Keywords
Endosonography; Pancreatic Cyst; Pancreatic Neoplasms
INTRODUCTION
The evaluation and management of suspected pancreatic cystic neoplasms is increasingly controversial. The management of symptomatic cyst neoplasms is straightforward: resection when feasible, regardless of histologic subtype [1, 2, 3]. There has been a clear rise in incidental pancreatic cysts, now identified by imaging in approximately 1% of the population [3], but can be present in up to 24% of autopsy series [4]. The evaluation and management of incidental, asymptomatic, pancreatic cystic neoplasms continues to evolve [5, 6]. Some barriers to obtaining a consensus lies in not knowing the true incidence of mucinous lesions, and the preponderance of small unilocular cysts in asymptomatic patients that are difficult to characterize radiographically [7]. One approach to patients with an indeterminate, incidental, asymptomatic pancreatic cystic lesion is to guide therapy based on analysis of pancreatic cyst fluid [1, 7]. Numerous markers have been studied to predict the accuracy of the histologic subtype [7, 8, 9, 10, 11]. If this approach is to be successfully employed, it is important to analyze all variables in the cyst fluid which can increase the accuracy of predicting the histologic subtype. However, practical limitations due to cyst size and cyst location may combine to limit the aspirate volume. The potential limitation of cyst size is important when the reported incidence of potentially malignant lesions incidental cysts under 2 cm is 42% [12]. We report our experience with cyst aspiration to evaluate the clinically practical issues of how much fluid can be aspirated and analyzed based on cyst size and location.
METHODS
A prospective clinical protocol with database and treatment algorithm was instituted in January 1999. The database includes all patients evaluated either in General Surgery or Gastroenterology for a suspected pancreatic cystic neoplasm as previously described [1]. One purpose of this prospective study is to determine the natural history of observed patients, with the principle selection criterion being cyst fluid analysis in asymptomatic patients. Patients suspected to harbor a pancreatic pseudocyst based on a history of pancreatitis from a proximate cause were excluded. Demographic data collected included sex, age and symptoms (abdominal pain, weight loss, steatorrhea, and jaundice). The management algorithm principally segregates patients based on symptoms; all symptomatic patients are advised resection without aspiration. Resection is also advised for lesions with suspicious radiographic findings of a mucinous neoplasm including few, thick septations, peripheral calcifications and pancreatic duct dilation. All asymptomatic patients are advised to undergo cyst aspiration analysis regardless of pancreatic cyst size.
Pancreatic cyst aspiration was performed during endoscopic ultrasound (EUS). All endoscopic procedures were performed in the outpatient setting with conscious sedation using a linear-array ultrasound endoscope (GFUC 140P, Olympus Optical Co., Tokyo, Japan). EUS-guided cyst aspiration was performed with a 22-gauge needle (Echotip; Wilson-Cook, Winston-Salem, NC, USA). A maximum fluid volume was aspirated via one cyst puncture with the goal of complete evacuation of small cysts, and aliquots sequentially portioned for cytology, CEA (ng/mL), amylase (U/L), CA 15-3 (U/mL), viscosity, and CA 19-9 (ng/mL). A minimum of 1 mL was proportioned for cytology followed by minimum of 0.5 mL for each additional chemistry. Theoretically, considering the minimum amounts to perform the assays and even proportioning of cyst fluid, an absolute minimum of 2 mL is required for “complete”cyst analysis: cytology, CEA and amylase. Cytologic samples were processed by the ThinPrep method (Cytyc Corp, Boxborough, MA, USA) yielding one alcohol fixed slide. This slide was Pap stained, examined, and subsequently destained and restained with the Alcian blue/PAS stain for mucin. Thus, extracellular mucin staining is available for any cytology specimen without requiring any additional cyst fluid. Satisfactory cytology interpretation includes adequate slide preparation, cyst fluid with minimal contamination by gut mucosa as judged by an experienced cytopathologist blinded to the pathology of the resected specimen (Figure 1). The database included maximum cyst diameter by imaging, volume of cyst aspirate, cyst location (head, uncinate, body, or tail), and variables obtained from cyst analysis. For the purpose of this report, a “variable” included any satisfactory cytology interpretation, and/or any measured chemistry result whether CEA, amylase, CA 19-9, viscosity, or CA 15-3, since all variables were sought at the initiation of the protocol and were not preferentially partitioned in a standardized fashion. Immediate or delayed endoscopic complications were also recorded.
Figure 1. This Alcian blue/PAS stain highlights mucin
(center) within cyst contents. The mucin appears purple
due to the presence of both acidic and neutral mucin.
This specimen came from a mucinous cystadenoma.
ETHICS
The prospective protocol was approved by the Institutional Review Board. All patients were counciled on the risks, benefits and alternatives of endoscopic ultrasound with aspiration and voluntarily agreed to proceed.
STATISTICS
Scatterplots were used to display the relationships between cyst size and each of the number of variables and aspiration volume. The strength of relationships was measured using the Spearman rank correlation coefficient (rs). Cyst locations were compared with respect to the number of variables by using the Kruskal-Wallis test. The relationship between likelihood of aspiration success and cyst size was assessed using a logistic regression model with cyst size logtransformed (base 2), and the resulting model equation was used to estimate likelihood of success for various cyst sizes. A two-tailed significance level of 0.05 was used for all tests. Statistical analyses were performed using R version 2.3.1 (https://www.Rproject. org).
RESULTS
Over a six year period ending in December 2005, 370 patients entered the prospective protocol for evaluation of a suspected pancreatic cystic neoplasm. Thirteen patients had cysts in multiple locations (five patients had aspiration of more than one cyst) and 13 had an undetermined location. There were 243 women (65.7%) and 127 men (34.3%) with a mean age of 64 years (range: 23-93 years). The distribution of the 344 (93.0%) unilocular pancreatic cysts were in the head in 125 (36.3%), tail in 105 (30.5%), body in 77 (22.4%), and in the uncinate in 37 (10.8%).
Aspiration was not pursued in 53 patients (14.3%). Six of these patients were operated for symptomatic cysts and aspiration was judged to be unnecessary. The remaining 47 patients had asymptomatic cysts with a median size of 1.5 cm, and either declined an aspiration attempt, assumed to be endoscopically inaccessible or deemed a poor surgical risk as the principle reasons for lack of an aspiration attempt. An additional 31 patients (8.4%) underwent a EUS, but aspiration was unsuccessful, and no volume retrieved. The median cyst diameter was 1.5 cm (range: 0.5-8 cm) and the cysts were located in the head in 13 (41.9%), body in 3 (9.7%), tail in 8 (25.8%) and uncinate in 7 (22.6%).
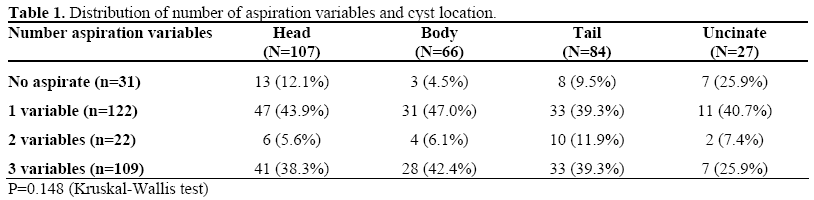
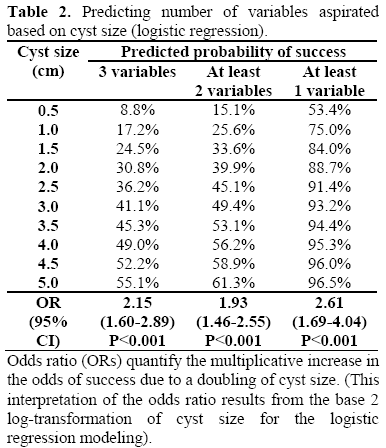
A total of 284 patients (76.8%) had cyst fluid aspirated and had available data regarding corresponding cyst size and location to compare with the aspiration results. The median cyst size for those aspirated was 2.0 cm (range: 0.3-17 cm). A total of 122 patients (43.0%) had one variable obtained (cytology plus/minus mucin, CEA, or amylase), 22 patients (7.7%) had two variables obtained, all three variables were obtained in 109 patients (38.4%); the additional 31 patients (10.9%) had zero variables obtained. Figure 2 plots the cyst size against number of variables obtained, and this demonstrates a positive correlation between size and number of variables aspirated (rs=0.31; P<0.001). The median cyst size was 2.2 cm for one variable, 2.2 cm for two variables, and 3.0 cm for three variables. Table 1 summarizes the variables determined by cyst location. The ability to obtain successful aspiration of multiple variables is independent of cyst location (P=0.148). The mean cyst volume aspirated was 8.3 mL (range: 0.5-250 mL) and this showed a significant positive relationship (rs=0.61; P<0.001) when plotting volume aspirated versus cyst size (Figure 3). Table 2 summarizes the data of logistic regression models predicting the success of aspiration of the number of variables based on cyst size. There was one endoscopic complication of a duodenal perforation requiring emergent exploration and duodenal repair for a serous cystadenoma of the pancreatic head that was not resected. Another patient had a duodenal wall hematoma that resolved without treatment or transfusion. There were no secondary infections of cysts, or pancreatitis.
Figure 2. Plot of cyst size (cm) vs. number of aspiration
variables (P<0.001; Spearman rank correlation).
Figure 3. Plot of aspiration volume (mL) by cyst size
(cm) (P<0.001; Spearman rank correlation).
DISCUSSION
The numerous asymptomatic cystic pancreatic lesions currently being discovered have created diagnostic and management dilemmas. Symptomatic lesions, or cysts with characteristic radiographic features of mucinous lesions should be managed with resection, and aspiration avoided. The suggested approach to asymptomatic incidentally discovered cystic lesions ranges from liberal resection [3, 5, 12] to observation [1, 13]. Knowing the correct approach is hampered by the inherent bias of retrospective surgical series, and the natural history of indeterminate and asymptomatic lesions which is currently poorly understood [6].
Aspiration of pancreatic cysts may have a pivotal role in patient management if several criteria are fulfilled. Cyst aspiration should be accurate in distinguishing histologic subtype, be safely performed and allow for obtaining all of the analyses sought. The goal of cyst aspiration is typically to distinguish mucinous histology form nonmucinous varieties. This presumes that asymptomatic individuals with a mucinous neoplasm will benefit definitively by resection if invasive carcinoma can be prevented. Numerous fluid aspiration variables have been analyzed with the most accurate results obtained for cyst fluid CEA and extracellular mucin [7, 9]. It is reasonable to assume that the combination of more than one aspiration variables will result in the most accurate interpretation of a given cyst. Our results indicated that EUS-guided aspiration can obtain fluid in 77% of patients and is independent of cyst location.
This study demonstrates a correlation between number of aspiration variables and cyst size. Our data allows us to estimate the number of variables likely to be obtained based on cyst size (refer to Table 2) which may assist the clinician in deciding whether to pursue an EUS-guided aspiration. For example, our data would indicate that the chance of an aspirate in a 2 cm cyst is 89% for obtaining at least one variable and 30% for obtaining all three variables. It is important to recognize that no fluid was aspirated in 9% with a median size of 1.5 cm which represents supportive data on which patients would not benefit from EUS or aspiration. It must then be decided what order the variables should be studied, and this may be equally problematic. Our sequence for testing is to obtain cytology with mucin staining followed by CEA, then amylase. This paradigm recognizes that the sensitivity of cytology for cyst fluid is low, but the specificity is high, and allows for studying extracellular mucin without obtaining any additional fluid [7, 14, 15, 16]. The assessment of extracellular mucin can be difficult with small cyst volumes, and we currently assess for the presence of acid mucin to help distinguish cyst mucin from gut contamination. In cysts with limited aspiration volume, we reserve the initial milliliter for this purpose, and additional 0.5 mL aliquots are proportioned for other studies. Thus, in the ideal situation where 2 mL of fluid is obtained and accurately proportioned, this would equate with complete evacuation of a 1.7 cm diameter cyst. The next variable in our algorithm is CEA measurement and its utility has been shown in a multi-institutional study for malignant and premalignant lesions [9]. We have advised resection for all mucinous lesions whether determined by aspirates with high CEA or presence of extracellular mucin, as neither result is completely accurate in our experience [1, 7]. An elevated amylase level in the cyst aspirate is associated with ductal communication which may be of some importance in distinguishing histologic subtype, or perhaps more useful for determining future treatment options, such as ablation therapy [17].
CONCLUSION
Indeterminate pancreatic cysts can be safely aspirated to achieve analysis of multiple variables. Successful aspiration is independent of cyst location, but correlates with cyst size. The chance of successful aspiration for multiple variables based on cyst size is predictable and useful in deciding which patients to aspirate. We currently do not recommend EUS or aspiration for cysts less than, or equal to, 1.5 cm.
Conflict of interest
The authors have no potential conflicts of interest
Acknowledgements
Supported by the generosity of James and Margaret Wilkes
References
- Walsh RM, Vogt DP, Henderson JM, Zuccaro G, Vargo J, Dumot J, et al. Natural history of indeterminate pancreatic cysts. Surgery 2005; 138:665- 70. [PMID 16269295]
- Hashimoto L, Walsh RM, Vogt D, et al. Presentation and management of cystic neoplasms of the pancreas. J Gastrointest Surg 1998; 2:504-8. [PMID 12000591]
- Spinelli KS, Fromwiller TE, Daniel RA, Kiely JM, Nakeeb A, Komorowski RA, et al. Cystic pancreatic neoplasms: observe or operate. Ann Surg 2004; 239:651-7. [PMID 15082969]
- Kimura W, Nagai H, Kuroda A, Muto T, Esaki Y. Analysis of small cystic lesions of the pancreas. Int J Pancreatol 1995; 18:197-206. [PMID 8708390]
- Goh BKP. Natural history of indeterminate pancreatic cysts. Surgery 2006; 39:856. [PMID 16782449]
- Walsh RM, Vogt DP, Henderson JM, Zuccaro G, Vargo J, Dumot J, et al. Natural history of indeterminate pancreatic cysts. Surgery 2005; 138:665- 70. [PMID 16269295]
- Walsh RM, Henderson JM, Vogt DP, Baker ME, O'malley CM Jr, Herts B, et al. Prospective preoperative determination of mucinous pancreatic cystic neoplasms. Surgery 2002; 132:628-33. [PMID 12407346]
- Brugge WR. Should all pancreatic cystic lesions be resected? Cyst-fluid analysis in the differential diagnosis of pancreatic cystic lesions: a meta-analysis. Gastrointest Endosc 2005; 62:390-1. [PMID 16111957]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology 2004; 126:1330-6. [PMID 15131794]
- Lewandrowski K, Lee J, Southern J, Centeno B, Warshaw A. Cyst fluid analysis in the differential diagnosis of pancreatic cysts: a new approach to the preoperative assessment of pancreatic cystic lesions. AJR Am J Roentgenol 1995; 164:815-9. [PMID 7537015]
- Fernández-del Castillo C, Alsfasser G, Targarona J, Brugge WR, Warshaw AL. Serum CA 19-9 in the management of cystic lesions of the pancreas. Pancreas 2006; 32:22. [PMID 16552345]
- Fernández-del Castillo C, Targarona J, Thayer SP, Rattner DW, Brugge WR, Warshaw AL. Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatic patients. Arch Surg 2003; 138:427-33. [PMID 12686529]
- Allen PJ, Jaques DP, D'Angelica M, Bowne WB, Conlon KC, Brennan MF. Cystic lesions of the pancreas: selection criteria for operative and nonoperative management of 209 patients. J Gastrointest Surg 2003; 7:970-7. [PMID 14675706]
- Ylagan LR, Edmundowicz S, Kasal K, Walsh D, Lu DW. Endoscopic ultrasound guided fine-needle aspiration cytology of pancreatic carcinoma: a 3-year experience and review of the literature. Cancer 2002; 96:362-9. [PMID 12478684]
- Centeno BA. Role of cytology in the diagnosis of cystic and intraductal papillary mucinous neoplasms. Gastrointest Endosc Clin N Am 2002; 12:697-708. [PMID 12607780]
- Recine M, Kaw M, Evans DB, Krishnamurthy S. Fine-needle aspiration cytology of mucinous tumors of the pancreas. Cancer 2004; 102:92-9. [PMID 15098253]
- Gan SI, Thompson CC, Lauwers GY, Bounds BC, Brugge WR. Ethanol lavage of pancreatic cystic lesions: initial pilot study. Gastrointest Endosc 2005; 61:746-52. [PMID 15855986]



