Philip Joseph1, Ravish Sanghi Raju1, Frederick Lorence Vyas1, Anu Eapen2, Venkatramani Sitaram1
1Departments of General Surgery Unit IV (Hepato-Biliary Pancreatic Surgery)
2Radiodiagnosis, Christian Medical College. Vellore, Tamil Nadu, India
- *Corresponding Author:
- Philip Joseph
Department of General Surgery Unit IV
Ida Scudder Road, Vellore 632004
Tamil Nadu, India
Phone: + 91-416.228.3428
Fax: +91-416.223.2035
E-mail: pj1982@cmcvellore.ac.in
Received: 31 May 2010 Accepted: 17 June 2010
Context Portal annular pancreas is a rare congenital anomaly resulting from fusion of the pancreatic parenchyma around the portal vein/superior mesenteric vein. It is asymptomatic, but could have serious consequences during pancreatic surgery, if unrecognized. We describe a variant of this anomaly encountered during pancreaticoduodenectomy and propose a new classification. Case report We report a 51-year-old male who underwent a pancreaticoduodenectomy for periampullary carcinoma. After division of the pancreatic neck, a sheath of tissue was found posterior and extending to the left of the portal vein. When we divided this tissue, a large duct was encountered; this duct communicated with the main pancreatic duct. On review of the CT images, the main pancreatic duct was seen to be passing posterior to the portal vein and a smaller accessory pancreatic duct was present anterior to the portal vein. We describe the surgical implications. Conclusion This variant of portal annular pancreas has not yet been reported during pancreaticoduodenectomy and we propose a new classification for this fusion anomaly.
Keywords
Pancreas; Pancreatic Ducts /abnormalities; Portal Vein
INTRODUCTION
There are three types of pancreatic fusion anomalies: annular pancreas, pancreas divisum and portal annular pancreas. Portal annular pancreas is the rarest of these and is mostly asymptomatic. To our knowledge this variant has not yet been reported during pancreaticoduodenectomy. It could be significant during surgical resection and pancreaticojejunostomy.
CASE REPORT
A 51-year-old male presented with painless jaundice, generalized pruritus and loss of weight of 3 months duration. He was icteric. Abdominal examination revealed an enlarged liver with a palpable gallbladder. A liver function test showed conjugated hyperbilirubinemia. A chest X-ray was normal. A CT scan revealed bilateral intrahepatic biliary dilatation and a dilated main pancreatic duct. A side view gastroduodenoscopy showed an ulcerative lesion in the ampulla of Vater; the histological report was moderately differentiated adenocarcinoma.
He underwent a pancreaticoduodenectomy. On transecting the neck of the pancreas, there was a small duct (4 mm) on the cut surface anterior to the portal vein. While dividing the bulky uncinate process, which seemed to extend posteriorly and to the left of the portal vein, a dilated duct (10 mm) was encountered. This dilated duct was found to be continuous with the main pancreatic duct posterior to the portal vein. The anterior duct in the neck of the pancreas terminated a few centimeters within the body of the pancreas without communication with the main pancreatic duct. The large pancreatic duct encountered in the uncinate process resection was closed with interrupted 5/0 polypropylene sutures. The neck of the pancreas anterior to the portal vein was excised up to the dilated main pancreatic duct, well to the left of the portal vein. The main pancreatic duct was laid open and a side to side pancreaticojejunostomy was performed. The patient made an uneventful recovery from the surgery. A review of the CT scan showed the double ducts encircling the portal vein with the main pancreatic duct lying posteriorly to the portal vein (Figures 1, 2, 3 and 4).
Figure 1. White arrows demonstrating the dual pancreatic ducts
around the portal vein.
Figure 2. Main pancreatic duct dipping posteriorly to course around
the portal vein highlighted by white arrows.
Figure 3. White arrow showing the site of obstruction.
Figure 4. White arrows showing the pancreatic ducts on either side
of the portal vein.
DISCUSSION
During fetal development, the ventral pancreas rotates initially to the right (6 mm embryo stage) and then to the left about the axis of the primitive gut to fuse posteriorly with the dorsal pancreas (7 mm embryo stage). In rare instances, this fusion occurs to the left of the mesenteric/portal vein, thus encircling the portal vein. It is more common in the swine pancreas while it is rare in human beings [1]. An incidence of 1.14% has been reported by Karasaki et al., based on an institutional review of CT scans [2].
The possibility of this anomaly during pancreatic head resection was first described by Sugiura et al. [3]. Complete fusion of the uncinate process with the body of the pancreas was described by Hamanaka et al. during a resection of the pancreas [4].
In our patient, it was not only the uncinate process which had fused with the body of the pancreas, it was the entire ventral bud which had encased the portal vein and then joined the main pancreatic duct. To our knowledge, this variant of portal annular pancreas has not yet been described during pancreatic head resection. The surgical implication is that the main pancreatic duct which is posterior to the portal vein as well as the accessory duct anterior to the portal vein need to be drained into the intestine. Our solution was to suture the end of the main pancreatic duct posterior to the portal vein, excise the accessory duct and pancreatic neck, open the dilated main pancreatic duct to the left of the portal vein over the anterior surface of the body of the pancreas and do a side to side pancreaticojejunostomy. Our patient made an uneventful recovery, went on to receive chemotherapy and is on follow-up.
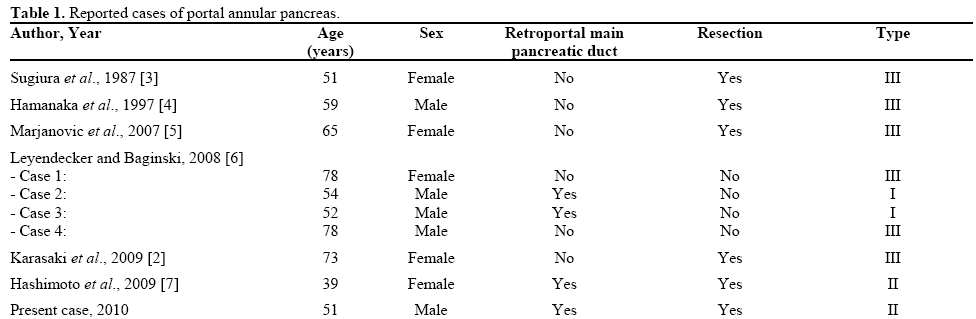
Portal annular pancreas may therefore be classified as type I when the ventral bud of the pancreas fuses with the body and ductal system of the pancreas posterior to the portal vein, type II when type I is associated with pancreas divisum (as it was in our patient) and type III when the uncinate process alone is involved in the encasement of the vessels and fusion. Each may be further divided into a, b and c (suprasplenic, infra- splenic and mixed) depending on its relationship to the splenic vein [2] (Figure 5). A CT scan is adequate for diagnosing this anomaly. In cases where the main pancreatic duct is not visible posterior to the portal vein, it can be diagnosed by demonstrating “continuity” of the extension of the uncinate process into the body of the pancreas in more than two slices on CT scan [2] (Table 1).
Figure 5. Schematic representation of the types of portal annular
pancreas.
Recognition of this anomaly pre-operatively will help avoid technical problems at the time of surgery.
Conflict of interest The authors have no potential conflict of interest
References
- Truty MJ, Smoot RL. Animal models in pancreatic surgery: a plea for pork. Pancreatology 2008; 8:546-50. [PMID 18824879]
- Karasaki H, Mizukami Y, Ishizaki A, Goto J, Yoshikawa D, Kino S, et al. Portal annular pancreas, a notable pancreatic malformation: Frequency, morphology, and implications for pancreatic surgery. Surgery 2009; 146:515-8. [PMID 19715809]
- Sugiura Y, Shima S, Yonekawa H, Yoshizumi Y, Ohtsuka H, Ogata T. The hypertrophic uncinate process of the pancreas wrapping the superior mesenteric vein and artery. Jpn J Surg 1987; 17:182-5. [PMID 3626212]
- Hamanaka Y, Evans J, Sagar G, Neoptolemos JP. Complete pancreatic encasement of the proximal hepatic portal vein: a previously undescribed congenital anomaly. Br J Surg 1997; 84:785. [PMID 9189086]
- Marjanovic G, Obermaier R, Benz S, Bley T, Juettner E, Hopt UT, Adam U. Complete pancreatic encasement of the portal vein: surgical implications of an extremely rare anomaly. Langenbecks Arch Sur 2007; 392:489-91. [PMID 17221270]
- Leyendecker JR, Baginski SG. Complete pancreatic encasement of the portal vein (circumportal pancreas): imaging findings and implications of a rare pancreatic anomaly. J Comput Assist Tomogr 2008; 32:61-4. [PMID 18303289]
- Hashimoto Y, Ross AS, Traverso LW. Circumportal pancreas with retroportal main pancreatic duct. Pancreas 2009; 38:713-5. [PMID 19629006]





