71.
- Shrikhande, S.V., et al., NK-1 receptor gene expression is related to pain in chronic pancreatitis. Pain, 2001. 91(3): p. 209-17.


