Keywords
Pancreatic Ducts; Pancreatitis
Abbreviations
ERCP endoscopic retrograde
cholangiopancreatography; NSAIDs non-steroidal anti-inflammatory
drugs; PD pancreatic duct
INTRODUCTION
Post endoscopic retrograde cholangiopancreatography
(ERCP) pancreatitis (PEP) is the most frequent
complication following ERCP, occurring in approximately
3.5% of unselected cases, with a 1-10% rate in average risk
patients, but 25-30% in high-risk patients, such as those
with suspected sphincter of Oddi dysfunction (SOD) [1].
PEP is classified as severe in 11% of cases, which has a
recognised morbidity and mortality [2].
Rectal non-steroidal anti-inflammatory drugs (NSAIDs)
have been shown to reduce the incidence, as well as the
severity, of PEP, even in high-risk patients [3, 4, 5]. The
most recent European Guidelines advise that rectal NSAIDs are used before or immediately after ERCP in all patients
without contraindications [6].
Prior to the rectal NSAIDs era, pancreatic duct (PD)
stenting was a well-established method of reducing PEP,
especially in high-risk patients. Randomised controlled
trials showed that prophylactic PD stenting reduced the
incidence of PEP by up to 70% [7, 8]. This trend has also
been confirmed in a recent meta-analysis that showed
that patients who had prophylactic PD stenting had a
significantly lower incidence of PEP than groups without
PD stents (OR=0.35, 95% CI 0.25-0.49) [9]. However,
if PD stenting is attempted, but fails, the rate of PEP
increases significantly to 35-66% in high-risk patients
[9, 10]. Therefore, the 2016 ESGE guideline on papillary
cannulation and sphincterotomy state that prophylactic
PD stenting should only be performed by experienced
endoscopists [11]. Interestingly, patients with failed PD
stent insertion who received rectal NSAIDs may have
lower rates of PEP, reported as only 5.3% in one study [5].
Larger studies including patients who had failed pancreatic
ducts stenting but had received rectal NSAIDs are required
to confirm these findings. Therefore, we retrospectively
assessed a large dataset including the failed PD stent group
in a period where all patients without a contraindication
received rectal NSAIDs.
METHODS
This was a retrospective cohort study conducted at
University College London Hospital (UCLH), in London, a
tertiary referral centre for ERCP.
Inclusion Criteria
Patients were >18 years old, who underwent an ERCP
between January 1st 2013 and June 30th 2015.
Data Recorded
Cases were identified from our prospectively collected
ERCP database. In addition, endoscopy (GI reporting tool,
Unisoft medical systems, UK), imaging (PACS: picture
archiving and communication system, GE Healthcare, USA),
and electronic patient record databases were searched
for procedure and patient outcome information. Patients
referred from other hospitals were contacted by telephone
maximally twice and if we were unable to contact them,
they were assumed as lost to follow-up.
Endoscopic Retrograde Cholangiopancreatography
(ERCP) Procedure
Informed written consent for each procedure was
obtained, and included consent for rectal NSAIDs
(Indomethacin or Diclofenac 100 mg rectally directly at end
of the procedure) in all patients without contraindications.
All ERCPs were performed by one of four experienced
endoscopists using a standard duodenoscope (JFV or TJFV;
Olympus KeyMed, Southend-on-Sea, UK) or Pentax scope
ED34-i10T video duodenal scope. All patients were observed
for 4 hours in the recovery area prior to discharge. Those
with significant co-morbidity or who became symptomatic
following the procedure were admitted to hospital for further
observation and management as needed. Patients were
discharged with written instruction concerning contacting
the unit in the event of new symptoms suggestive of postprocedure
complications.
Prophylactic PD stenting was attempted in those
patients with predicted high risk of PEP (e.g. suspected
sphincter of Oddi dysfunction, multiple pancreatic duct cannulation). Therapeutic PD stents were inserted in
patients undergoing pancreatic endotherapy. Failed PD
stenting was defined as attempt to stent but failure to
actually deploy, which is a recorded field in our prospective
ERCP data sheet. Single pigtail unflanged 5Fr 5-7 cm stents
were used for prophylaxis (Cook Medical Inc, Bloomington,
IN, USA). The type of therapeutic pancreatic stent used
was chosen at the discretion of the endoscopist, but were
5-7Fr, 3-9 cm (Cook Medical Inc).
Pancreatitis Definition
Post ERCP pancreatitis (PEP) was defined as new or
worsened abdominal pain, in association with a serum
concentration of pancreatic enzymes (amylase or lipase)
that was at least three times the upper limit of normal at
more than 24 hours after the procedure, requiring hospital
admission or a prolongation of planned admission [12].
Statistical Analyses
Statistical Package for Social Sciences for Windows,
version 18.0 (SPSS Inc., Chicago, IL, USA) was used to
perform all statistical analyses. Relative risks were
calculated according to Altman, 1991.
RESULTS
Patient Demographics and Indications for ERCP
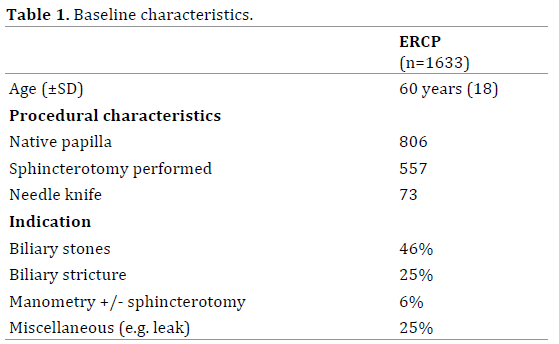
A total of 1633 ERCP procedures were performed
during the 30 month study period (Figure 1). The mean
(SD) age was 60 years (±18). Indications for ERCP included
the management of biliary stones (46%), assessment and
treatment of a biliary stricture (25%), and SOD (manometry
+/- sphincterotomy) (6%). The remaining 25% consisted
of a heterogeneous group (e.g. stent removal/change,
biliary leak) (Table 1).
Figure 1. Flow diaphragm of ERCPs and number of patients needing stents with subsequent post-ERCP pancreatitis (PEP) rates.
Indications for PD Stent Insertion and Rate of Post
ERCP Pancreatitis
Prophylactic PD stenting was attempted in 213
patients (13% of total ERCPs), and was successful in 94%
of cases. Indications for stenting included SOD (24%), prior to needle knife/pre-cut sphincterotomy (10%),
and pancreatic sphincterotomy (2.5%). Prophylactic PD
stenting failed in 12 patients, with PEP in one patient
(8.3%). Successful prophylactic PD was associated with
PEP in 9%, with no difference in relative risk of developing
PEP in the failed prophylactic versus the successful PD
stent placement (p=0.8).
Patients with successful prophylactic PD stents had a
9% risk of PEP vs. 1.4% in those without PD stent placement
(Table 2). There was no difference in relative risk to develop
PEP in the prophylactic PD stent group compared to the
therapeutic PD stent group, 5.5 (p=0.09). Patients receiving
prophylactic PD stents were at higher risk to develop PEP
compared to the unstented group, 6.6 (p<0.001).

Rectal NSAIDs
Rectal NSAIDS were administered to 87% of patients.
Of the 214 patients who did not receive rectal NSAIDs, 106
patients had contra-indications to NSAIDs (group A) and
no specific reason was found/given for 108 patients (group
B). Group A had 1 episode of PEP without prophylactic
PD stent and had PD stents inserted in 18 patients (12
prophylactic, 2 assist cannulation, 4 therapeutic). Group B
had no PEP episodes and had 12 patients with PD stents (8
prophylactic, 3 assist cannulation, 1 failed prophylactic).
In a sub-group of patients, 8 patients (3.8%), who
had contra-indications to NSAIDs and had successful
prophylactic PD stent no PEP was reported.
Other Adverse Events
Nine patients (0.6%) developed perforation, of whom 3
had PD stents and 6 had sphincterotomy (n=4 needle knife).
A total of 17 (1%) developed minor post-sphincterotomy
bleeding (none requiring transfusion).
DISCUSSION
In patients at high risk of PEP, historical studies
estimate the risk of PEP to be as high as 30-40% [12, 13, 14]. In a seminal study of ERCP in patients with
suspected SOD, Tanarsky et al. showed that PD stent
placement reduced the risk of PEP from 26% to 7% [10].
An important observation of studies of PD stenting is that
whilst high rates of successful stent placement have been
reported from specialist centres (>96%), attempted, but
failed, stenting is associated with markedly increased rates
of PEP (>60%), with an increased risk of a severe course
[15, 16]. In the present study of a large single-centre
cohort of patients, the rate of PEP in patients receiving PD
stenting (with a predicted high risk of PEP) was 9%, a level
expected on the basis of previous studies. The interesting
observation was that the rate of PEP in those in whom PD
stenting failed was only 8%. In addition, the only patient
in this group who developed PEP following failed PD stent
insertion had a contra-indication to NSAIDs. Our study
supports the findings of Choksi et al. who reported that
in those patients in whom PD stenting was unsuccessful,
35% developed PEP, but when rectal NSAIDs were given
the rate of PEP was only 5% [5]. It therefore seems likely that routine rectal NSAIDs use attenuates the risk of
PEP, perhaps to the extent that this negates the need for
prophylactic PD stenting (as suggested by an apparent lack
of increase in PEP in the setting of failed PD stenting).
The question remains as to whether the routine use of
rectal NSAIDs alone renders PD stenting an unnecessary
additional intervention in reducing the incidence of PEP.
Recently, the combination of rectal NSAIDs and stents
has not been shown to be superior to either approach
alone [1]. Although in our study 9% of patients receiving
prophylactic PD stenting and NSAIDs developed PEP,
compared to 1.4% who received only NSAIDS, this is likely
to be explained by the endoscopists’ pre- or peri-procedure
assessment of the patients as being at high risk of PEP,
leading to a decision to attempt PD stenting. However, it
is not possible to categorically conclude from our study
whether the increased relative risk of PEP in those patients
undergoing attempted PD stenting (RR 6.6 (p≤0.001)),
compared to the unstented group, was due to inherent
risk of PEP in those selected for stenting, or as a result
of attempted stenting per se. In a recent retrospective
study from China (623 patients in the period 2008-
2014), the authors concluded that prophylactic PD
stents may be a superior method in preventing PEP
when compared to NSAIDs [17]. Interestingly though,
rectal NSAIDs were only given in high-risk cases at
the discretion of the surgeon/ endoscopist and when
given, they were not immediately given after ERCP. The
latter is relevant as a recent analysis of randomised
controlled trials showed that PEP was reduced
especially in the group where rectal NSAIDs were given
before ERCP [18]. Surprisingly, a recently published
randomized controlled trial did not show reduced PEP
risks in patients receiving rectal indomethacin [19]. An
explanation could be that most of these patients (70%)
were of average risk for PEP. Another explanation for
the results could be the use of indomethacin as a metaanalysis
of 11 randomised controlled trials showed no
significant effect of Indomethacin on preventing PEP
compared to other NSAIDs [18]. An awaited prospective
randomised study of rectal NSAIDs versus rectal NSAIDs
and PD stenting in patients at high risk of PEP may help
to resolve this important clinical question [20] .
Limitations of this study include the fact that the
data was collected retrospectively; 7% of patients did not receive NSAIDS, despite the absence of recorded
contraindication; and 7.6% patients were lost to followup
in the unstented group compared to 3% in the stented
group. Also, as PD stent insertion was left to the discretion
of the endoscopist, eg. to assist biliary cannulation, this was
likely a source of bias as to which patients were stented
by the 4 experienced endoscopists doing the procedures.
Lastly, we showed that unfortunately 108/214 patients
who didn’t receive rectal NSAIDs didn’t seem to have had
an apparent reason for this, which we have used in an audit
to optimise rectal NSAIDs implementation.
CONCLUSION
In this large single centre cohort study of patients
undergoing ERCP, in whom prophylactic NSAIDs were given
as standard, no difference in rates of PEP were seen in those
high risk patients who underwent successful PD stenting,
compared to those in whom PD stenting was attempted,
but failed. Despite the retrospective character of this study
with limitations as outlined above, our findings do support
emerging data that the benefit of NSAIDS may negate or
reduce the necessity of PD stenting to reduce the risk of PEP.
Acknowledgments
Funding: This work was supported by NIH Grant PO1
CA084203.
Conflict of Interest
The authors declare that they have no conflict of interest
References
- Akbar A, Abu Dayyeh BK, Baron TH, Wang Z, Altayar O, Murad MH.
Rectal nonsteroidal anti-inflammatory drugs are superior to pancreatic
duct stents in preventing pancreatitis after endoscopic retrograde
cholangiopancreatography: a network meta-analysis. Clin Gastroenterol
Hepatol 2013; 11:778-83. [PMID: 23376320]
- Hanna MS, Portal AJ, Dhanda AD, Przemioslo R. UK wide survey on
the prevention of post-ERCP pancreatitis. Frontline Gastroenterol 2014;
5:103-110. [PMID: 24724007]
- Sun HL, Han B, Zhai HP, Cheng XH, Ma K. Rectal NSAIDs for the
prevention of post-ERCP pancreatitis: a meta-analysis of randomized
controlled trials. Surgeon 2014; 12:141-7. [PMID: 24332479]
- Elmunzer BJ, Scheiman JM, Lehman GA, Chak A, Mosler P, Higgins PD,
et al. A Randomized Trial of Rectal Indomethacin to Prevent Post-ERCP
Pancreatitis. N Engl J Med 2012; 366:1414-1422. [PMID: 22494121]
- Choksi NS, Fogel EL, Cote GA, Romagnuolo J, Elta GH, Scheiman JM,
et al. The risk of post-ERCP pancreatitis and the protective effect of rectal
indomethacin in cases of attempted but unsuccessful prophylactic pancreatic
stent placement. Gastrointest Endosc 2015; 81:150-5. [PMID: 25527053]
- Dumonceau JM, Andriulli A, Elmunzer BJ, Mariani A, Meister T,
Deviere J, et al. Prophylaxis of post-ERCP pancreatitis: European Society
of Gastrointestinal Endoscopy (ESGE) Guideline - updated June 2014.
Endoscopy 2014; 46:799-815. [PMID: 25148137]
- Choudhary A, Bechtold ML, Arif M, Szary NM, Puli SR, Othman MO,
et al. Pancreatic stents for prophylaxis against post-ERCP pancreatitis: a
meta-analysis and systematic review. Gastrointest Endosc 2011; 73:275-
82. [PMID: 21295641]
- Mazaki T, Masuda H, Takayama T. Prophylactic pancreatic stent
placement and post-ERCP pancreatitis: a systematic review and metaanalysis.
Endoscopy 2010; 42:842-53. [PMID: 23612857]
- Fan JH, Qian JB, Wang YM, Shi RH, Zhao CJ. Updated meta-analysis
of pancreatic stent placement in preventing post-endoscopic retrograde
cholangiopancreatography pancreatitis. World J Gastroenterol 2015;
21:7577-83. [PMID: 26140006]
- Tarnasky PR, Palesch YY, Cunningham JT, Mauldin PD, Cotton
PB, Hawes RH. Pancreatic stenting prevents pancreatitis after biliary
sphincterotomy in patients with sphincter of Oddi dysfunction.
Gastroenterology 1998; 115:1518-24. [PMID: 9834280]
- Testoni PA, Mariani A, Aabakken L, Arvanitakis M, Bories E,
Costamagna G, et al. Papillary cannulation and sphincterotomy techniques
at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical
Guideline. Endoscopy 2016; 48:657-83. [PMID: 27299638]
- Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al.
Endoscopic sphincterotomy complications and their management: an attempt
at consensus. Gastrointest Endosc 1991; 37:383-93. [PMID: 2070995]
- Gottlieb K, Sherman S. ERCP and biliary endoscopic sphincterotomyinduced
pancreatitis. Gastrointest Endosc Clin N Am 1998; 8:87-114.
[PMID: 9405753]
- Freeman ML. Adverse outcomes of ERCP. Gastrointest Endosc 2002;
56:S273-S282. [PMID: 12447281]
- Lee TH, Moon JH, Choi HJ, Han SH, Cheon YK, Cho YD, et al.
Prophylactic temporary 3F pancreatic duct stent to prevent post-ERCP
pancreatitis in patients with a difficult biliary cannulation: a multicenter,
prospective, randomized study. Gastrointest Endosc 2012; 76:578-85.
[PMID: 22771100]
- Freeman ML, Overby C, Qi D. Pancreatic stent insertion: consequences
of failure and results of a modified technique to maximize success.
Gastrointest Endosc 2004; 59:8-14. [PMID: 14722540]
- Li GD, Jia XY, Dong HY, Pang QP, Zhai HL, Zhang XJ, et al. Pancreatic Stent
or Rectal Indomethacin-Which Better Prevents Post-ERCP Pancreatitis?:
A Propensity Score Matching Analysis. Medicine (Baltimore) 2016;
95:e2994. [PMID: 26962808]
- Rustagi T, Njei B. Factors Affecting the Efficacy of Nonsteroidal
Anti-inflammatory Drugs in Preventing Post-Endoscopic Retrograde
Cholangiopancreatography Pancreatitis: A Systematic Review and Metaanalysis.
Pancreas 2015; 44:859-67. [PMID: 26168316]
- Levenick JM, Gordon SR, Fadden LL, Levy LC, Rockacy MJ, Hyder
SM, et al. Rectal Indomethacin Does Not Prevent Post-ERCP Pancreatitis
in Consecutive Patients. Gastroenterology 2016; 150:911-7; quiz e19.
[PMID: 26775631]
- Elmunzer BJ, Serrano J, Chak A, Edmundowicz SA, Papachristou GI,
Scheiman JM, et al. Rectal indomethacin alone versus indomethacin and
prophylactic pancreatic stent placement for preventing pancreatitis after
ERCP: study protocol for a randomized controlled trial. Trials 2016;
17:120. [PMID: 26941086]


