Keywords
Gastroparesis; Pancreaticoduodenectomy; Pancreatic Fistula
Abbreviations
ISGPS International Study Group of Pancreatic Surgery
INTRODUCTION
Delayed gastric emptying remains one of the major causes of morbidity following pancreaticoduodenectomy despite continued improvements in perioperative patient management [1, 2, 3, 4, 5]. The true incidence of delayed gastric emptying until recently has been difficult to ascertain due to variations in definition [1, 2, 3, 4, 5].
Only recently have consensus guidelines been established by the International Study Group of Pancreatic Surgery (ISGPS) to define delayed gastric emptying and grade its severity [6]. Even in large series that utilize standard operative and reconstruction techniques, there is high variability in the incidence of delayed gastric emptying, based on ISGPS criteria, ranging from 14% to 45% [7, 8, 9]. It is conceivable that despite the set definitions, there may be underreporting of delayed gastric emptying.
The exact cause of delayed gastric emptying following pancreaticoduodenectomy appears to be multifactorial [10, 11, 12, 13, 14, 15]. Altered neuro-hormonal pathways, physiologic response to intra-abdominal sepsis or post pancreaticoduodenectomy associated acute pancreatitis and anatomic factors appear to play a role [16, 17, 18, 19]. Due to a lack of homogeneity between groups of patients studied and variations in definitions, definite conclusions regarding the variables that influence delayed gastric emptying cannot be reached [20].
Technical factors in the construction of the gastroenterostomy or duodenoenterostomy have been implicated in the development of delayed gastric emptying [16, 21, 22]. Significant edema or kinking at this anastomosis at either the afferent or efferent limb may be a factor in the development of delayed gastric emptying. Any potential obstruction at the level of this anastomosis following a standard reconstruction would increase biliary and pancreatic anastomotic outflow pressures. This could translate to an increase risk of pancreatic and biliary fistula and intra-abdominal sepsis.
Improved function of the gastroenterostomy or duodenoenterostomy may be possible with the formation enteroenterostomy between the afferent and efferent limbs distal to the gastroenterostomy or duodenoenterostomy. This was first reported by Braun over 100 years ago in the setting of gastric surgery, following formation of a gastroenterostomy, to divert bile from afferent limb and decrease reflux into the stomach [23]. The formation of Braun enteroenterostomy following classic pancreaticoduodenectomy potentially stabilizes and reduces kinking at the gastroenterostomy. Food passing through either the afferent or efferent limbs can progress distally through the Braun enteroenterostomy. It also directs pancreatic and biliary secretions away from the stomach, reducing exposure of the gastric mucosa to potentially irritating effects of bile. In cases of edema and kinking at the gastroenterostomy, the diverting ability of pancreatic and biliary secretions is maintained, without pressure increases in the biliopancreatic limb.
A change in reconstruction technique was undertaken utilizing the Braun enteroenterostomy following nonpylorus preserving pancreaticoduodenal resection with the aim of reducing delayed gastric emptying.
PATIENTS AND METHODS
Patient Population
All patients undergoing pancreaticoduodenectomy by a single surgeon (M.N.) from August 2009 to November 2011 were included in this study. Forty-four consecutive patients were included. To determine any possible benefit in delayed gastric emptying rates and overall outcomes the addition of Braun enteroenterostomy was introduced in August 2010, after20 non-pylorus preserving pancreaticoduodenal resections had been performed having determined a baseline delayed gastric emptying rate. Data were collected prospectively. Cross-checks were made between prospectively collected data and patient’s charts to re-confirm recorded findings.
Pre-Operative Details
Demographic data, laboratory tests and indications for surgery were recorded for all patients. Sodium picosulfate (Picoprep; Ferring Pharmaceuticals, Pymble, NSW, Australia) bowel preparation was administered the day prior to surgery.
Operative Details
All surgical procedures involved one lead surgeon (M.N.) with the reconstruction technique set-up has shown (Figure 1). Prophylactic antibiotics and subcutaneous heparin was administered in all cases. Antrectomy was performed as routine by use of linear stapler. A retrocolic limb jejunum was utilized for the pancreatic and biliary anastomoses. An end-to-side pancreaticojejunal two-layer anastomosis was formed.
Figure 1. a. Schematic diagram demonstrating that anatomy
following standard reconstruction, with an omental flap positioned
behind the gastrojejunal anastomosis compared to (b.) the anatomy
following reconstruction with the addition of Braun
enteroenterostomy.
The internal duct to mucosa reconstruction was created with interrupted 5/0 Maxonsutures (Covidien Pty. Ltd., Melbourne, Australia). An outer row of interrupted 3/0 Silk (Covidien Pty. Ltd., Melbourne, Australia) was used to approximate the pancreatic capsule parenchyma with the jejunal seromuscular layer. Anend- to-side hepaticojejunostomy was formed 10 to 15 cm distal to the pancreatic anastomosis using a single layer using 5/0 Maxon or 4/0 Vicryl (Johnson and Johnson Co., Melbourne, Australia) based on the duct diameter. An antecolic limb of intestine was the brought up to the stomach to create a gastroenterostomy in two-layer fashion spanning 5 to 6 cm (3/0 Vicryl and 3/0 Silk). A tongue of vascularized omentum was fashioned from the greater curve of the stomach to lay behind the gastroenterostomy as previously described [16].
A Braun enteroenterostomy, when performed, was constructed approximately 25 cm distal to the gastroenterostomy by a side to side stapled anastomosis, with two firings of 45 mm length vascular stapler in opposite directions. The enterotomy was closed in two layers (3/0 Vicryl and 3/0 Silk). The defect between the small bowel limbs and the mesentery was closed with interrupted 3/0 Silk sutures. Approximately 10 to 20 minutes was required to complete this anastomosis.
One round 19F silicon Blake® drain (Johnson and Johnson Co., Melbourne, Australia) was placed posterior to the biliary and one posterior to the pancreatic anastomoses and connected to low pressure closed bulb suction. A 16F nasogastric tube was inserted and positioned in the gastric fundus before the end of the case.
Post-Operative Details
A standard fast-track management protocol was utilized for all patients. Post-operatively all patients were treated in an intensive care unit (ICU) setting for only the first 12 to 24 hours, unless further monitoring was required. Antibiotics were ceased after 24 hours. Nasogastric tubes were routinely removed day 1 post operatively. A liquid diet was commenced day 2 post operatively. There was progression from fluid intake to a soft diet as tolerated over the next few days. The right and left drains were checked for amylase and bilirubin at day 5 and were removed if there was no evidence of any pancreatic or biliary leakage. In all cases erythromycin lactobionate (Link Medical Products Pty. Ltd, Clareville, NSW, Australia) was given intravenously at 200 mg every 6 hours starting on day 2 post-operatively and continued until a soft diet was tolerated. Jejunal feeding tubes were only inserted in patients considered to be malnourished and in whom a period of additional nutritional supplementation was through be required. A proton pump inhibitor was administered intravenously following surgery and converted to oral dosage once a diet was tolerated and continued for at least two weeks post discharge. Pancreatic enzyme supplements were prescribed once a soft diet was commenced. This was continued postoperatively with the dosage altered according to symptoms. Tight serum glucose control was maintained post-operatively by use of an insulin sliding scale. Patients were discharged after day 7 if they were self-caring, had no evidence of an infection and were tolerating a diet.
Operative details including operative time, estimated blood loss, pancreatic texture and pancreatic duct diameter were recorded.
Complications
The primary end point of this study was delayed gastric emptying. This was defined according to the International Study Group of Pancreatic Surgery (ISGPS) as the inability to return to a standard diet by day 7 post-operatively or reinsertion of a nasogastric tube prior to this period [6]. In cases of delayed gastric emptying the severity was defined. All other specific complications were defined according to ISGPS criteria where available [8, 24]. In particular, pancreatic fistula was defined as any measurable amount of fluid after post-operative day 3 with an amylase level 3 times or greater than serum amylase [25]. Patients in whom intra-abdominal collections required drainage in the perioperative period were considered to have high impact pancreatic fistula, unless another explanation was clearly available. Mortality was defined as death within 30 days after surgery.
ETHICS
Institutional review board (IRB) approval was obtained for review of patient data and conforms to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008. Standard consent for surgery was undertaken.
STATISTICS
Results were expressed as median (range) unless otherwise stated. Comparisons between categorical variables were determined by the chi square, the linearby- linear association and the Fisher’s exact tests as appropriate. Non-categorical variables were assessed by the Mann-Whitney U test. Multivariate analysis using a backward regression model was undertaken to determine factors independently associated with delayed gastric emptying including all factors where the P value was less than 0.1 on univariate analysis. A statistical software package (SPSS Version 18.0, Chicago, IL, USA) was used for statistical analysis, with P<0.05 considered statistically significant.
RESULTS
Patient Characteristics
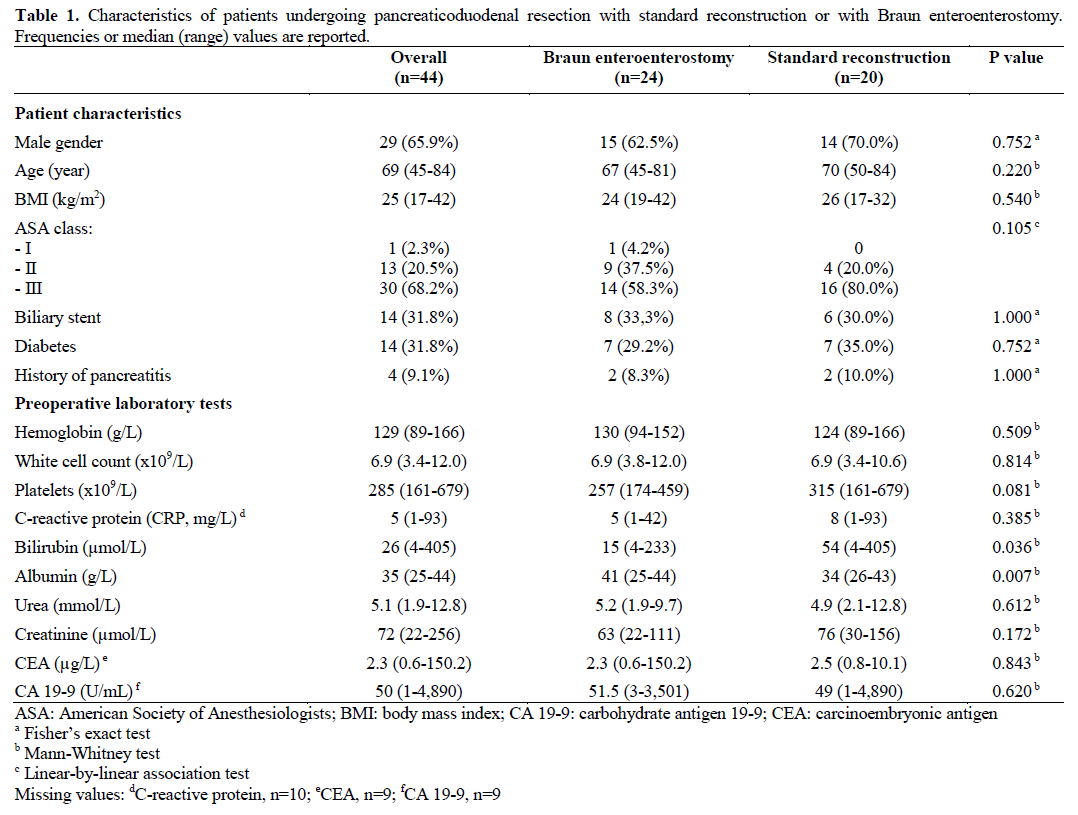
The characteristics of the patient treated in each group are shown in Table 1. There were 24 patients in the Braun enteroenterostomy group and 20 in the standard reconstruction group during the study period. There were no significant differences in demographic characteristics. The median bilirubin level at the time of diagnosis was significantly lower in the Braun enteroenterostomy group (15 μmol/L, range: 4-233 μmol/L vs. 54 μmol/L, range: 4-405 μmol/L; P=0.036), while the albumin level was significantly higher (41 g/L , range: 25-44 g/L vs. 34 g/L, range: 26-43 g/L; P=0.007). There were no other significant differences in laboratory variables.
Operative and Perioperative Variables
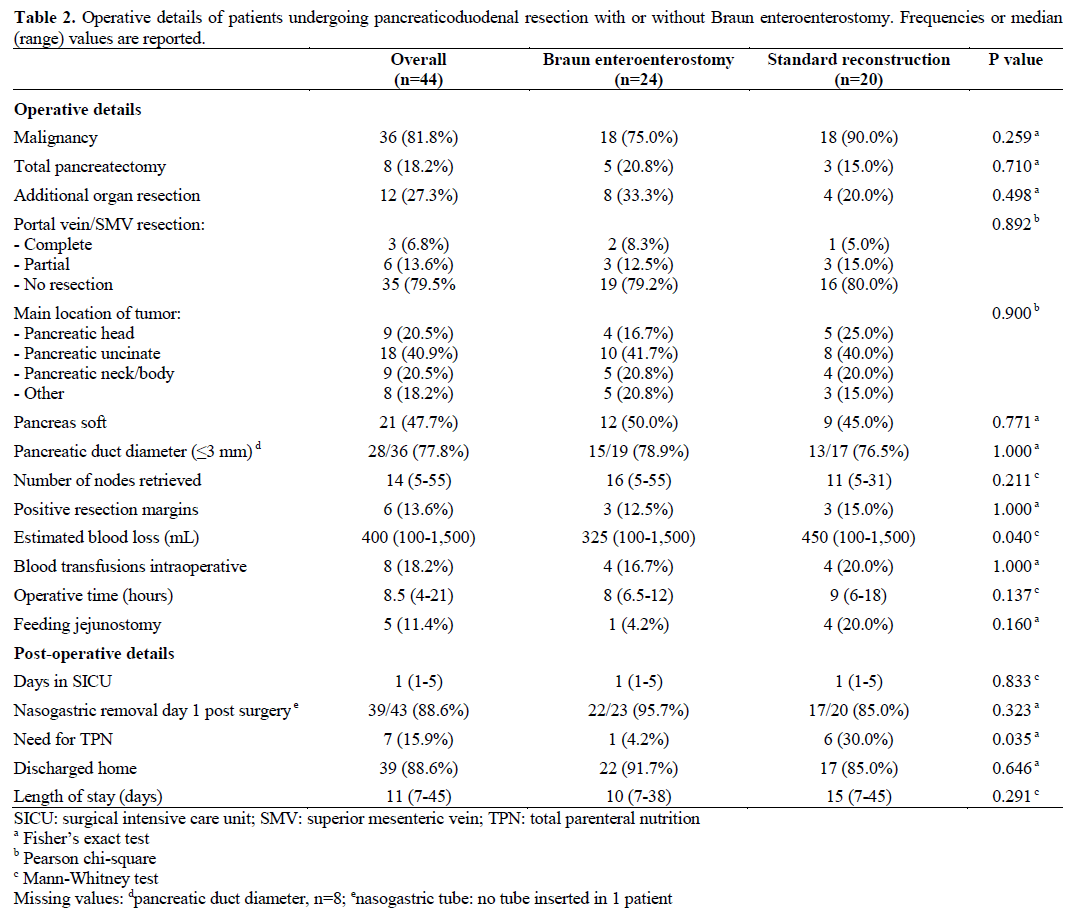
Operative and perioperative details are summarized in Table 2. In this series the main tumor location was within the pancreatic uncinate process in 40.9% of cases. There were no major differences between the groups in terms of tumor type, location, pancreatic texture, pancreatic duct size, resection margins and the number of nodes harvested. The median estimated blood loss was lower in the Braun enteroenterostomy group (325 mL, range: 100-1,500 mL vs. 450 mL, range: 100-1,500 mL; P=0.040); however, the intraoperative blood transfusion requirements were similar. Post-operative length of intensive care stay and overall length of hospital stay was similar. Patients in the Braun enteroenterostomy group less frequently required total parenteral nutrition (TPN) during the course of their management (1/24, 4.2% vs. 6/20, 30.0%; P=0.035).
Complications
Complication data are shown in Table 3. There was one mortality in the standard reconstruction group in this series (4.2%). This was in a 65-year-old patient with advanced bile duct cancer treated by right trisegmental and caudate liver resection combined with pancreaticoduodenectomy. The patient died of massive sudden intra-abdominal hemorrhage at day 8 post operatively, presumed secondary to ruptured pseudoaneurysm.
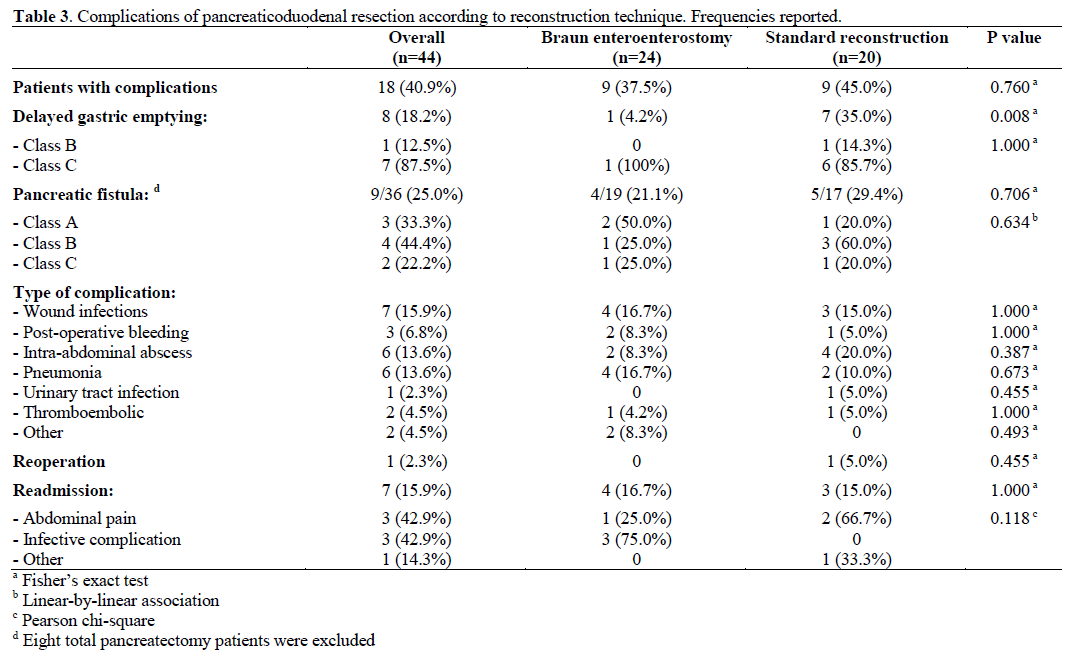
Overall complications between the groups were similar except for delayed gastric emptying. The delayed gastric emptying rate was significantly lower in the Braun enteroenterostomy group (1/24, 4.2% versus 7/20, 35.0%; P=0.008). In the Braun enteroenterostomy group delayed gastric emptying occurred in a 78-yearold man following a total pancreatectomy performed for multifocal intraductal mucinous neoplasia. The patient had long-standing insulin dependent diabetes pre-operatively. Post operatively he developed significant gastro-intestinal bleeding of unknown etiology. There was no evidence of pseudoaneurysm on CT imaging and upper gastrointestinal endoscopy showed no evidence of bleeding and patent gastroenterostomy. The bleeding stopped without treatment, but the patient developed significant delayed gastric emptying and required several weeks of TPN before return of normal gastric functioning. None of the three patients undergoing total pancreatectomy in the first 20 patients prior to the introduction of Braun enteroenterostomy had delayed gastric emptying.
The overall pancreatic fistula rate excluding the eight patients who had a total pancreatectomy in this series was 25.0%. The fistula was graded as class A in 33.3% of cases. There were no significant differences between the groups, although in the Braun enteroenterostomy group 50.0% of fistulas were class A compared to 20.0% in the standard group.
There were no other significant differences in complications between the groups. No complication was attributed to Braun enteroenterostomy. Readmission rates were similar between the groups.
Factors Associated with Delayed Gastric Emptying
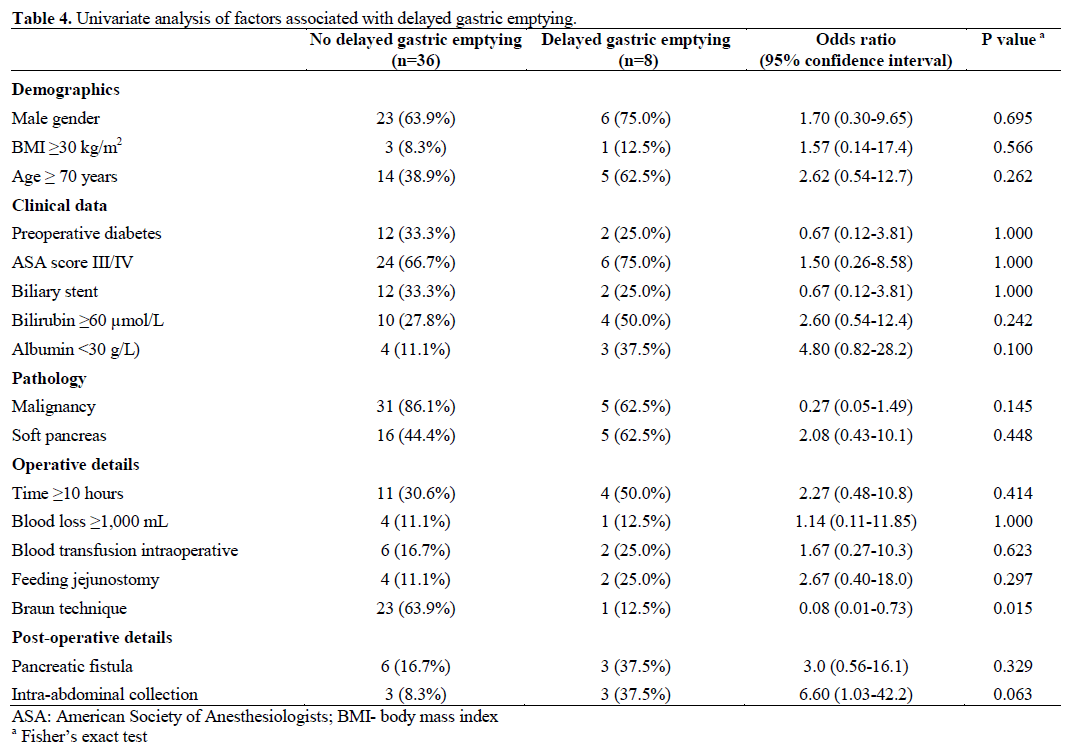
The association of various factors with delayed gastric emptying by univariate analysis is shown in Table 4. Braun enteroenterostomy was the only significant factor associated with delayed gastric emptying with an odds ratio of 0.08 (95% confidence interval: 0.01-0.73) (P=0.015). A trend toward increased delayed gastric emptying was noted in patients with intra-abdominal collections, with an odds ratio of 6.60 (95% confidence interval: 1.03-42.2) (P=0.063). At multivariate analysis (including Braun enteroenterostomy and intraabdominal infection as the factors with a significance of p<0.1) Braun enteroenterostomy was the only independent factor associated with reduced delayed gastric emptying with an odds ratio of 0.08 (95% confidence interval: 0.01-0.73) (P=0.025).
DISCUSSION
Delayed gastric emptying continues to be a common problem after pancreaticoduodenal resection. The incidence is higher than previously reported if it is defined using strict ISGPS criteria in centers performing standard pancreaticoduodenal resection and reconstruction techniques [7, 8, 9]. Theories regarding the causes of delayed gastric emptying include: pyloric, antral and duodenal ischemia [26, 27], gastroparesis related to abdominal complications [10, 12, 28, 29, 30, 31, 32], post-operative pancreatitis associated pancreatic leak or ilues [19, 33], disruption of hormone and neuronal homeostasis mechanisms [12, 15, 17, 20, 34, 35, 36, 37, 38, 39], pylorspasm [18, 40] and torsion or angulation at the gastroenterostomy or duodenoenterostomy [21, 26, 41].
In our study all patients underwent antral resection as the preferred technique. This allowed consistent gastrojejunostomy reconstruction with no major issues regarding anastomotic blood supply. We acknowledge that there are some reports of long-term advantages of pylorus preservation, including earlier recovery of body weight, reduced diarrhea, and reduction in dumping symptoms [32, 42, 43]. This is however not supported by all studies [44]. Several studies have suggested decreased delayed gastric emptying antral resection [45, 46, 47]. However, most large series suggest that there is no difference in delayed gastric emptying between pylorus preservation and antral resection [48, 49].
A change in technique was performed in an attempt to reduce delayed gastric emptying rates. All operations were performed using the same technique, with the only difference being the addition of Braun enteroenterostomy in some patients. It could however be argued that improvements in results may reflect a learning curve [50]. All these cases were performed by one surgeon after completion of fellowship training in high volume pancreatic surgery centers. A learning curve is unlikely to provide an adequate explanation, given that all other complications remained the same, including the overall pancreatic fistula rate. There was a reduction in estimated blood loss in the Braun enteroenterostomy group, which was not clinically significant. We acknowledge that our study suffers from a lack of randomization and it was performed in a single institution during two separate time periods. All patients however had a uniform operative technique and there was no selective use of a particular method, with the first 20 consecutive patients treated by standard reconstruction and the next 24 consecutive patients having the addition of a Braun enteroenterostomy. In this series there was a planned change of technique to determine if there was benefit in performing a Braun enteroenterostomy, rather than a change of technique due to the discovery of a particular problem. No patients were excluded from this study.
The Braun enteroenterostomy has several potential benefits. Once the Braun enteroenterostomy anastomosis is completed and the space between the mesenteric limbs is closed with sutures, this tends to stabilize the afferent and efferent limbs of the gastrojejunostomy. The gastrojejunostomy itself becomes more stabilized, with a low tendency to twist and angulate. In cases of an obstruction at the level of the gastroenterostomy, the Braun enteroenterostomy ensures that there is no increase in pressure in the biliopancreatic limb. This may theoretically reduce the incidence or severity of a pancreatic fistula, although a difference in pancreatic fistula rate was not observed in our series. The Braun enteroenterostomy, as with a Roux-en-Y anastomosis reduces alkaline reflux into the stomach, which may have an irritant effect. The lack of division of the small bowel in cases of Braun enteroenterostomy avoids disruption of myoelectric activity of the gut [51]. The Braun enteroenterostomy allows a gastric content that passes into either the efferent or afferent limb of the gastroenterostomy to pass distally unimpeded. Kinking at either of these limbs alone theoretically would not alter gastric emptying in these circumstances.
There is one report by Hochwald et al. of the use of Braun enteroenterostomy following pancreaticoduodenectomy to reduce delayed gastric emptying [52]. Five different surgeons contributed to this study with slight variations on management protocols. The study examined patients undergoing classic pancreaticoduodenectomy over a five-year period from 2001 to 2006. There were 35 patients undergoing standard reconstruction compared to 70 with the addition of Braun enteroenterostomy, with a significant reduction in delayed gastric emptying (10% versus 26%; P<0.05). This was based on a delayed gastric emptying definition of an inability to take liquid or solid food by postoperative day 10. When the ISGPS definition was used the delayed gastric emptying rate increased, but it remained lower in the Braun enteroenterostomy group (36% versus 60%; P=0.02). Multivariate analysis was not utilized to examine for factors associated with delayed gastric emptying. Our report of delayed gastric emptying based on the ISPS criteria was lower than this study. The technique utilized in our series was similar to that reported by Hochwald et al., with the exception of placement of a vascularized omental pedicle behind the gastroenterostomy and routine administration of erythromycin post-operatively. There is also a report of reduced delayed gastric emptying in small cohort study utilizing a Braun enteroenterostomy with stapling of the afferent limb of the gastrojejunostomy in the setting of classic pancreaticoduodenal resection [53]. This reconstruction, referred to as uncut Roux-en-Y gastrojejunostomy, was utilized in 13 patients without any case of delayed gastric emptying. The authors of that paper felt that this reconstruction was better than a standard Roux-en-Y reconstruction as it maintained the small bowel integrity, and did not disrupt the myoelectric activity of the small bowel. We do not consider stapling the afferent limb of the gastrojejunostomy to be of any benefit, as this limb provides a route through which gastric contents can pass in cases of kinking or obstruction of the efferent limb.
CONCLUSION
Our study suggests that the use of Braun enteroenterostomy leads to significant reductions in the incidence of delayed gastric emptying following pancreaticoduodenal resection. The technique adds very little to overall operative time and itself does not appear to cause increased morbidity. A randomized control trial is required to fully confirm the potential advantages of Braun enteroenterostomy in reducing delayed gastric emptying.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Pratt W, Joseph S, Callery MP, Vollmer CM, Jr. POSSUM accurately predicts morbidity for pancreatic resection. Surgery 2008;143(1): 8-19.
- Lowy AM, Lee JE, Pisters PW, Davidson BS, Fenoglio CJ, Stanford P, Jinnah R, Evans DB. Prospective, randomized trial of octreotide to prevent pancreatic fistula after pancreaticoduodenectomy for malignant disease. Ann Surg 1997;226(5): 632- 641.
- DeOliveira ML, Winter JM, Schafer M, Cunningham SC, Cameron JL, Yeo CJ, Clavien PA. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann Surg 2006;244(6): 931- 937; discussion 937-939.
- Grobmyer SR, Pieracci FM, Allen PJ, Brennan MF, Jaques DP. Defining morbidity after pancreaticoduodenectomy: use of a prospective complication grading system. J Am CollSurg 2007;204(3): 356-364.
- BalcomJHt, Rattner DW, Warshaw AL, Chang Y, Fernandezdel Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg 2001;136(4): 391-398.
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG, Traverso LW, Yeo CJ, Buchler MW. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007;142(5): 761- 768.
- Malleo G, Crippa S, Butturini G, Salvia R, Partelli S, Rossini R, Bacchion M, Pederzoli P, Bassi C. Delayed gastric emptying after pylorus-preserving pancreaticoduodenectomy: validation of International Study Group of Pancreatic Surgery classification and analysis of risk factors. HPB (Oxford) 2010;12(9): 610-618.
- Tan WJ, Kow AW, Liau KH. Moving towards the New International Study Group for Pancreatic Surgery (ISGPS) definitions in pancreaticoduodenectomy: a comparison between the old and new. HPB (Oxford) 2011;13(8): 566-572.
- Welsch T, Borm M, Degrate L, Hinz U, Buchler MW, Wente MN. Evaluation of the International Study Group of Pancreatic Surgery definition of delayed gastric emptying after pancreatoduodenectomy in a high-volume centre. Br J Surg 2010;97(7): 1043-1050.
- Miedema BW, Sarr MG, van Heerden JA, Nagorney DM, McIlrath DC, Ilstrup D. Complications following pancreaticoduodenectomy. Current management. Arch Surg 1992;127(8): 945-949; discussion 949-950.
- Hocking MP, Harrison WD, Sninsky CA. Gastric dysrhythmias following pylorus-preserving pancreaticoduodenectomy. Possible mechanism for early delayed gastric emptying. Dig Dis Sci 1990;35(10): 1226-1230.
- Braasch JW, Deziel DJ, Rossi RL, Watkins E, Jr., Winter PF. Pyloric and gastric preserving pancreatic resection. Experience with 87 patients. Ann Surg 1986;204(4): 411-418.
- Liberski SM, Koch KL, Atnip RG, Stern RM. Ischemic gastroparesis: resolution after revascularization. Gastroenterology 1990;99(1): 252-257.
- Martignoni ME, Friess H, Sell F, Ricken L, Shrikhande S, Kulli C, Buchler MW. Enteral nutrition prolongs delayed gastric emptying in patients after Whipple resection. Am J Surg 2000;180(1): 18-23.
- Tanaka M, Sarr MG. Role of the duodenum in the control of canine gastrointestinal motility. Gastroenterology 1988;94(3): 622- 629.
- Nikfarjam M, Kimchi ET, Gusani NJ, Shah SM, Sehmbey M, Shereef S, Staveley-O'Carroll KF. A reduction in delayed gastric emptying by classic pancreaticoduodenectomy with an antecolicgastrojejunal anastomosis and a retrogastricomental patch. J GastrointestSurg 2009;13(9): 1674-1682.
- Lytras D, Paraskevas KI, Avgerinos C, Manes C, Touloumis Z, Paraskeva KD, Dervenis C. Therapeutic strategies for the management of delayed gastric emptying after pancreatic resection. Langenbecks Arch Surg 2007;392(1): 1-12.
- Kawai M, Tani M, Hirono S, Miyazawa M, Shimizu A, Uchiyama K, Yamaue H. Pylorus ring resection reduces delayed gastric emptying in patients undergoing pancreatoduodenectomy: a prospective, randomized, controlled trial of pylorus-resecting versus pylorus-preserving pancreatoduodenectomy. Ann Surg 2011;253(3): 495-501.
- Raty S, Sand J, Lantto E, Nordback I. Postoperative acute pancreatitis as a major determinant of postoperative delayed gastric emptying after pancreaticoduodenectomy. J GastrointestSurg 2006;10(8): 1131-1139.
- Traverso LW, Hashimoto Y. Delayed gastric emptying: the state of the highest level of evidence. J HepatobiliaryPancreatSurg 2008;15(3): 262-269.
- Masui T, Doi R, Kawaguchi Y, Uemoto S. Delayed gastric emptying improved by straight stomach reconstruction with twisted anastomosis to the jejunum after pylorus-preserving pancreaticoduodenectomy (PPPD) in 118 consecutive patients at a single institution. Surg Today 2011.
- Tani M, Terasawa H, Kawai M, Ina S, Hirono S, Uchiyama K, Yamaue H. Improvement of delayed gastric emptying in pyloruspreservingpancreaticoduodenectomy: results of a prospective, randomized, controlled trial. Ann Surg 2006;243(3): 316-320.
- Braun H. UeberdieGasto-enteostomie und gleichzeutigausgefuhrteEntero-anastomose. Arch KlinChir 1893;45: 361.
- Pratt WB, Maithel SK, Vanounou T, Huang ZS, Callery MP, Vollmer CM, Jr. Clinical and economic validation of the International Study Group of Pancreatic Fistula (ISGPF) classification scheme. Ann Surg 2007;245(3): 443-451.
- Bassi C, Falconi M, Molinari E, Salvia R, Butturini G, Sartori N, Mantovani W, Pederzoli P. Reconstruction by pancreaticojejunostomy versus pancreaticogastrostomy following pancreatectomy: results of a comparative study. Ann Surg 2005;242(6): 767-771, discussion 771-763.
- Itani KM, Coleman RE, Meyers WC, Akwari OE. Pyloruspreservingpancreatoduodenectomy. A clinical and physiologic appraisal. Ann Surg 1986;204(6): 655-664.
- Kurosaki I, Hatakeyama K. Preservation of the left gastric vein in delayed gastric emptying after pylorus-preserving pancreaticoduodenectomy. J GastrointestSurg 2005;9(6): 846-852.
- Haddad O, Porcu-Buisson G, Sakr R, Guidicelli B, Letreut YP, Gamerre M. Diagnosis and management of adenocarcinoma of the ampulla of Vater during pregnancy. Eur J ObstetGynecolReprodBiol 2005;119(2): 246-249.
- Horstmann O, Becker H, Post S, Nustede R. Is delayed gastric emptying following pancreaticoduodenectomy related to pylorus preservation? Langenbecks Arch Surg 1999;384(4): 354-359.
- Horstmann O, Markus PM, Ghadimi MB, Becker H. Pylorus preservation has no impact on delayed gastric emptying after pancreatic head resection. Pancreas 2004;28(1): 69-74.
- Riediger H, Makowiec F, Schareck WD, Hopt UT, Adam U. Delayed gastric emptying after pylorus-preserving pancreatoduodenectomy is strongly related to other postoperative complications. J GastrointestSurg 2003;7(6): 758-765.
- Hunt DR, McLean R. Pylorus-preserving pancreatectomy: functional results. Br J Surg 1989;76(2): 173-176.
- Lin PW, Lin YJ. Prospective randomized comparison between pylorus-preserving and standard pancreaticoduodenectomy. Br J Surg 1999;86(5): 603-607.
- Meyer BM, Werth BA, Beglinger C, Hildebrand P, Jansen JB, Zach D, Rovati LC, Stalder GA. Role of cholecystokinin in regulation of gastrointestinal motor functions. Lancet 1989;2(8653): 12-15.
- Fox JE, Daniel EE, Jury J, Robotham H. The mechanism of motilin excitation of the canine small intestine. Life Sci 1984;34(10): 1001-1006.
- Naritomi G, Tanaka M, Matsunaga H, Yokohata K, Ogawa Y, Chijiiwa K, Yamaguchi K. Pancreatic head resection with and without preservation of the duodenum: different postoperative gastric motility. Surgery 1996;120(5): 831-837.
- Tait IS. Whipple's resection-proximal pancreaticoduodenectomy (PD). J R CollSurgEdinb 2002;47(3): 528-540.
- Tanaka M, Sarr MG. Total duodenectomy: effect on canine gastrointestinal motility. J Surg Res 1987;42(5): 483-493.
- Kim HC, Suzuki T, Kajiwara T, Miyashita T, Imamura M, Tobe T. Exocrine and endocrine stomach after gastrobulbar preserving pancreatoduodenectomy. Ann Surg 1987;206(6): 717-727.
- Kim DK, Hindenburg AA, Sharma SK, Suk CH, Gress FG, Staszewski H, Grendell JH, Reed WP. Is pylorospasm a cause of delayed gastric emptying after pylorus-preserving pancreaticoduodenectomy? Ann SurgOncol 2005;12(3): 222-227.
- Ueno T, Tanaka A, Hamanaka Y, Tsurumi M, Suzuki T. A proposal mechanism of early delayed gastric emptying after pylorus preserving pancreatoduodenectomy. Hepatogastroenterology 1995;42(3): 269-274.
- Traverso LW, Longmire WP, Jr. Preservation of the pylorus in pancreaticoduodenectomy a follow-up evaluation. Ann Surg 1980;192(3): 306-310.
- Pitt HA, Grace PA. Cancer of the pancreas. Pylorus-preserving resection of the pancreas. Baillieres ClinGastro enterol 1990;4(4): 917-930.
- Han SS, Kim SW, Jang JY, Park YH. A comparison of the longterm functional outcomes of standard pancreatoduodenectomy and pylorus-preserving pancreatoduodenectomy. Hepatogastroenterology 2007;54(78): 1831-1835.
- van Berge Henegouwen MI, van Gulik TM, DeWit LT, Allema JH, Rauws EA, Obertop H, Gouma DJ. Delayed gastric emptying after standard pancreaticoduodenectomy versus pylorus-preserving pancreaticoduodenectomy: an analysis of 200 consecutive patients. J Am CollSurg 1997;185(4): 373-379.
- Patel AG, Toyama MT, Kusske AM, Alexander P, Ashley SW, Reber HA. Pylorus-preserving Whipple resection for pancreatic cancer. Is it any better? Arch Surg 1995;130(8): 838-842; discussion 842-833.
- Lin PW, Shan YS, Lin YJ, Hung CJ. Pancreaticoduodenectomy for pancreatic head cancer: PPPD versus Whipple procedure. Hepatogastroenterology 2005;52(65): 1601-1604.
- Alsaif F. Pylorus preserving pancreaticoduodenectomy for periampullary carcinoma, is it a good option? Saudi J Gastroenterol 2010;16(2): 75-78
- Tran KT, Smeenk HG, van Eijck CH, Kazemier G, Hop WC, Greve JW, Terpstra OT, Zijlstra JA, Klinkert P, Jeekel H. Pylorus preserving pancreaticoduodenectomy versus standard Whipple procedure: a prospective, randomized, multicenter analysis of 170 patients with pancreatic and periampullary tumors. Ann Surg 2004;240(5): 738-745.
- Hardacre JM. Is there a learning curve for pancreaticoduodenectomy after fellowship training? HPB Surg2010;2010: 230287.
- Tu BN, Sarr MG, Kelly KA. Early clinical results with the uncut Roux reconstruction after gastrectomy: limitations of the stapling technique. Am J Surg 1995;170(3): 262-264.
- Hochwald SN, Grobmyer SR, Hemming AW, Curran E, Bloom DA, Delano M, Behrns KE, Copeland EM, Vogel SB. Braun enteroenterostomy is associated with reduced delayed gastric emptying and early resumption of oral feeding following pancreaticoduodenectomy. J SurgOncol 2010;101(5): 351-355.
- Wayne MG, Jorge IA, Cooperman AM. Alternative reconstruction after pancreaticoduodenectomy. World J SurgOncol 2008;6: 9.


