Keywords
Facility-based childbirth; Associated factors; Kombolcha Woreda
Background
Maternal mortality remains a major challenge to health systems worldwide. An estimated 303,000 maternal deaths occurred globally in 2015, yielding an overall MMR (Maternal Mortality Ratio) of 216 maternal deaths per 100,000 live births. Developing regions account for approximately 99% of the estimated global maternal deaths in 2015, with sub- Saharan Africa alone accounting for roughly 66% and Ethiopia accounting for 3.6% [1]. Most of these deaths are because of the lack of access to skilled childbirth attendances and emergency cares [2]. Around 80% of maternal deaths worldwide are brought about by such direct causes as hemorrhage, infection, obstructed labor, unsafe abortion and high blood pressure. Severe bleeding which usually occurs after the mother has given birth is the single most feared complication claiming the lives of most mothers [3].
The safe motherhood initiative strongly emphasizes on ensuring the availability and accessibility of skilled care during pregnancy and childbirth, of which facility-based childbirth is one element. Improving maternal and child health requires increasing the percentage of women giving birth in health institutions with the assistance of trained staff, which is the central goal of the safe motherhood and child survival movements [4].
As Ethiopian Demographic and Health Survey (EDHS 2011) has shown the maternal mortality was 676/100,000 live births, for the seven years period preceding the survey which was not significantly different from EDHS 2005 report 673/100,000 live birth. But there was steady decline in the MMR for the 7 years period preceding the surveys: from 871 deaths per 100,000 live births in the 2000 EDHS, to 673 deaths per 100,000 live births in the 2005 EDHS, and to 676 deaths in the 2011 EDHS, to reach 412 deaths per 100,000 live births in the 2016 EDHS [5- 7].
In Ethiopia, the proportions of births attended by skilled personnel are very much lower than sub-Saharan Africa. Even for women who have access to the services, the proportion of births occurring in health facilities is very low. Slightly over one in 4 live births in the five years preceding the survey were delivered by a skilled provider 28% or in a health facility 26% [2,5-7].
Facility-based childbirth in Oromia region was 4.3% in EDHS 2005 and increased to 8% in EDHS 2011 and 18.8% in EDHS 2016, which was much lower than the national level [5].
Even if there is physical access to facility-based childbirth, many women may not use them because of demographic and socioeconomic factors, health system organization, culture, gender, health seeking behavior, obstetric characteristics, education and other factors at individual, household, and community levels that shape an individual’s ability to seek health care.
However, few attempts have been made to show how these factors affect facility-based childbirth in Kombolcha Woreda. Therefore, this study aimed to identify determinants of facilitybased childbirth and associated factors in Kombolcha Woreda, Oromia Regional State, Ethiopia.
Methods
Study area and period
Community-based cross-sectional study was conducted from September 25 to October 15, 2014 in Kombolcha Woreda which is one of the 16 woreda in East Hararge Zone of Oromia Regional State, Ethiopia. The woreda is structured into 18 Rural and 2 urban kebeles with a total population of 170,000. Of these 86,238 are male and 83,902 are female. The number of women in the reproductive age (15-49) were estimated to be 37,652 and pregnant mothers add up to 6,295 per year. The woreda owned 4 health centers and 22 health posts. Health service coverage of the woreda was estimated to be 100% [8].
Sample size determination and sampling procedures
Women of child bearing age, who gave birth to at least one child within the past 24 months in Kombolcha Woreda, were the source population. The sample was estimated using sample size determination formula for single population proportion using the following assumptions. A facility-based childbirth proportion of 18.2%; and desired precision of 4%, 95% confidence level, design effect of two and 10% non-response rate were considered. With 10% non-response rate the final sample size was 785 [9].
Multi stage sampling method with stratification of the woreda into rural and urban areas was used in selecting the study subjects. Kombolcha Woreda had 18 rural and 2 urban kebeles (kebele is the smallest administrative unit in Ethiopia), 5 kebeles from the Rural and two kebele from the urban were selected by simple random sampling method. In the selected kebeles, households having the target were identified by house to house visit as a census. In the census, women who gave birth within the past 2 years in Kombolcha Woreda, and lived a minimum of 1 year in the woreda, prior to the survey was identified and this was used to randomly select the study subjects. The sample size was distributed to the seven kebeles proportionate to the size of their population. If more than one eligible woman were encountered in the household, a lottery method was used to determine the woman to be interviewed.
Data collection procedures
Structured and pre-tested questionnaire was prepared first in English and then translated into local language (Afan Oromo) for data collection. The Afan Oromo version was again translated back to English to check consistency and finally Afan Oromo version were used for the data collection. Six female diploma nurses conducted face to face interviews and one BSc. nurse supervised the data collection process. Training was given to the data collectors and supervisor before the actual data collection on the aim of the study, data collection tool and art of interviewing.
Data were collected on mothers’ age, marital status, place of residence, family income, educational status, occupation, educational status of the husband, occupation of the husband, facility-based childbirth, distance from health facility, family size, communication media possession, ANC (Antenatal Care) visit, parity and problems related to pregnancy.
Data processing and analysis
Each data were checked for completeness at field level, coded and were entered into Epi Info Version 3.5.1 database and checked for errors during data entry and exported to SPSS Version 20.0 for analysis. Data exploration was done to visualize the general feature of the data. After exploration, uni-variate, bivariate and multivariate analyses were performed step by step.
Binary and multiple logistic regressions were run to assess the associations of various factors with facility-based childbirth. The results were presented in the form of tables, figures and summary statistics. The strength of association of predictor variables with facility-based childbirth was assessed using odds ratio with 95% confidence interval.
Finally, multivariate analysis using forward stepwise multiple logistic regression technique was done to evaluate independent effect of each variable on facility-based childbirth by controlling the effect of others. A p-value <0.05 was considered as statistical significance.
Ethical considerations
Official permissions and letter of cooperation were obtained from Kombolcha Woreda Health Office, Kombolcha Woreda Administrative Office and Kombolcha Town Administrative. Study subjects were informed about the purpose of the study, their right to refuse and to withdraw. Written consent was obtained from each study subjects before data collection. Confidentiality was maintained by omitting personal identifications of respondents such as names from the questionnaire.
Results
A total of 785 mothers who gave birth in the last 12 months were interviewed; out of these 87.3% (n=685) were rural dwellers and 12.7% (n=100) were urban dwellers with 100% response rate. The mean age of the respondents was 26.34 years with a standard deviation (SD) of 4.68 years. 59.1% (n=464) of the mothers were in the age range of 20-29 years. The majority (93.8%) of the mothers were married. 64% (n=502) of the total mothers and 39.5% (n=291) of the total respondents’ husbands were illiterate. 58.4% (n=458) of the respondents had either radio or TV, and 41.6% (n=327) did not possess media of communication. 53% (n=416) of mothers had family size of less than or equal to five and 47% (n=369) had more than five individuals within the household (Table 1).
| Variables |
Frequency |
Percent (%) |
| Place of residence |
|
|
| Urban |
100 |
12.7 |
| Rural |
685 |
87.3 |
| Age of the mothers at interview |
|
|
| 15-19 |
39 |
5 |
| 20-24 |
195 |
24.8 |
| 25-29 |
269 |
34.3 |
| 30-34 |
161 |
20.5 |
| 35+ |
121 |
15.4 |
| Distance from health facility |
|
|
| ≤ 3 0min |
105 |
13.4 |
| 31 min-1 h |
546 |
69.6 |
| >1 h |
134 |
17 |
| Religion |
|
|
| Orthodox |
82 |
10.4 |
| Muslim |
689 |
87.8 |
| Protestant |
14 |
1.8 |
| Educational status of the mother |
|
|
| Unable to read and write |
502 |
64 |
| Primary education |
240 |
20 |
| Secondary and post-secondary |
43 |
5.5 |
| Occupational status of the mother |
|
|
| House wife |
633 |
80.7 |
| Government employee |
36 |
2.6 |
| Merchant/farmer |
116 |
5 |
| Occupational status of the husband (n=736) |
|
|
| Farmer |
578 |
78.6 |
| Government employee |
43 |
5.9 |
| Daily laborer/merchant other |
115 |
4.1 |
| Educational status of the husband (n=736) |
|
|
| Unable to read and write |
298 |
39.5 |
| Primary education |
332 |
30.8 |
| Secondary and post-secondary |
106 |
7.7 |
| Income in month in ETB |
|
|
| 100-499 |
180 |
22.9 |
| 500-999 |
386 |
49.1 |
| ≥ 1000 |
219 |
27.9 |
Table 1: Socio-demographic characteristics of the study participants, Kombolcha Woreda, East Hararghe Zone, Ethiopia, October, 2014.
Obstetric characteristics
76.1% (n=598) of the mothers had their first pregnancy before the age of 20 years. During the last pregnancy, 61% (n=479) of the mothers had at least one ANC (Antenatal Care) visit. Among the mothers who attended ANC, more than half (54%) of them visited health facilities two to three times. Out of the total respondents, only 14.2% (n=112) gave birth at health facilities (hospitals and health centers) and the vast majority (85.8%) delivered at home. Among the mothers who delivered at home, 69% (n=465) were assisted by their families or relatives; 20.7% (n=139) delivered with assistance of untrained TBA.
Of those who went to health facilities, 75% (n=84) delivered at health centers, (17.7% (n=20) at hospital, and the rest (7.3%) at private clinics (Table 2). Many different reasons were forwarded for home childbirth. 78% (n=525) said delivering at home is norm or usual practice (Figure 1).
| Variable |
Frequency |
Percent (%) |
| Age at first pregnancy (years) |
|
|
| <20 |
598 |
76.1 |
| ≥ 20 |
187 |
23.9 |
| Gravidity |
|
|
| 1 |
176 |
22.4 |
| 2-4 |
366 |
46.6 |
| ≥ 5 |
243 |
31 |
| Parity |
|
|
| One |
137 |
17.4 |
| Two-four |
386 |
49.2 |
| Five and above |
262 |
33.4 |
| Ever had abortion |
|
|
| Yes |
65 |
8.3 |
| No |
720 |
91.7 |
| ANC visit during previous pregnancy (n=609) |
|
|
| Yes |
256 |
42 |
| No |
353 |
58 |
| ANC visit during last pregnancy |
|
|
| Yes |
479 |
61 |
| No |
306 |
39 |
| Number of ANC visits to last pregnancy (n=479) |
|
|
| One |
50 |
10.4 |
| Two to three |
259 |
54 |
| Four and above |
170 |
35.6 |
| Place of last month childbirth |
|
|
| Home |
673 |
85.8 |
| Health facility |
112 |
14.2 |
| Assistance during home childbirth (n=673) |
|
|
| Family member |
465 |
69.0 |
| No one |
24 |
3.6 |
| Untrained TBAs |
139 |
20.7 |
| Others* |
45 |
6.7 |
| Reasons for childbirth at health facility (n=112) |
|
|
| For ANC service |
71 |
63.7 |
| For childbirth |
19 |
17.3 |
| For problems related to pregnancy |
17 |
15 |
| For problems not related to pregnancy |
7 |
6 |
| Problems faced during/before labor |
|
|
| Yes |
94 |
12 |
| No |
691 |
88 |
Notes: * Neighbors, non-relatives
Abbreviations: ANC: Antenatal Care; TBAs: Traditional Birth Attendants
Table 2: Obstetric characteristics and childbirth of the study participants, Kombolcha Woreda, East Hararghe Zone, Ethiopia, October, 2014.
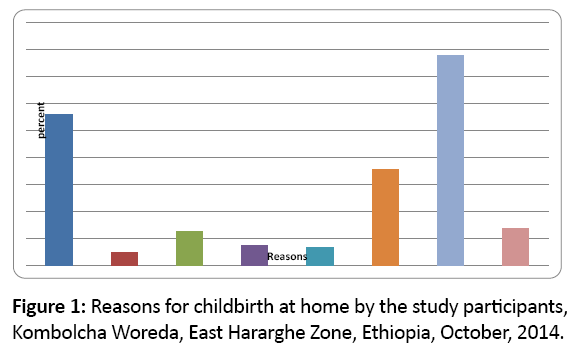
Figure 1: Reasons for childbirth at home by the study participants, Kombolcha Woreda, East Hararghe Zone, Ethiopia, October, 2014.
Factors associated with facility-based childbirth
On the bivariate analysis, facility-based childbirth was significantly associated with the age of mothers, residence, occupational and educational status of the mothers, and the occupational and educational status of the husbands as well as owning of TV or Radio, parity and ANC visit during the last pregnancy. From the variables found to be significant in the bivariate analysis, mothers’ age at interview, residence, educational status of couples, ANC visit during the last pregnancy, problem faced during pregnancy and parity were significantly associated with facility-based childbirth in multiple logistic regression analysis.
Mothers age between 15-24 years during the interview were about 4 times (AOR=4.23, 95% CI: 1.35, 20.29) more likely to deliver at health institutions than mothers more than 35 years and above. Urban mothers were about 3.4 times more likely to deliver at health institutions than rural mothers (AOR=3.44, 95% CI: 1.54, 7.40). Mothers with secondary education and above were 4.1 times more likely to deliver at health facilities as compared to those who were not able to read and write (AOR=4.13, 95% CI: 1.46, 11.73). Regarding the educational status of husbands, mothers whose husband attended secondary school and above were 2 times (AOR=2.05, 95% CI: 1.62, 8.32) more likely to deliver at health institutions as compared to mothers whose husbands were unable to read and write.
ANC visit during the last pregnancy was also found to be a strong predictor of facility-based childbirth. Mothers who visited health facilities for ANC during pregnancy were 4.2 times (AOR=4.22, 95% CI: 1.82, 11.65) more likely to deliver at health institutions than those who did not visit ANC during the last pregnancy. Parity was also another important factor which was associated with the place of childbirth. Mothers who delivered their first babies were 2.7 times more likely to utilize health institutions as compared to those who had five and more deliveries (AOR=2.67, 95% CI: 1.02, 4.86). Mothers who had problems during pregnancy were 2.2 times (AOR=2.21, 95% CI: 1.82, 9.65) more likely to deliver at health institutions than those who did not had health problems during pregnancy (Table 3).
| Variables |
Facility-based childbirth |
COR (95% C.I.) |
AOR (95%C.I.) |
| Yes |
No |
|
|
| Place of residence |
|
|
|
|
| Urban |
42 |
58 |
6.7 (3.52, 12.93)* |
3.44 (1.54, 7.40)** |
| Rural |
55 |
630 |
1 |
1 |
| Age of the mothers at interview |
|
|
|
|
| 15-24 |
69 |
165 |
9,89 (3.14, 31.03)* |
4.23 (1.35, 20.29)** |
| 25-34 |
44 |
386 |
2.73 (0.967, 7.8)* |
2.30 (0.89, 7.33) |
| 35+ |
12 |
109 |
1 |
1 |
| Educational status of mother |
|
|
|
|
| Unable to read and write |
45 |
457 |
1 |
1 |
| Primary education |
37 |
203 |
1.56 (0.91, 2.72) |
1.29 (0.65, 2.79) |
| Secondary education & above |
29 |
14 |
7.10 (3.18, 15.96)* |
4.13 (1.46, 11.73)** |
| Possessing TV & Radio |
|
|
|
|
| Yes |
65 |
393 |
2.54 (1.34, 4.71)* |
|
| No |
29 |
298 |
1 |
|
| ANC visit |
|
|
|
|
| Yes |
88 |
391 |
6.90 (3.04, 17.82)* |
4.22 (1.82, 11.65)** |
| No |
106 |
200 |
1 |
1 |
| Occupation of mother |
|
|
|
|
| House wife |
69 |
564 |
1 |
|
| Government employee |
17 |
19 |
10.82 (3.35, 35.03)* |
|
| Merchant/farmer |
16 |
100 |
1.43 (0.69, 2.98)* |
|
| Occupation of husband |
|
|
|
|
| Farmer |
53 |
525 |
1 |
|
| Government employee |
17 |
26 |
14.14 (5.16, 39.17)* |
|
| Merchant/daily laborer/other |
28 |
87 |
4.46 (2.19, 9.22)* |
|
| Educational status of husband |
|
|
|
|
| Unable to read and write |
28 |
270 |
1 |
|
| Primary education |
35 |
297 |
2.41 (1.23, 4.71) |
0.83 (0.46, 1.53) |
| Secondary education &above |
50 |
56 |
4.4 (3.46, 12.60)* |
2.05 (1.62, 8.32)** |
| Parity |
|
|
|
|
| 1 |
34 |
103 |
3.98 (2.16, 8.05)* |
2.67 (1.02, 4.86)* |
| 2-4 |
45 |
341 |
1.57 (0.82, 3.04) |
0.86 (0.49, 1.46) |
| >=5 |
19 |
243 |
1 |
1 |
| Problems faced during/before labor |
|
|
|
|
| Yes |
28 |
119 |
5.6 (3.21, 15.43)* |
2.21 (1.82, 9.65)** |
| No |
66 |
572 |
1 |
1 |
Notes: *Statistically significant at p<0.05, **statistically significant at p<0.05 when adjusted for other variables
Abbreviations: COR: Crude Odds Ratio; AOR: Adjusted Odds Ratio
Table 3: Bivariate and multivariate analysis of factors associated with facility-based childbirth in Kombolcha Woreda, East Hararghe Zone, Ethiopia, October, 2014.
Discussion
This study aimed to identify determinants of facility-based childbirth and associated factors in Kombolcha Woreda. The proportion of facility-based childbirth was 14.2% and mothers’ age at interview, residence, educational status of couples, ANC visit during the last pregnancy, parity and problem faced during pregnancy were significantly associated with facility-based childbirth.
The proportion of facility based childbirth in this study was higher than the national and the Oromia Region EDHS result of 2011 which were 10% and 8.0%, respectively, but lower than the national result of EDHS 2016 which was 18.8% [7,9]. This might be due to the time gap, i.e., since 2011 there might have been improvements in accessing and utilizing of the services.
The result was in line with studies done in Munesa Woreda and Sekela District in 2011, in which facility-based childbirth were 12.3% and 12.1%, respectively [10,11]. However, it was lower than studies conducted in Dodota Woreda, which was 18.2% [9]. This might be due the fact that there were differences in study area and population.
The current study also revealed that mothers’ place of residence was strongly associated with facility-based childbirth. Mothers who lived in urban kebeles were about 3.4 times more likely to deliver in health institutions as compared to those who lived in rural kebeles. The finding was consistent with EDHS 2011 and study done in Munesa and Dodota Woreda [9,10]. The study in Tigray Region and Nigeria also showed that urban/ rural differences had significant associations with the place of delivery [12,13]. This might be because in urban areas, the proportion of educated mothers was higher; accessibility to public and private clinic was higher and mothers could have better decision making autonomy than rural mothers. The ability to pay or cost of the services might also affect the women to utilize health facilities.
Maternal age was also one of the predictors of facilitybased childbirth. Mother’s age between 15-24 years during the interview were about 4 times more likely to deliver at health institutions than mothers more than 35 years and above. This finding was in line with the study done in North Gondar Zone which showed that utilization of delivery service was higher in younger age group (15-24 years) as compared to lower utilization of the services by mothers with age groups 25-34 years and 35 years and above [14]. This finding was also in consistent with studies done in Kenya, and Afghanistan which showed that younger women were more likely to utilize facilitybased childbirth as compared to older ones [15,16]. The possible explanation for this could be that younger women were more likely to be more literate than older women.
In this study, educational status of the mother had also significant association with facility-based childbirth. Women who attended secondary education and above were about 4.1 times more likely to deliver at the health institution when compared to women who were not able to read and write. This finding was similar to the study conducted in Sekela district on the utilization of facility-based childbirth which showed that mothers who attended secondary education and above were 12 times more likely to utilize delivery service than those mothers who had primary education and below [11]. This has also been recorded in other studies done in Dodota and Munesa Woreda, Ethiopia [9,10], Tanzania, Burkina Faso and Afghanistan [16- 18]. These might be due to the fact that educated women had better awareness about the benefits of utilization of facilitybased childbirth than rural women.
Another associated factor for utilization of health care for childbirth is the problem faced during or before labor. When a woman had difficulties in previous labor, the woman prefers to give birth in health facilities. These findings have also been documented in similar studies done in Dodota Woreda [9]; the fear of facing the same problem forces them to take precaution. Mothers might be more confident about the birth due to their experience of previous deliveries.
Husbands’ educational level was also one of the factors that predicted facility-based childbirth. This finding was in line with study done in Munesa Woreda, South-eastern Nigeria, and Northern Nigeria [10,13,19]. The possible explanation for this might be educated husbands might understand the benefits of giving birth at health facilities.
This study also revealed that mothers who had ANC visits during the last pregnancy were about 4.2 times more likely to give birth in health facilities than mothers who did not have any ANC visits during the last pregnancy. The result was consistent with other studies done in Gonder, Munesa, Sekela, Mali and Nepal, which revealed that those mothers who attended ANC were more likely to utilize delivery care services than those who did not attend ANC [10,11,14,20,21]. Counseling during pregnancy on the benefits of facility-based childbirth and risks of home childbirth could benefit these women.
Conclusion and Recommendation
This study revealed that the proportion of women who gave birth at health facilities in the woreda was low even though 61% of the mothers attended ANC services during their last pregnancy. A birth attended by skilled personnel is crucial in ensuring safe childbirth of mothers and hence reducing maternal death. However, large proportion (85.8%) of mothers gave birth at home without a skilled attendant.
ANC follow up and problems faced during the last pregnancy have shown significant association with facilitybased childbirth. Therefore, proper scaling up of ANC services; which is an entry point for other MCH services and follow up with special attention on counseling for problems that may occur during labor and safe facility-based childbirth is needed.
Besides these; changes in health system structure, improving accessibility, working on equity and empowering mothers is essential, and could help them in decision making regarding their own health, being committed to use the services and able to persuade their partner and family members if they encountered opposition.
Acknowledgement
Our appreciation goes to all staff members of Kombolcha Woreda Health Office for their kind assistance during the entire process of the study. We would also like to extend our appreciation to the study participants, supervisors and data collectors.
Authors’ Contributions
DB wrote the proposal, participated in data collection, entered and analyzed the data and drafted the paper. AT approved the proposal with some revisions, participated in data collection and revised subsequent drafts of the paper. All authors read and approved the final manuscript.
References
- Trends in maternal mortality (2015) Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division.
- World Health Organization (2012) Trends in maternal mortality: 1990 to 2010 Estimates developed by WHO, UNICEF, UNFPA and The World Bank. Geneva.
- Hogan MC, Foreman KJ, Naghavi M (2010) Maternal Mortality for 181 countries, 1980-2008: A systematic analysis of progress towards MDG5. Lancet. 375:1609-1623.
- Kesterton AJ, Cleland J, Sloggett A, Ronsmans C (2010) Institutional delivery in rural India: The relative importance of accessibility and economic status. BMC Pregnancy Childbirth. 10:30.
- Central Statistical Agency and ICF International (2012) Ethiopia demographic and health survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International.
- Central Statistical Agency and ORC Macro (2006) Ethiopia demographic and health survey 2005. Addis Ababa, Ethiopia and Calverton, Maryland, USA.
- Central Statistical Agency (CSA) and ICF (2016) Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia and Rockville, Maryland, USA. CSA and ICF.
- Kombolcha Woreda Health Office Data, 2014.
- Fikre, Demissie (2012) Prevalence of institutional delivery and associated factors in Dodota Woreda (district), Oromia regional state, Ethiopia. Reprod Health 9:33.
- Amano (2012) Institutional delivery service utilization in Munisa Woreda, South East Ethiopia: A community based cross-sectional study. BMC Pregnancy Childbirth. 12:105.
- Teferra (2012) Institutional delivery service utilization and associated factors among mothers who gave birth in the last 12 months in Sekela District, North West of Ethiopia: A community - based cross sectional study. BMC Pregnancy Childbirth. 12:74.
- Melaku (2014)Poor linkages in maternal health care services? Evidence on antenatal care and institutional delivery from a community-based longitudinal study in Tigray region, Ethiopia. BMC Pregnancy Childbirth 14:418.
- Onah HE, Ikeako LC, Iloabachie GC (2006) Factors associated with the use of maternity services in Enugu, south-eastern Nigeria. Soc Sci Med. 63:1870-1878.
- Mesfin N, Damen H, Getnet M (2004) Assessment of safe delivery service utilization among women of child bearing age in North Gondar Zone. EJHD. 18:146-150.
- Van E, Hanneke MB, Frank O (2006) Use of antenatal services and delivery care among women in rural Western Kenya: A community based survey. Reprod Health. 3:3.
- Mayhew M, Hansen M, Peters D (2008) Determinants of skilled birth attendant utilization in Afghanistan: A cross-sectional study. Am J Public Health. 98:1849-1856.
- Mrisho M, Schellenberg J, Mushi A, Obrist B, Mshinda H, et al. (2007) Factors affecting home delivery in rural Tanzania. Trop Med Int Health. 4:862-872.
- Hounton S, Chapman G, Ronsmans C (2008) Accessibility and utilization of delivery care within a skilled care initiative in rural Burkina Faso. Trop Med Int Health 6:44-52.
- Sheshu AU, Gwarzo, Indris SH (2006) Determinants of place of delivery among semi-urban women in Northern Nigeria. Ann Afr Med. 5:68-72.
- Gage AJ (2007) Barriers to the utilization of maternal health care in rural Mali. Soc Sci Med. 65:1666-1682.
- Wagle R, Sabroe S, Nielsen BB (2004) Socioeconomic and physical distance to the maternity hospital as predictors for place of delivery: An observational study from Nepal. BMC Pregnancy Childbirth. 4:8.

