Keywords
Anxiety disorders; Psychologists; Mental retardation; Disruptive disorders; Expressed emotion
Introduction
Anxiety Disorders (AD) constitute the most prevalent mental disease in children, affecting 9-21% of children and adolescents at some point in their lives [1]. Children can manifest transient symptoms of anxiety as part of typical development [2,3], but childhood AD often persist in adolescence and adulthood [1]. The most common AD in children include Separation Anxiety Disorder (SAD) which typical to childhood, even if it may persist until adolescence and adulthood, Social Anxiety (SA) and Specific Phobia (SP). On the other hand, Generalized Anxiety Disorder (GAD) and Panic Disorder (PD) are less frequent in children (Table 1) [4].
| Anxiety type |
Definition and main symptoms |
Age of asset |
12-month prevalence1 |
| Separation Anxiety (SAD) |
Excessive anxiety when children are separated from their parents or caregivers.
Symptoms: tendency to worry about something bad occurring to loved ones while they are apart, refusal of situations that take family far, such as going to school |
Childhood |
4% |
| Generalized Anxiety Disorder (GAD) |
Persistent, excessive, and unrealistic worries about everyday life.
Symptoms: tendency to strive for perfection and seek constant reassurance from others |
Childhood or adolescence |
0.9% |
| Social Anxiety (SA) |
Extreme fear of being scrutinized and judged by others in social situations.
Symptoms: social ability impairment, unsatisfactory relationships with peers |
Childhood |
7% |
| Specific Phobia (SP) |
Intense and irrational fear of a specific object or situations, like animals, water, dark or medical procedures.
Symptoms: avoidance of phobic things and situations, anxious feelings and physiological symptomatology like crying, headaches or stomach-aches. |
Childhood |
5% |
| Panic Disorder (PD) |
At least 2 sudden and unexpected anxiety attacks and a concern of having another one that lasts more than 4 weeks.
Symptoms: physical reactions, such as nausea, heavy breathing and shaking |
Childhood |
0.4% |
Note: APA DSM-5 (2013)1
Table 1: Main paediatric anxiety disorders.
Clinical anxiety causes significant problems in daily functioning and AD are often associated with other comorbid conditions as depression, suicidality or substance use disorders [5]. Consequently, it is imperative to identify the characteristic of children with pathological anxiety as well as the cognitive underpinnings of paediatric anxiety disorders to develop efficient therapeutic intervention and prevent a chronic evolution of anxiety. Etiological models of pathological anxiety postulate a central role of emotion dysregulation, notably abnormal reactions to stress and motivational stimuli [6]. Given the particular salience of Emotional Facial Expressions (EFE) in everyday life, they are first- choice stimuli to explore cognitive processing of emotional information [7].
Accordingly, numerous studies have demonstrated a biased processing of EFE in anxiety disorders in children [8] and adults [9]. Amongst the most typical paradigms used to examine these biases, spatial cueing paradigms are designed to evaluate selective attention, and Stroop paradigms to evaluate the abilities to control emotional interferences [8,10]. Benoit et al. [11] study suggested that anxious children displayed longer response latencies to name the colour of filters placed over grayscale emotional faces, regardless of the type of anxiety, in comparison with control children. Age may play a moderator effect in the occurrence of attentional biases, as younger (7-10 years old) moderately-anxious children were described as presenting an enhanced bias for emotional faces as compared to older children (11-14 years old) in emotional Stroop and visual probe tasks [12]. Accordingly, these authors hypothesised that attentional bias to threat decreases with age, possibly with the development of attentional control [13]. The importance of inhibition abilities was also outlined by Hadwin et al. [14] who found a correlation between high social concerns and low inhibition capabilities toward angry EFE in comparison to neutral ones, in children from 6 to 12 years. Concerning the extend of the biases, some studies observed a slower response for angry faces solely [12] while others reported longer RT also for happy faces [11,15] and even for neutral faces [11]. Such inconsistencies may be explained by the fact that some paradigms presented adult faces [12], mixed child and adult faces [11] or schematic faces [14,15]. When comparing child and adult faces, Benoit et al. [11] reported slower colour naming, meaning enhanced interferences, for adult faces than for child faces, irrespective of facial expressions and anxiety levels. Accordingly, adult expressions may be more salient and attract more attentional resources, but this hypothesis has not been tested anymore.
If anxiety can alter the perception of EFE, it can also lead to emotion identification biases. The ability to identify emotions develops from birth, as babies can discriminate emotional facial expressions at 4 months [16], categorize those 3 months later [17] and perceive pleasant or unpleasant meaning around the age of 1 year. The recognition of fundamental EFE emerges between 2 and 3 years [18] and is excellent between 5 and 6 years for joy, sadness and anger [19,20], while recognition of fear, disgust and surprise appears later and improves between 5 and 10 years [21]. Nevertheless, behavioural and neuroimaging studies indicate that EFE recognition capabilities and associated brain regions continue to develop during childhood and late adolescence. The ability to identify EFE has mostly been explored by mean of explicit tasks in which participants have to recognize the displayed EFE. Two studies found no emotionlabeling deficits [22,23] in anxious children, regardless the type of anxiety. However, other results suggest decreased abilities to identify anger in anxious adolescents [24]. These discrepancies could result from differences in methods and anxiety diagnosis, as SA seems particularly associated with slower identification RT for neutral faces [25] and lower accuracy for faces expressing happiness, sadness and disgust [26].
However, very few researches compared the abilities to identify adult and child EFE. Indeed, children interact more with peers than adults during the day school and their relationships with peers and adults cater to different dynamics. Their interaction with adults are usually laced with dependence and authority while interaction with other children is rather driven by social inclusion concern. Gifford-Smith and Brownell [27] pointed out that peer acceptance is most critical in elementary school and decreases with age. Accordingly, children may process adult and child-posed faces differently, as suggested by Benoit et al. [11]. Three studies did not report difference between child and adult faces when anxious and non-anxious children completed Forced- Choice (FC) tasks [22,23,25]. However, Easter et al. [28] revealed higher error rates for adult faces than child faces for both anxious (GAD, SAD, SP) and non-anxious youths performing in EFE identification task (FC: anger, fear, joy, sadness). The two groups did not differ on child faces accuracy, whereas the experimental group showed poorer performance on adult faces accuracy than the control group. This result suggests a differential processing of adults and peers’ emotions in anxiety. Age may also impact on emotion labelling abilities, as suggested by McClure et al. [23]. Their study recruited participants with bipolar and anxious disorders from 10 to 16 years old. Younger bipolar adolescents made more errors in identifying child faces expressing high or low levels of anger. This difference was not found in older participants. This hypothesis could interestingly be examined by recruiting younger anxious children (under 10).
Accordingly, our study aimed to investigate whether anxiety disturbed the processing of angry and happy expression in children and whether attention biases or identification biases were more pronounced for adult faces or child faces. To this aim, we proposed a forced-choice paradigm in which children had to judge the gender, the age or the emotional expression of adult and child EFE. This paradigm has been used to study emotion processing in other pathologies than anxiety disorders, such as depression [29] or schizophrenia. As children reach the same emotional recognition abilities than adults at age 6 [30] and anxiety is often diagnosed around 8 years old [31], we decided to focus on children between 6 and 9. We first expected differences in child and adult EFE processing (RT and CA). As children aged less than 9 are less efficient in inhibiting emotional information [32], we expected, in all participants, better and faster identification in the explicit condition (identifying emotion) than the implicit ones (identifying age and gender) and we hypothesised that all children should identify anger faster than joy [33]. We expected anxious children, in comparison with the control group, to be more accurate in identifying child EFE than adult ones [28], and to identify faster angry faces, but to answer slower for angry faces in the implicit condition (identifying age and gender) because of the interference elicited by threat.
Methods
Participants
Participants included 40 French-speaking children (22 males, 18 females) aged from 6 to 9 years old (M=7.54, SD=0.83). Anxious children were recruited through e-mail advertisements, flyers distributed through schools, mental health centres and independent psychologists. Participants were included in the clinical group if they were currently in mental health treatment for anxiety (11 children) and/or if they met SCARED (scores ≥ 25) and STAI-C criteria (scores ≥ 34) for an anxiety disorder (9 children). In the anxious group, 11 children received a diagnosis from a psychologist: 3 SA, 3 SAD, 2 GAD, 1 Performance Anxiety (PA) and 2 comorbid SA-SAD (Table 2). They were from 6 different provinces of Belgium (Walloon Brabant, Liege, Brussels, Luxembourg, Hainaut and Namur). Exclusion criteria included mental retardation, physical handicap and ADHD, since the study involved a computer-based attention task. Control children presented no anxious complain and performed low anxiety scores at SCARED and STAI inventories.
| Characteristics |
Anxious (n=20)
Mean (SD) |
Healthy (n=20)
Mean (SD) |
Statistics |
p |
| Gender |
60% male |
50% male |
X2=0.4 |
n.s. |
| Age |
92.4 months (10.8) |
92.4 months (8.4) |
t(38)=-1.1 |
n.s. |
| Laterality |
95% right-hander |
95% right-hander |
X2=0.8 |
n.s. |
| STAI (trait) |
-1.4 (0.7) |
-0.4 (0.47) |
t(38)=5.2 |
<0.001 |
| SCARED |
39.6 (17.6) |
24.1 (10.0) |
t(38)=3.4 |
0.001 |
| Anxiety comorbidity |
Single diagnosis
• SA
• GAD
• SADPerformance |
SCARED 6
3
5
2 |
Psy. 3
2
3
1 |
- |
4 (20%)
5 (25%)
3 (15%)
3 (15%) |
|
Two diagnoses
• SA + SAD |
4 |
2 |
- |
5 (25%) |
|
Note: SCARED: Screen for Anxiety and Related Disorders; STAI: State-Trait Anxiety Inventory for Children; Psy: Psychologist Diagnosis; SA: Social Anxiety; GAD: Generalized Anxiety Disorder; SAD: Separation Anxiety Disorder
Table 2: Characteristics of anxious and healthy control participants.
Procedure
The study protocol was approved by the Ethical Panel of the Catholic University of Louvain, where the study took place. Upon arrival at the research lab, parents and children were presented with the study protocol and asked to sign consent and assent forms. The child first completed the self-reported inventory (see below) and then achieved the experimental session. Parents were also administered a semi-structured interview about child's fears and were asked about their child's past and current psychological treatment for anxiety.
Measures
STAI-C: To assess children level of anxiety, they were administered the French version [34] of the Spielberger State-trait Anxiety Inventory for Children [35]. This scale contains a 20-items state subscale and a 20-items trait. Items are scored on 3-point Likert scales (1=Almost never, 2=Sometimes, 3=Often) evaluating the frequency of anxiety symptoms experiences.
SCARED-R-51: The Screen for Child Anxiety Related Emotional Disorders (SCARED-R) [3,36] is a 51-item self-report instrument constructed for evaluating anxiety disorders, discriminating other associated disorders such as depression and disruptive disorders and distinguishing specific types of anxiety such as GAD (e.g. “I worry about things working out for me”), SA (e.g. “I don't like to be with people I don't know”) or SAD (e.g. “I don't like being away from my family”). Items are scored on 3-point Likert scales (1=Never/Rarely; 2=Sometimes; 3=Often). In our study, the French version [37] was used. This version is validated for children between the ages of 8 and 15.
EFE judgment task: The stimulus set was composed of pictures of Caucasian human faces, taken from Radboud faces database [38]. Facial stimuli were oval-trimmed by excluding non-facial contours and hair and resized at the same size, so that eyes appeared at the same level on the screen. They differed in gender (man or female), cohort (adult or child) and expressed emotion (anger or happiness). 48 different stimuli were then generated (3 men, 3 boys, 3 women, 3 girls, each expressing anger or happiness). Children were confronted to three conditions, as they were asked to make dichotomous judgment on EFE (‘happy’ or ‘angry’) or on non-emotional features (age or gender). Participants were seated 40 cm in front of an LCD monitor with a display resolution of 1,280 × 1,024 pixels. The task was programed with an ePrime 2.0 device and was presented as a game where the instruction appears at the beginning of each block (‘tell me if the person on the screen is a boy or a girl/child or adult/happy or angry’). Participants were confronted to 12 blocks of 50 stimuli, 4 in each condition (age, gender or emotion), the conditions changed between each block and their order was counterbalanced between the participants.
A trial started with the presentation of a fixation cross on a white background for 500 ms. Stimuli were then presented one by one for 500 ms and the inter-trial interval lasted between 1000 and 1500 ms. The entire experiment consisted of 600 trials, with a pseudo-randomized presentation of the different types of cues within each block. Children were tested individually in a single-session lasting approximately 45 min.
Statistical Analysis
Statistical analyses were computed using Statistical Package for Social Sciences, version 23 (SPSS 23.0). We examined children correct answers rates (CA) and their Reaction Time (RT) on correct answers. For this purpose, 3 × 2 × 2 × 2 repeated-measures Analyses of Variance (ANOVA) were conducted with condition (judgment on age, gender or emotion), emotion (expressing happiness or anger) and cohort (adult vs. child) as within-subject factors, and Group as between subject factor (anxious and non-anxious participants). CA and RT results appear in Table 3. Alpha level of significance was set at 0.05. Greenhouse-Geiser epsilon correction was used in order to compensate for violation of sphericity and Bonferroni post-hoc tests to explore simple effects when appropriate. Eta-squared were calculated to certify statistical power. Finally, in-depth paired t-tests analyses were likewise conducted to explore interaction effects.
| |
Adult Cohort Mean (SD) (N=40) |
Child Cohort Mean (SD) (N=40) |
| Anger Emotion |
Happiness Emotion |
Anger Emotion |
Happiness Emotion |
| Age |
RT CA |
622 (202)
48.9 (20.0) |
628 (188)
50.4 (21.5) |
645 (173)
61.0 (17.6) |
641 (204)
59.0 (17.7) |
| Emotion |
RT CA |
629 (149)
70.3 (15.2) |
619 (153)
68.5 (15.7) |
639 (158)
62.0 (18.2) |
639 (166)
62.2 (19.1) |
| Gender |
RT CA |
621 (197)
53.0 (13.5) |
627 (177)
55.7 (13.5) |
648 (205)
46.7 (9.3) |
629 (204)
46.1 (8.2) |
Note: SD: Standard Deviation; RT: Reaction Time; CA: Correct Answer
Table 3: Descriptive statistiques.
Results
Firstly, our results revealed significant differences in CA rates between conditions, F(2,38)=57.603, p<0.001, partial η2=0.603. More precisely, participants registered better scores in the emotion judgment condition than in the age condition (p<0.001). Gender judgment was the most difficult condition with a rate of 50% mistakes (Emotion-Gender: p<0.001; age-gender: p<0.001).
Second, our results showed a main effect of the emotional expression displayed by stimuli through conditions, F(1,38)=4.374, p=0.043, partial η2=0.103, with more accurate judgments on angry faces than happy ones. Interestingly, an interaction between condition and emotion (F(2,38)=7.669, p=0.003, partial η2=0.168) means that this effect was only present in the emotion condition (t(39)=2.906, p=0.006), but not in gender (t(39)=-0.999, n.s.), nor in age judgment (t(39)=0.265, n.s.).
Third, our results showed a main effect of cohort on RT, F(1,38)=8.024, p=0.007, partial η2=0.174, as participants answered faster to adult EFE stimuli as compared to child EFE trials. This cohort factor interacted with condition, F(2,38)=13.558, p<0.001, partial η2=0.263 and paired t-tests revealed that adult EFE speeded up the judgment in gender condition, t(39)=4.451, p<0.001, whereas the contrary appeared in the age condition, t(39)=2.600, p=0.013. No differences were observed in the emotion condition, t(39)=0.791, n.s.
Interestingly, the influence of cohort tended to interact with children’ level of anxiety on CA, F(1,38)=3.596, p=0.066, partial η2=0.086, suggesting anxious participants judged more accurately child faces (t(19)=1.858, p=0.079) while non-anxious youths did not show this trend (t(19)=0.972, n.s.).
This effect was further modulated by emotion, as a third-level interaction between cohort, emotion, and group were marginally observed for CA’s rates (F(1,38)=2.936, p=0.095, partial η2=0.072). This interaction was decomposed in each group and results showed the interaction effect only in the experimental group, F(1,38)=8.424, p=0.009, η2=0.307, but not in the control group, F(1,38)=0.122, p=0.730, η2=0.006). Anxious children answered more properly at child faces expressing anger than at adult ones expressing anger (t(19) =2.786, p=0.012), but no cohort effect emerged for happy faces (t(19)=0.743, n.s.).
This triple interaction was also found in RT, F(1,38)=4.656, p=0.037, η2=0.109. Non-anxious children the interaction showed the interaction between cohort and emotion (F(2,38)=3.879, p=0.064, η2=0.170), meaning that no difference appeared for happy faces (t(19)=-0.218, n.s), but they answered faster to anger on adult faces as compared to child ones (t(19)=2.632, p=0.016). In the anxious group, F(2,38)=4.778, p=0.042, η2=0.201, the interaction between stimuli-cohort and stimuli-emotion was significant for happy faces, t(19)=-2.598, p=0.018, but not for angry faces, t(19)=0.654, n.s.
Discussion
This aim of this study was to investigate whether anxiety can disturb two different levels of information treatment in children while processing adult and child EFE. The results of the present study provided consistent evidence to our hypotheses.
First, we expected a main effect of stimuli type, which was confirmed by shorter RT for adult EFE regarding child ones. Thus, children process faster the facial features of adult faces. According to our second assumption, this effect is modulated by the condition. In the age condition, children had higher accuracy while processing child EFE than adult EFE, suggesting that they identify easier their peers than adults. On the contrary, the opposite pattern was found for gender identification. Children registered the lowest accuracy levels in this condition but they performed slightly above the chance level in identifying the gender of adult faces. This finding is in line with Wild et al. [39] results which highlighted two major phenomena. Firstly, levels of accuracy in gender identification varied from just above chance in 7 year-olds to nearly perfect in adults (developmental factor). As our study involved children from 6 to 9 years old, this developmental factor could explain their worse performance in gender condition. Secondly, they showed that children and adults performed less accurately for child faces than for adult ones. This effect might be attributed to the more pronounced salience of male and female features on adult faces (perceptive factor).
Second, children performed better when they have to identify the emotional expressions of faces as compared to the other dimensions (gender or age), confirming the children’s reliable abilities to recognize emotions [30]. Moreover, all participants demonstrated an influence of emotion on EFE processing. As a matter of fact, children identified more correctly anger expression than joy expression. This finding is in the line with Kindt and Van Den Hout’s [33] theory suggesting that all children under 10 present attentional biases toward threat due to the immaturity of inhibition functions. They may also be due to the salience of anger features at a bottom-up level. Furthermore, the following results support our hypotheses concerning an attentional bias toward child faces in anxious participants and its modulation by anger. In fact, anxious children showed in all conditions a better recognition of child faces together to slower RT to process them. Moreover, our result showed a crucial distinction in processing patterns in anger recognition between anxious and non-anxious participants. Anxious children identified more easily child EFE displaying anger, indexed by higher accuracy and shorter RT (Figure 1), whereas the non-anxious children identified faster adult anger expression.
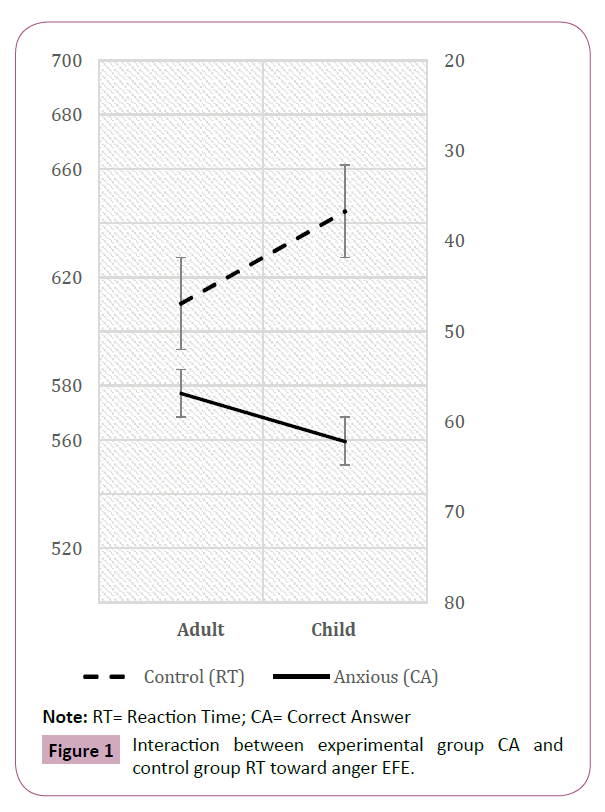
Note: RT= Reaction Time; CA= Correct Answer
Figure 1: Interaction between experimental group CA and control group RT toward anger EFE.
In contradiction with Guyer et al. [22] and Melfsen and Florin’s [25] conclusions, our study pointed out significant differences in the children’ processing of adult and child EFE, when they display anger. This inconsistent result may be attributed to the comorbidity in Guyer’s study participants’ panel, which included in the same experimental group children with anxious and/or major depressive disorder and to the type of anxiety disorder recruited in Melfsen and Florin’s study (social phobia), while we mainly recruited children suffering from GAD, SAD and SA.
While considering emotional faces identification in anxious children, EFE generation choice seems to be of great importance. If anxious and non-anxious children presented a recognition bias toward angry faces, it has two different sources. Non-anxious participants showed more interest in adult angry EFE, whereas anxious children showed more interest in child angry ones. This finding supported a different triggering factor of threat perception, that is to say a differential source of threat for each group. These results are consistent with Easter et al. [28] and Jarros et al. [24] studies, which showed poorest performances in adult EFE recognition in anxious groups (GAD, SAD, SP).
By contrast, Simonian et al. [26] did not found any deficit in adult angry EFE identification in social anxious children. Once again, the difference between these two studies may be attributed to anxiety types recruited since Easter et al. [28] selected anxious children suffering from various anxiety disorders (GAD, SAD, SP) whereas Simonian et al. [26] participants were suffering from social phobia. Accordingly, one may hypothesize that social anxiety is not characterised by deficit in labelling emotions [40], contrary to other types of AD.
These results should be considered from the child’s perspective. In their social environment, adult angry faces mainly indicate the possible occurrence of punitive measures, while child angry faces more probably index peers’ disapproval. On that basis, we can hypothesize that non-anxious children may be more sensitive to punishment threat, whereas anxious children and especially social anxious children may rather fear social rejection. As McClure et al. [23] suggested it in mood disorders, social impairment in paediatric anxiety should be considered in the understanding of identification bias toward peers’ angry faces.
Limitations and Conclusion
To sum up, our study confirmed the interference of emotion on children’s emotional processing, when they have to judge another dimension such as age or gender. It also provided arguments in favour of a differential adult and child EFE processing in anxious and non-anxious children. Even if angry faces were easily recognized by all participants, our design allowed us to clearly disentangle different triggering sources in anxious and non-anxious conditions. Unfortunately, the size of our sample did not allow us to conduct analyses considering participants’ age and type of anxiety with a satisfactory statistical level. Despite these limitations, the study presented here builds on previous research by providing further insights on aetiology of paediatric anxiety by highlighting the significance of anxious children’s peers’ emotional evaluation in social rejection. Thus, EFE displaying child faces seem to be more appropriate in evaluating identification abilities in anxious children and should be preferred in paediatric anxiety studies. To precise these findings, further research would be benefit by recruiting a sufficiently large sample that allows researchers to compare face recognition patterns in distinct types of anxiety.
References
- Ramsawh HJ, Chavira DA, Stein MB (2010) Burden of anxiety disorders in pediatric medical settings: prevalence, phenomenology, and a research agenda. Arch Pediatr Adolesc Med 164: 965-972.
- Morris RJ, Kratochwill TR (1991) The practice of child therapy (3rd edn). NY, USA: Pergamon p: 587.
- Muris P, Merckelbach H, Mayer B, Meesters C (1998) Common fears and their relationship to anxiety disorders symptomatology in normal children. Pers Individ Dif 24: 575-578.
- Beesdo K, Knappe S, Pine DS (2009) Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr Clin North Am 32: 483-524.
- Vasa RA, Pine DS (2004) Neurobiology. In: Morris TL, March JS (eds.) Anxiety disorder in childrens and adolescents (2nd edn.). New York: Guilford Press, pp: 3-26.
- Mogg K, Bradley BP (1998) A cognitive-motivational analysis of anxiety. Behav Res Ther 36: 809-848.
- Fox E (2002) Processing emotional facial expressions: the role of anxiety and awareness. Cogn Affect Behav Neurosci 2: 52-63.
- Bar-Haim Y, Lamy D, Pergamin L, Bakermans-Kranenburg MJ, Van Ijzendoorn MH (2007) Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull 133: 1.
- Leleu V, Douilliez C, Rusinek S (2014) Difficulty in disengaging attention from threatening facial expressions in anxiety: a new approach in terms of benefits. J Behav Ther Exp Psychiatry 45: 203-207.
- Cisler JM, Koster EH (2010) Mechanisms of attentional biases towards threat in anxiety disorders: an integrative review. Clin Psychol Rev 30: 203-216.
- Benoit KE, McNally RJ, Rapee RM, Gamble AL, Wiseman AL (2007) Processing of emotional faces in children and adolescents with anxiety disorders. Behav Change 24: 183-194.
- Reinholdt-Dunne ML, Mogg K, Esbjorn B, Bradley B (2011) Effects of age and anxiety on processing threat cues in healthy children. J Exp Psychopathol 3: 30-41.
- Vasey MW, Daleiden EL, Williams LL, Brown LM (1995) Biased attention in childhood anxiety disorders: a preliminary study. J Abnorm Child Psychol 23: 267-279.
- Hadwin JA, Donnelly N, Richards A, French CC, Patel U (2009) Childhood anxiety and attention to emotion faces in a modified stroop task. Brit J Dev Psychol 27: 487-494.
- Heim-Dreger U, Kohlmann CW, Eschenbeck H, Burkhardt U (2006) Attentional biases for threatening faces in children: vigilant and avoidant processes. Emotion 6: 320-325.
- Schwartz GM, Izard CE, Ansul SE (1985) The 5-month-old's ability to discriminate facial expressions of emotion. Infant Behav Dev 8: 65-77.
- Nelson CA (1987) The recognition of facial expressions in the first two years of life: Mechanisms of development. Child Dev pp: 889-909.
- Izard CE (1971) The Face of Emotion. New York: Appleton-Century Crofts.
- Camras LA, Allison K (1985) Children's understanding of emotional facial expressions and verbal labels. J Nonverbal Behav 9: 84-94.
- Denham SA, McKinley M, Couchoud EA, Holt R (1990) Emotional and behavioral predictors of preschool peer ratings. Child Dev 61: 1145-1152.
- Kirouac G, Doré F, Gosselin P (1985) Recognition of emotional facial expressions. Etholo Dev Child 131-147.
- Guyer AE, McClure EB, Adler AD, Brotman MA, Rich BA, et al. (2007) Specificity of facial expression labelling deficits in childhood psychopathology. J Child Psychol Psychiatry 48: 863-871.
- McClure EB, Pope K, Hoberman AJ, Pine DS, Leibenluft E (2003) Facial expression recognition in adolescents with mood and anxiety disorders. Am J Psychiatry 160: 1172-1174.
- Jarros RB, Salum GA, Belem da Silva CT, Toazza R, de Abreu Costa M, et al. (2012) Anxiety disorders in adolescence are associated with impaired facial expression recognition to negative valence. J Psychiatr Res 46: 147-151.
- Melfsen S, Florin I (2002) Do socially anxious children show deficits in classifying facial expressions of emotions? J Nonverbal Behav 26: 109-126.
- Simonian SJ, Beidel DC, Turner SM, Berkes JL, Long JH (2001) Recognition of facial affect by children and adolescents diagnosed with social phobia. Child Psychiatry Hum Dev 32: 137-145.
- Gifford-Smith ME, Brownell CA (2003) Childhood peer relationships: social acceptance, friendships, and peer networks. J Sch Psychol 41: 235-284.
- Easter J, McClure EB, Monk CS, Dhanani M, Hodgdon H, et al. (2005) Emotion recognition deficits in pediatric anxiety disorders: implications for amygdala research. J Child Adolesc Psychopharmacol 15: 563-570.
- Archer J, Hay DC, Young AW (1992) Face processing in psychiatric conditions. Br J Clin Psychol 31: 45-61.
- Gosselin P, Roberge P, Lavallée MF (1995) Le développement de la reconnaissance des expressions faciales émotionnelles du répertoire humain. Enfance 48: 379- 396.
- Keller MB, Lavori PW, Wunder J, Beardslee WR, Schwartz CE, et al. (1992) Chronic course of anxiety disorders in children and adolescents. J Am Acad Child Adolesc Psychiatry 31: 595-599.
- Britton JC, Lissek S, Grillon C, Norcross MA, Pine DS (2011) Development of anxiety: the role of threat appraisal and fear learning. Depress Anxiety 28: 5-17.
- Kindt M, Van Den Hout M (2001) Selective attention and anxiety: A perspective on developmental issues and the causal status. J Psychopathol Behav Assess 23: 193-202.
- Turgeon L, Chartrand É (2003) Reliability and validity of the revised children's manifest anxiety scale in a French-Canadian sample. Psychol Assessment 15: 378.
- Spielberger CD (1973) State-trait anxiety inventory for children. Consulting Psychologists Press.
- Muris P, Dreessen L, Bögels S, Weckx M, Melick M (2004) A questionnaire for screening a broad range of DSMâ€ÂÂÂÂdefined anxiety disorder symptoms in clinically referred children and adolescents. J Child Psychol Psychiatry 45: 813-820.
- Martin A, Gosselin P (2012) Propriétés psychométriques de l'adaptation francophone d'une mesure de symptômes des troubles anxieux auprès d'enfants et d'adolescents (SCARED-R). Can J Behav Sci J Behav Sci 44: 70.
- Langner O, Dotsch R, Bijlstra G, Wigboldus DH, Hawk ST, et al. (2010) Presentation and validation of the Radboud Faces Database. Cogn Emot 24: 1377-1388.
- Wild HA, Barrett SE, Spence MJ, O'Toole AJ, Cheng YD, et al. (2000) Recognition and sex categorization of adults' and children's faces: Examining performance in the absence of sex-stereotyped cues. J Exp Child Psychol 77: 269-291.
- Philippot P, Douilliez C (2005) Social phobics do not misinterpret facial expression of emotion. Behav Res Ther 43: 639-652.

