Keywords
Cholangiopancreatography, Magnetic Resonance; Pancreas; Pancreatic Ducts; Pancreatic Neoplasms
INTRODUCTION
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas is a unique clinical entity characterized by intraductal proliferation of mucin-producing epithelial cells that caused cystic dilatation of pancreatic duct [1], which was first reported by Ohhashi et al. [2]. It shows a wide spectrum of histological differentiation from lowgrade dysplasia, intermediate-grade dysplasia, high-grade dysplasia, which had been named non-invasive carcinoma, to invasive carcinoma [3]. According to the location of tumor, IPMN is classified into 2 types of main duct IPMN (MD-IPMN) and branch duct IPMN (BD-IPMN), which have been managed differently from each other by the guidelines published in 2006 [4]. Resection has been recommended to all MD-IPMNs because the average frequency of malignancy has been 70% and approximately two-thirds of them have been invasive. In contrast, in BD-IPMN, surgery has been recommended only to neoplasms that had higher likelihood of malignancy or caused symptoms on the ground of lower frequencies of malignancy and invasive carcinoma, which have been 25% and 15%, respectively. However, it was reported that when surgery was performed according to the guidelines, a considerable number of benign BD-IPMNs were resected [5-7]. In the guidelines revised in 2012, a new algorithm was proposed for the management of BDIPMNs in order to avoid unnecessary surgery [8]. However, the algorithm, which remains to be validated, was too complex to refer to in clinical practice. One of the reasons for the failure in identifying simple indicators of surgery may be a selection bias in numerous studies that examined resected BD-IPMNs exclusively in analyzing factors that may predict malignancy [9-15]. In the present study, using statistical methods, we attempted to identify predictors of malignancy in all BD-IPMNs including resected neoplasms and non-resected ones that were not submitted to surgery because of their lower likelihood of malignancy.
METHODS
Patients
Consecutive patients who were diagnosed to have BD-IPMNs at Osaka Medical Center for Cancer and Cardiovascular Diseases were enrolled. This study protocol was approved by the institutional review board of Osaka Medical Center for Cancer and Cardiovascular Diseases.
They underwent also ultrasound (US), endoscopic ultrasound (EUS), computed tomography (CT) or magnetic resonance cholangiopancreatography (MRCP). IPMN was identified by its typical features such as open orifice of the duodenal papilla, secretion of mucus, or filling defect in dilated main pancreatic duct (MPD) or cyst communicating with it. Cyst size and MPD diameter were measured by MRCP, and mural nodule size by US or EUS. All the patients underwent endoscopic retrograde pancreatography (ERP) and pancreatic juice was collected during the procedure using a duodenoscope (JF260, Olympus, Tokyo, Japan). After cannulation of a catheter into the main pancreatic duct, contrast medium was injected through the catheter to obtain a pancreatogram. A guidewire (0.025-inch Jagwire, Boston Scientific, Natick, MA, or 0.032-inch Radifocus, Terumo, Tokyo, Japan) was inserted through the catheter, which was further advanced into the main duct over the guidewire. After the guidewire was withdrawn, pancreatic juice was aspirated using syringes. All procedures were performed under fluoroscopic control. Pancreatic juice was centrifuged, cell pellets were smeared on several slide glasses, fixed in 95% ethanol, and stained by Papanicolaou’s method. The specimens were diagnosed as normal, atypical, suspicious, strongly suspicious, or malignant. Normal, atypical, suspicious, and strongly suspicious were considered as negative, and malignant as positive.
BD-IPMNs were defined as those that had mural nodules in dilated branch ducts. In addition, IPMNs without mural nodules were classified as BD-IPMN when their MPD diameters were <10mm and cyst sizes were more than three times as large as MPD diameters. Moreover, IPMNs without mural nodules were classified as BD-IPMN even though MPD diameters were ≥10mm when their cyst sizes were ≥30 mm and MPD dilated only at its vicinity.
Consequently, 202 patients with BD-IPMNs were enrolled. 35 patients underwent surgery and their BD-IPMNs were confirmed by histological examination. Low-grade and intermediate-grade dysplasia were classified as benign BDIPMN, and high-grade dysplasia and invasive carcinoma as malignant BD-IPMN. The remaining 167 patients who had BD-IPMNs in which mural nodules were absent or <10mm and cytology indicated benign neoplasms at the initial diagnosis. They were regarded as benign BD-IPMNs, because they had lower likelihood of malignancy at the initial diagnosis and did not increase in morphological parameters during follow-up by imaging examinations for 1 year.
ETHICS
This study protocol was approved by the institutional review board of Osaka Medical Center for Cancer and Cardiovascular Diseases. Written informed consent was obtained from all study patients.
STATISTICS
Statistical analysis was performed by software (SPSS II, IBM Corporation, Chicago, IL). Comparison of continuous data was performed by Mann-Whiteny’s U test and categorical data by chi square test. Receiver operating characteristic (ROC) curve was used to determine the optimal cutoff values for continuous data. Univariate analysis was performed by logistic regression model using factors which were shown to be significantly different between benign and malignant BD-IPMNs by Mann- Whiteny’s U test or chi square test. Multivariate analysis was further performed by logistic regression model using factors shown to be statistically significant by univariate analysis. A p-value less than 0.05 were considered to be statistically significant.
RESULTS
Background Characteristics of the Study Patients
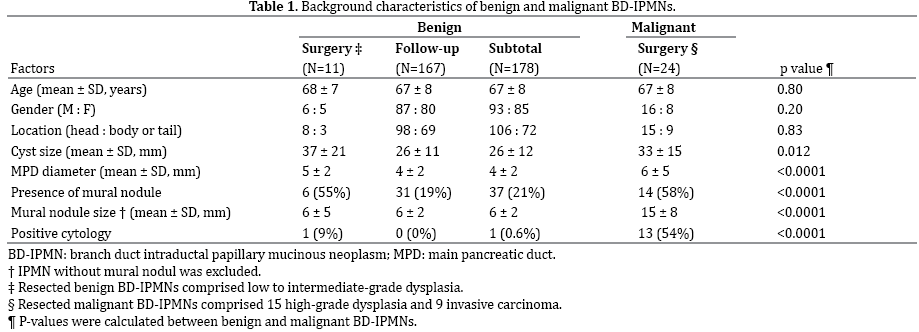
Background characteristics of 202 patients with BD-IPMNs were shown in Table 1. One hundred and seventy-eight benign BD-IPMNs comprised 11 confirmed by surgery and 167 diagnosed by imaging examinations and followup; 24 malignant BD-IPNMNs were confirmed by surgery. Resected BD-IPMNs comprised 11 low to intermediategrade dysplasia, 15 high-grade dysplasia, and 9 invasive carcinoma. Cyst size, MPD diameter, and mural nodule size were significantly greater in malignant BD-IPMNs than in benign neoplasms. Presence of mural nodule and positive cytology were significantly more frequent in malignant BD-IPMNs than in benign neoplasms.
Determination of Predictors of Malignancy
ROC curves that determined the cutoff values of cyst size, MPD diameter, and mural nodule size for discriminating benign from malignant BD-IPMNs were shown in Figure 1. Optimal cutoff values of cyst size, MPD diameter, and mural nodule size were determined as 30 mm, 6 mm, and 10 mm, respectively.
Figure 1. Receiver operating characteristic (ROC) curve was drawn to
determine the optimal cutoff values for cyst size, main pancreatic duct
(MPD) diameter, and nodule size. Area under the ROC curve for cyst size,
MPD diameter, and nodule size were 0.64, 0.63, and 0.74, respectively.
The optimal cutoff values for cyst size, MPD diameter, and nodule size
were determined as 30 mm, 6 mm, and 10 mm, respectively.
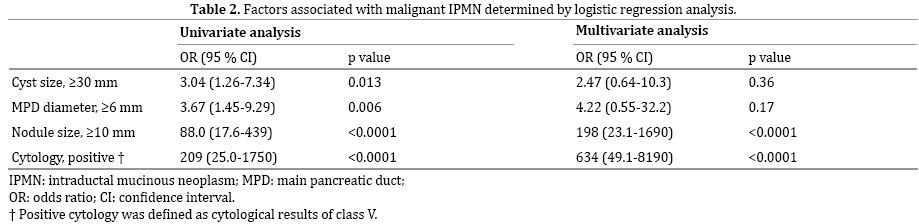
Univariate analysis by logistic regression model showed that cyst ≥30 mm, MPD diameter ≥6 mm, mural nodule ≥10 mm, and positive cytology were predictors of malignancy in BD-IPMN (Table 2). Multivariate analysis by logistic regression model showed that mural nodule ≥10 mm (OR 198, 95% CI 23.1-1690, p<0.0001) and positive cytology (OR 634, 95% CI 49.1-8190, p<0.0001) were independent predictors of malignancy in BD-IPMN.
Diagnostic Accuracies of Mural Nodule Size and Cytology
Diagnostic accuracies of mural nodule size and cytology were shown in Table 3. Sensitivity, specificity, and overall accuracy of mural nodule size ≥10 mm were 50%, 99%, and 93%, respectively. Those of positive cytology were 54%, 99%, and 94%, respectively. When BD-IPMNs with mural nodules ≥10 mm or positive cytology were diagnosed to be malignant, those were 88%, 98%, and 97%, respectively.

DISCUSSION
In the present study, mural nodule size ≥10 mm and positive cytology were demonstrated to be independent predictors of malignancy in BD-IPMN. These predictors were identified by examining all BD-IPMNs including resected neoplasms and non-resected ones that were not submitted to surgery because of their lower likelihood of malignancy. This was quite consistent with our recent suggestion that mural nodule ≥10 mm and positive cytology might be indicators of surgery during follow-up of BD-IPMNs with lower likelihood of malignancy [16]. Sensitivity and specificity for malignancy were 88% and 98%, respectively, when BD-IPMNs with either of these predictors were diagnosed to be malignant.
The original guidelines for the management of IPMN recommended surgery to BD-IPMNs that had cyst ≥30 mm, MPD ≥6 mm, mural nodule, positive cytology, or symptoms on the ground of 8 surgical series describing their lower frequencies of malignancy and invasive carcinoma, which have been 25% and 15% in average, respectively [4]; however, not a few benign BD-IPMNs were resected when surgery was performed according to the guidelines [5-7]. In the revised guidelines, a new algorithm for the management of BD-IPMNs was proposed in order to avoid unnecessary surgery [8]. Resection was recommended to BD-IPMNs with “high risk stigmata” of bile duct obstruction, enhancing solid component, or MPD ≥10 mm. In addition, resection was recommended to BD-IPMNs with “worrisome features” of cyst size ≥30 mm, thickened or enhancing cyst walls, non-enhancing mural nodule, or abrupt change in caliber of pancreatic duct with distal pancreatic atrophy, if they had definite mural nodule, MPD features suspicious for involvement, or cytologically suspicious or positive results for malignancy. However, these criteria, which remain to be validated, are rather complex in clinical practice.
Most studies that aimed to identify predictor of malignancy in BD-IPMN have been performed by examining resected neoplasms exclusively [9-15]. Result of analysis including only resected BD-IPMNs with higher likelihood of malignancy and excluding neoplasms for which surgery was not indicated because of their lower likelihood of malignancy may have been distorted by selection bias. This may have been one of the reasons why simple predictors of malignancy in BD-IPMN have not been identified. The present study which included not only resected BD-IPMNs but also non-resected neoplasms with lower likelihood of malignancy was free from the selection bias which most previous studies could not escape. BDIPMNs in which mural nodules were absent or <10 mm and cytology indicated benign neoplasms at baseline, and remained unchanged in imaging parameters for 1 year were included in the present study by regarding them as benign neoplasms.
Morphological predictors of malignancy in BD-IPMNs were cyst size ≥30 mm [7, 9, 12], dilatation of MPD [10, 14], and presence of mural nodule [7, 9-13, 15]. Consistently, a very recent meta-analysis showed that these 3 factors were their indicators of malignancy (17). In the present study, analysis was performed using ROC curve in order to determine the cyst size, MPD diameter, and mural nodule size that could discriminate malignant from benign BD-IPMNs (Figure 2). Subsequent univariate and multivariate analysis by factors including these parameters showed that mural nodule size ≥10mm was the only predictor of malignancy except positive cytology of pancreatic juice. Presence of mural nodule was a strong indicator of malignancy in BD-IMMN [7, 9-13, 15], but their sizes have not been considered. In discrimination of malignant and benign BD-IPMNs, their sizes have to be taken into consideration, because IPMNs with larger nodules were shown likely to be malignant in a few studies that did not examine MD-IPMNs and BDIPMNs separately [17-22]. Recently, by investigating BDIPMNs exclusively, it was shown that the mural nodule sizes were significantly greater in malignant neoplasms than in benign ones (16.4 mm vs. 4.3 mm) [23]. In addition, it was reported that using cut off values of 5 mm and 7 mm, sensitivities and specificities for malignancy in BD-IPMN were 73% and 80%, 86% and 100%, respectively [24, 25].

Figure 2. A representative case of malignant IPMN with nodule size
of ≥10 mm in size and negative cytology. (a). Magnetic resonance
pancreatography (MRP) showed a cyst of 15 mm in size at the pancreatic
body and the diffuse dilated main pancreatic duct . (b). Endoscopic
retrograde pancreatography (ERP) showed a filling defect in the cyst and
peri-cystic area which indicated presence of mucus. Tip of the catheter
used for aspiration of pancreatic juice was inserted into the cyst. (c,d).
CT and endoscopic ultrasound showed a mural nodule of 15 mm in size
inside the cyst. (e). Microscopic examination of pancreatic juice revealed
hyperplastic cells which were classified into class II (Papanicolaou’s
stain). Despite negative cytological result, the patient underwent surgery
because of mural nodule of ≥10 mm in size. (f). Final diagnosis was
determined as non-invasive intraductal papillary mucinous carcinoma
by microscopic examination of the resected specimens. A mural nodule
consisted of carcinomatous epithelia was observed inside the cyst at the
pancreatic body.
A low sensitivity of 50% and a high specificity of 99% in the present study indicated that a substantial number of malignant BD-IPMNs had mural nodules <10 mm and few benign BD-IPMNs had mural nodules ≥10 mm. Moreover, because not a few malignant BD-IPMNs lacked mural nodule [22], discrimination of malignant from benign neoplasms by setting a cut off value is limited in accuracy. In order not to miss malignant BD-IPMNs in selecting candidate for surgery, another predictor of malignancy should be considered.
Another test for predicting malignancy in IPMN is cytologic examination of pancreatic juice. We had reported for the first time that pancreatic juice cytology was a predictor of malignancy in IPMN, when it was called mucin producing tumor of the pancreas [26]. However, later investigations could not reproduce a promising result like ours [27] but yielded only low sensitivities for malignancy, where calculation was performed in all IPMNs including MD-IPMNs and BD-IPMNs [10, 28]. In contrast, studies that calculated sensitivities of cytology individually in MD-IPMNs and BD-IPMNs yielded higher sensitivities in the former and lower ones in the latter [24, 29, 30]. Especially, Yamaguchi reported a high sensitivity of 80% in MD-IPMNs by collecting materials directly using peroral pancreatoscopy, which was a procedure similar to ours that had been published [27], and a low sensitivity of 42% chiefly in BD-IPMNs using catheter alone [30]. Results of these reports indicated that higher sensitivities of pancreatic juice cytology were yielded only by acquiring specimens directly from the neoplasms in MPD, whereas lower sensitivities were produced because malignant cells were not aspirated directly but sampled using a catheter placed in MPD that communicated with dilated branch ducts harboring neoplasm. In order to improve the diagnostic accuracy of pancreatic juice cytology in BD-IPMNs, it is important to obtain a sufficient volume of mucous pancreatic juice and to identify a few malignant cells among a vast majority of benign adenomatous cells in the specimen [26]. In the present study, significance of cytology was the identification of malignant BD-IPMNs that was not detected by mural nodule size ≥10 mm. A sensitivity of 50% by mural nodule size alone increased to 88% without lowering specificity by diagnosing BD-IPMNs with mural nodules <10 mm as malignant when they had positive results of cytology. Despite its low sensitivities reported, one of the predictors of malignancy in BD-IPMN is positive cytology in pancreatic juice [13, 29, 31], which is recommended in its management (Figure 3).
Figure 3. A representative case of malignant IPMN without mural
nodule and positive cytology. (a). MRP showed a cyst of 16 mm in size
at the pancreatic body. (b). ERP showed the MPD without dilation. (c,d).
Mural nodule was not detected inside the cyst by CT and ultrasound. E).
Microscopic examination of pancreatic juice revealed adenocarcinoma
(Papanicolaou’s stain,). The patient underwent surgery because of
positive cytology. (f). Final diagnosis was determined as non-invasive
intraductal papillary mucinous carcinoma by microscopic examination of
the resected specimens. Carcinomatous epithelia showing low- papillary
architecture were observed along the cystic wall at the pancreatic body.
Limitation of the present study is its single center and retrospective nature. In addition, prospective multicenter study is necessary to validate our indication for surgery. Moreover, as mentioned above, analysis was performed by including not only resected BD-IPMNs but also neoplasms that were not resected because of their lower likelihood of malignancy without establishment of histological diagnosis. Few of them may be malignant, because they had lower likelihood of malignancy at the initial diagnosis and remained unchanged on imaging parameters during follow-up for 1 year.
In conclusion, simple predictors of malignancy in BD-IPMN were identified in the present study. They were mural nodule ≥10 mm and positive cytology. When BD-IPMNs that had either of the indicators were diagnosed to be malignant, sensitivities and specificities for malignancy were 88% and 98%, respectively. It is expected that the indication of surgery for BD-IPMNs should be simplified in the guidelines.
Conflict of Interest
The authors declare no conflict of interest.
References
- Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Saavedra J, Biankin AV, Biankin SA, Compton C, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia (PanIN) and intraductal papillary mucinous neoplasms (IPMNs). Am J Surg Pathol. 2004; 28: 977-987. [PMID: 15252303]
- Ohhashi K, Murakami Y, Maruyama M. Four cases of mucous secreting pancreatic cancer [in Japanese]
- Prog Dig Endosc. 1982; 20: 348-351. Adsay NV, Kloppel G, Fukushima N, et al. Intraductal neoplasms of the pancreas. In: World Health Organization classification of tumours of the digestive system. 2010; 304-310.
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, Yamaguchi K, Yamao K, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006; 6:17–32. [PMID: 16327281]
- Pelaez-Luna M, Chari ST, Smyrk TC, Takahashi N, Clain JE, Levy MJ, Pearson RK, et al. Do consensus indications for resection in branch duct intraductal papillary mucinous neoplasm predict malignancy? A study of 147 patients. Am J Gastroenterol. 2007; 102:1759–1764. [PMID: 17686073]
- Tang RS, Weinberg B, Dawson DW, Reber H, Hines OJ, Tomlinson JS, Chaudhari V, Raman S, Farrell JJ. Evaluation of the guidelines for management of pancreatic branch-duct intraductal papillary mucinous neoplasm. Clin Gastroenterol Hepatol. 2008; 6: 815-819. [PMID: 18602036]
- Woo SM, Ryu JK, Lee SH, Yoon WJ, Kim YT, Yoon YB. Branch duct intraductal papillary mucinous neoplasms in a retrospective series of 190 patients. Br J Surg. 2009; 96: 405–411. [PMID: 19283746]
- Tanaka M, Fernandez-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, Kimura W, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology. 2012; 12: 183–197. [PMID: 22687371]
- Sugiyama M, Izumisato Y, Abe N, Masaki T, Mori T, Atomi Y. Predictive factors for malignancy in intraductal papillary-mucinous tumors of the pancreas. Br J Surg. 2003; 90: 1244- 1249. [PMID: 14515294]
- Serikawa M, Sasaki T, Fujimoto Y, Kuwahara K, Chayama K. Management of intraductal papillary- mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol. 2006; 40: 856-862. [PMID: 17016145]
- Schmidt CM, White PB, Waters JA, Yiannoutsos CT, Cummings OW, Baker M, Howard TJ, et al. Intraductal papillary mucinous neoplasms. Predictors of malignant and invasive pathology. Ann Surg. 2007; 246: 644-654. [PMID: 17893501]
- Rodriguez JR, Salvia R, Crippa S, Warshaw AL, Bassi C, Falconi M, Thayer SP, et al. Branch-duct intraductal papillary mucinous neoplasms: observations in 145 patients who underwent resection. Gastroenterology. 2007; 133: 72-79. [PMID: 17631133]
- Schnelldorfer T, Sarr MG, Nagorney DM, Zhang L, Smyrk TC, Qin R, Chari ST, Farnell MB. Experience with 208 resections for Intraductal papillary mucinous neoplasm of the pancreas. Arch Surg. 2008; 143: 639- 646. [PMID: 18645105]
- Mimura T, Masuda A, Matsumoto I, Shiomi I, Yoshida S, Sugimoto M, Sanuki T, et al. Predictors of malignant intraductal papillary mucinous neoplasm of the pancreas. J Clin Gastroenterol. 2010; 44: 224-229. [PMID: 20453661]
- Akita H, Takeda Y, Hoshino H, Wada H, Kobayashi S, Marubashi S, Eguchi H, et al. Mural nodule in branch duct-type intraductal papillary mucinous neoplasms of the pancreas is a marker of malignant transformation and indication for surgery. Am J Surg. 2011; 202: 214–219. [PMID: 21376305]
- Uehara H, Ishikawa O, Katayama K, Kawada N, Ikezawa K, Fukutake N, Takakura R, et al. Size of mural nodule as an indicator of surgery for branch duct intraductal papillary mucinous neoplasm of the pancreas during follow-up. J Gastroenterol. 2011; 46: 657–663. [PMID: 21085997]
- Kim KW, Park SH, Pyo J, Yoon SH, Byun JH, Lee MG, Krajewski KM, Ramaiya NH. Imaging features to distinguish malignant and benign branch-duct type intraductal papillary mucinous neoplasms of the pancreas. A meta-analysis. Ann Surg. 2014; 259: 72–81. [PMID: 23657084]
- Kubo H, Chijiiwa Y, Akahoshi K, Hamada S, Harada N, Sumii T, Takashima M, Nawata H. Intraductal papillary-mucinous tumors of the pancreas: differential diagnosis between benign and malignant tumors by endoscopic ultrasonography. Am J Gastroenterol. 2001; 96: 1429-1434. [PMID: 11374678]
- Choi BS, Kim TK, Kim AY, Kim KW, Park SW, Kim PN, Ha HK, Lee MG, Kim SC. Differential diagnosis of benign and malignant intraductal papillary mucinous tumors of the pancreas: MR cholangiopancreatography and MR angiography. Korean J Radiol. 2003; 4: 157- 162. [PMID: 14530644]
- Kawai M, Uchiyama K, Tani M, Onishi H, Kinoshita H, Ueno M, Hama T, Yamaue H. Clinicopathological features of malignant intraductal papillary mucinous tumors of the pancreas: the differential diagnosis from benign entities. Arch Surg. 2004; 139: 188-192. [PMID: 14769579]
- Ogawa H, Itoh S, Ikeda M, Suzuki K, Naganawa S. Intraductal papillary mucinous neoplasm of the pancreas: assessment of the likelihood of invasiveness with multisection CT. Radiology. 2008; 248: 876–886. [PMID: 18632526]
- Shimizu Y, Yamaue H, Maguchi H, Yamao K, Hirono S, Osanai M, Hijioka S, et al. Predictors of malignancy in intraductal papillary mucinous neoplasm of the pancreas. Analysis of 310 pancreatic resection patients at multiple high-volume centers. Pancreas. 2013; 42: 883-888. [PMID: 23508017]
- Kobayashi N, Sugimori K, Shimamura T, Hosono K, Watanabe S, Kato S, Ueda M, et al. Endoscopic ultrasonographic findings predict the risk of carcinoma in branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreatology. 2012;12: 141-145. [PMID: 22487524]
- Hirono S, Tani M, Kawai M, Okada K, Miyazawa M, Shimizu A, Kitahata Y, Yamaue H. The carcinoembryonic antigen level in pancreatic juice and mural nodule size are predictors of malignancy for branch duct type intraductal papillary mucinous neoplasms of the pancreas. Ann Surg. 2012; 255: 517–522. [PMID: 22301608]
- Zhang HM, Yao F, Liu GF, Wang XB, Xiu DH, Gen I. The differences in imaging features of malignant and benign branch duct type of intraductal papillary mucinous tumor. Eur J Radiol. 2011; 80: 744-748. [PMID: 21454028]
- Uehara H, Nakaizumi A, Iishi H, Tatsuta M, Kitamra T, Okuda S, Ohigashi H, et al. Cytologic examination of pancreatic juice differential diagnosis of benign and malignant mucin-producing tumors of the pancreas. Cancer 1994; 74: 826-833. [PMID: 8039110]
- Uehara H, Nakaizumi A, Tatsuta M, Iishi H, Kitamura T, Ohigashi H, Ishikawa O, Takenaka A. Diagnosis of carcinoma in situ of the pancreas by peroralpancreatoscopy and pancreatoscopic cytology. Cancer. 1997; 79: 454-461. [PMID: 9028354]
- Murakami Y, Uemura K, Hayashidani Y, Sudo T, Sueda T. Predictive factors of malignant or invasive intraductal papillary-mucinous neoplasms of the pancreas. J Gastrointest Surg. 2007; 11: 338–344. [PMID: 17458608]
- Yamaguchi T, Shira Y, Ishiharai T, Sudo K, Nakagawa A, Ito H, Miyazaki M, Nomura F, Saisho H. Pancreatic juice cytology in the diagnosis of intraductal papillary mucinous neoplasm of the pancreas. Cancer. 2005; 104: 2830-2836. [PMID: 16287152]
- Yamaguchi K, Nakamura M, Shirahane K, Kawamoto M, Konomi H, Ohta M, Tanaka M. Pancreatic juice cytology in IPMN of the pancreas. Pancreatology. 2005; 5: 416-421. [PMID: 15985766]
- Ohtsuka T, Kono H, Nagayoshi Y, Mori Y, Tsutsumi K, Sadakari Y, Takahata S, et al. An increase in the number of predictive factors augments the likelihood of malignancy in branch duct intraductal papillary mucinous neoplasm of the pancreas. Surgery. 2012; 151:76-83. [PMID: 21875733]



