Keywords
Carcinoma; Neoplasms, Second Primary; Pancreas; Pancreatectomy; Recurrence
Abbreviations
CA: carbohydrate antigen; JPS: Japan Pancreas Society; PPPD: pylorus-preserving pancreaticoduodenectomy
INTRODUCTION
Invasive ductal carcinomas of the pancreas often develop extra-pancreatic growths to the pancreatic bed, major vessels, neural plexus and adjacent organs, and can also develop distant metastases. Unless treated during the early stages, most pancreatic carcinomas eventually become intractable. Long-term survival is rare in pancreatic carcinoma patients, and high recurrence rates are observed even in R0 cases. Although surgical resection is the only curative therapeutic option for recurrent or metachronous pancreatic carcinomas, most such cancers are beyond surgical curability. Remnant or repeated pancreatectomy for recurrent or metachronous pancreatic carcinomas is extremely rare, with only a few cases having been reported in the literature [1, 2, 3, 4, 5]. A second resection for recurrent or metachronous pancreatic carcinoma remains under consideration.
The present report describes two cases in which remnant pancreatectomy was used to treat recurrent or metachronous pancreatic carcinoma. The use of FDGPET was a key factor in the detection of the lesions. Both patients were alive at least 8 months after surgery.
CASE REPORTS
Case#1
A 65-year-old man showed a dilatation of the main pancreatic duct on abdominal US at an annual medical checkup. An abdominal CT scan showed a 1 cm tumor in the head of the pancreas (Figure 1a), and dilatation of the main pancreatic duct in the distal part of the pancreas was demonstrated by MRCP (Figure 1b). A pylorus-preserving pancreaticoduodenectomy (PPPD) was performed in December 2000. The tumor was confirmed histopathologically to be a welldifferentiated adenocarcinoma without lymph node metastasis (T1N0M0; R0; pathological stage: IA) (Figure 1c). Although the surgical margins were negative, pancreatic intraepithelial neoplasia was present in the resected pancreas. Adjuvant chemotherapy (4 cycles of 5-fluorouracil, leucovorin and mitomycin C given intravenously) was administered for 4 months. Periodic check-ups were performed thereafter.
Figure 1. Case#1: initial operation. a. A tumor approximately 1 cm
in diameter was detected in the pancreatic head on abdominal CT
(arrow). b. The main pancreatic duct was disrupted, and the main
pancreatic duct of the distal pancreas was dilated on MRCP. c. Welldifferentiated
tubular carcinoma. Marked fibrosis and acinus atrophy
were observed. Mild atypical cells with a slightly swollen nucleus
formed an irregular ductal structure and invaded the parenchyma.
(H&E stain, x100).
In January 2008, the patient complained of hydrodipsia and polyuria, and was diagnosed with diabetes mellitus. An abdominal CT scan revealed a 3 cm tumor in the tail of the pancreas (Figure 2a). Tumor marker (CEA and carbohydrate antigen (CA) 19-9) levels were within the reference limits, and had been throughout previous monitoring. Recurrence was confirmed using FDG-PET at 84 months after the initial operation. The FDG-PET hot spot corresponded with the tumor location shown by the CT scan (Figure 2b). The patient underwent surgery in June 2008. An intra-operative pathological examination indicated an adenocarcinoma of the remnant pancreas. A remnant distal pancreatectomy with a splenectomy was performed. The histopathological findings for the second neoplasm were similar to those of the initial lesion (Figure 2c).
Figure 2. Case#1: second operation. a. A tumor approximately 3 cm
in diameter was detected in the pancreatic tail on abdominal CT. b. A
hot spot in FDG-PET corresponded to the tumor site on CT. c. A
well- or moderately-differentiated tubular adenocarcinoma similar to
the initial pancreatic cancer was detected. Mild atypical cells with a
slightly swollen nucleus formed an irregular ductal structure and
invaded the parenchyma. (H&E stain, x100).
Carcinoma cells had invaded vessels, lymph ducts and neurons, and there were lymph node metastases (T3N1M0; R0; pathological stage: IIB). The patient was alive at 10 months after the second operation without any recurrence.
Case#2
A 67-year-old man showed a pancreatic tumor on abdominal US at an annual medical checkup. An abdominal CT scan detected a 1 cm tumor in the body of the pancreas and main pancreatic duct dilatation of the distal pancreas (Figure 3a). A distal pancreatectomy with splenectomy was performed in February 2006.
Figure 3. Case#2: initial operation. a. A tumor approximately 1 cm
in diameter and main pancreatic duct dilatation of the distal pancreas
was detected in the pancreatic body on abdominal CT. b. Adenocarcinoma of the pancreas. Atypical cells with a swollen
nucleus formed a papillary projection. c. Mild atypical epithelia
projected from the cut edge of the main pancreatic duct. (H&E stain,
x100).
Histopathological examination confirmed a welldifferentiated adenocarcinoma with no vessel or lymph duct invasion and no lymph node metastasis (Figure 3b). Mild atypical epithelia were observed at the cut edge of the main pancreatic duct (T1N0M0; R0; pathological stage: IA) (Figure 3c). Periodic checkups without adjuvant chemotherapy were carried out for 2 years, and there were no abnormal findings in abdominal CT scans or tumor marker assays.
In March 2008 (28 months after the initial operation), the CA 19-9 level increased to 44 U/mL (reference range: 0-36 U/mL). An abdominal CT scan revealed a low density lesion at the cut end of the pancreas (Figure 4a), and this region appeared as a hot spot on FDG-PET (Figure 4b). A remnant proximal pancreatectomy with duodenectomy was performed in August 2008. Histopathological examination of the second neoplasm confirmed a moderately- to poorlydifferentiated adenocarcinoma which were different than the findings in the initial neoplasm (Figure 4c). The second findings led to a diagnosis of a metachronous pancreatic carcinoma with vessel, lymph duct and neuron invasion accompanied by lymph node metastases (T3N1M0; R0; pathological stage: IIB). The patient showed multiple liver metastases 8 months after the second operation.
Figure 4. Case#2: second operation. a. Abdominal CT revealed a
low-density lesion at the cut end of the pancreatic head. b. FDG-PET
showed a hot spot at the same pancreas head location as the tumor
appeared on CT. c. Moderately differentiated tubular
adenocarcinoma. The cancer cells invaded as a tubular and/or
papillary structure. (H&E stain, x100).
DISCUSSION
Invasive ductal carcinoma of the pancreas is one of the most intractable carcinomas. Although various treatments, such as chemotherapy and/or radiation, have been developed, surgical resection provides the only chance of cure and long-term survival. According to the Pancreatic Cancer Registry Report 2007 of the Japan Pancreas Society (JPS), the 5-year survival rate for invasive ductal carcinoma of the pancreas is 6.9- 11.6% in all cases and 11.2-20% in cases which undergo surgical resection [6, 7]. Recurrences are found within 2 years in more than half of surgical resection cases [8, 9, 10]. The most common forms of recurrence are local recurrence, liver metastases and peritoneal disseminations [11, 12], and these are generally beyond surgical resection or indications for chemotherapy and/or radiation therapy. Few recurrent or metachronous pancreatic carcinomas are resectable. In the present paper, we describe two patients who underwent a repeat pancreatectomy for pancreatic carcinoma. The pathogenesis of secondary carcinoma, whether recurrent or metachronous de novo, is usually hard to determine. In Case#1, the secondary carcinoma was diagnosed as being an ectopic recurrence, due to its histopathological similarity to the primary carcinoma, although the presence of a pancreatic intraepithelial neoplasia suggested a metachronous de novo carcinoma. In Case#2, the relatively slow growth of the secondary carcinoma suggested that it arose via multicentric de novo carcinogenesis.
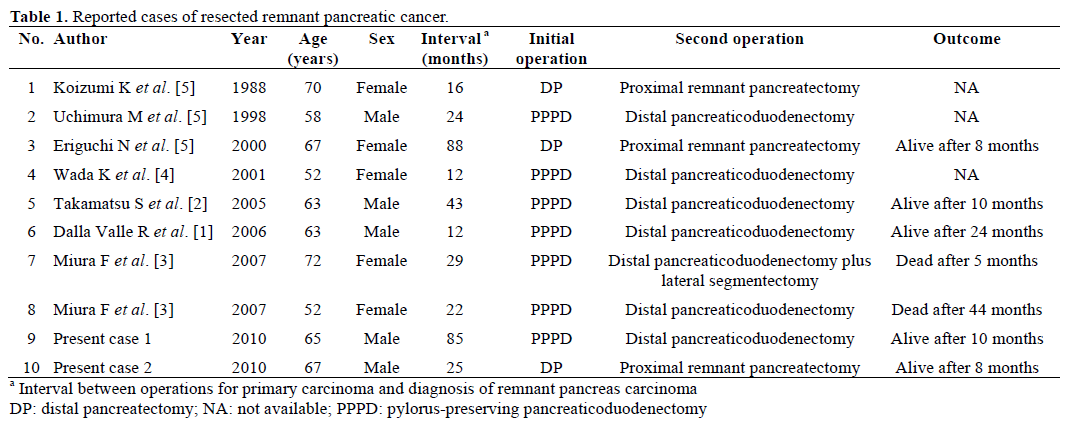
Although there has been an increase in the number of reports of remnant pancreatectomy for IPMNs, common bile duct carcinoma or carcinoma of papilla of Vater, we found very few reports of remnant pancreatectomy for recurrent or metachronous pancreatic carcinoma [1, 2, 3, 4, 5]. Ten cases, including the present cases, have been reported in the literature (Table 1) [1, 2, 3, 4, 5]. These cases include five male and five female patients, with an average patient age of 62.9 years (range: 52-72 years). The average time interval between the initial primary carcinoma operation and the diagnosis of a remnant pancreatic carcinoma was 35.6 months (range: 12-88 months). All cases underwent a remnant pancreatectomy, with one case also undergoing a lateral segmentectomy of the liver. The average survival time after the second operation was 15.6 months (range:, 4- 44 months). Five patients were alive at the time of writing, and one patient has been alive for 44 months after surgery.
In the present cases, FDG-PET provided valuable information for the diagnosis of remnant pancreatic carcinoma. FDG-PET is useful for diagnosing pancreatic tumors [13, 14] and can also play a key role in the diagnosis of remnant pancreatic carcinoma. In Case#1, FDG-PET was carried out after an abdominal CT indicated a tumor lesion in the remnant pancreas. In Case#2, FDG-PET was carried out when CA 19-9 levels increased without obvious tumor detection on abdominal CT. These cases indicate that FDG-PET can be a key modality in the differential diagnosis of remnant pancreatic lesions. Considering the high cost of FDG-PET, it should be performed after other, less costly modalities.
Recent progress in chemotherapy has improved outcomes in pancreatic carcinoma patients. Randomized control trials, such as the Charité Onkologie (CONKO-001) [15] and the European Study Group for Pancreatic Cancer (ESPAC-1) [16], have demonstrated that adjuvant chemotherapy improved overall survival and disease free survival after pancreatic resection. Improved pancreatic carcinoma outcomes provide more opportunity for remnant pancreatectomies and the possibility of cure in selected cases.
In summary, remnant pancreatectomy should be considered as a treatment option for recurrent or metachronous pancreatic carcinoma. An appropriate follow-up and preoperative assessment including FDGPET is essential for selecting the cases which could be candidates for a remnant pancreatectomy.
Conflict of interest
The authors have no potential conflicts of interest
Grants and financial support
None
References
- Dalla Valle R, Mancini C, Crafa P, Passalacqua R. Pancreatic carcinoma recurrence in the remnant pancreas after a pancreaticoduodenectomy. JOP. J Pancreas (Online) 2006; 7:473-7. [PMID 16998244]
- Takamatsu S, Ban D, Irie T, Noguchi N, Kudoh A, Nakamura N, et al. Resection of a cancer developing in the remnant pancreas after a pancreaticoduodenectomy for pancreas head cancer. J GastrointestSurg 2005; 9:263-9. [PMID 15694823]
- Miura F, Takada T, Amano H, Yoshida M, Isaka T, Toyota N, et al. Repeated pancreatectomy after pancreatoduodenectomy. J GastrointestSurg 2007; 11:179-86. [PMID 17390170]
- Wada K, Takada T, Yasuda H, Amano H, Yoshida M. A repeated pancreatectomy in the remnant pancreas 22 months after pylorus-preserving pancreatoduodenectomy for pancreatic adenocarcinoma. J HepatobiliaryPancreatSurg 2001; 8:174-8. [PMID 11455476]
- Eriguchi N, Aoyagi S, Imayama H, Okuda K, Hara M, Fukuda S, et al. Resectable carcinoma of the pancreatic head developing 7 years and 4 months after distal pancreatectomy for carcinoma of the pancreatic tail. J HepatobiliaryPancreatSurg 2000; 7:316-20. [PMID 10982633]
- Japan Pancreas Society. Pancreatic Cancer Registry Report 2007. Suizo 2007; 22:e1-425. [ISSN 1881-2805]
- Yeo CJ, Cameron JL, Lillemoe KD, Sitzmann JV, Hruban RH, Goodman SN, et al. Pancreaticoduodenectomy for cancer of the head of the pancreas. 201 patients. Ann Surg 1995; 221:721-31. [PMID 7794076]
- Ishikawa O, Wada H, Ohigashi H, Doki Y, Yokoyama S, Noura S, et al. Postoperative cytology for drained fluid from the pancreatic bed after "curative" resection of pancreatic cancers: Does it predict both the patient's prognosis and the site of cancer recurrence? Ann Surg 2003; 238:103-10. [PMID 12832972]
- Sperti C, Pasquali C, Piccoli A, Pedrazzoli S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg 1997; 21:195-200. [PMID 8995078]
- Kayahara M, Nagakawa T, Ueno K, Ohta T, Takeda T, Miyazaki I. An evaluation of radical resection for pancreatic cancer based on the mode of recurrence as determined by autopsy and diagnostic imaging. Cancer 1993; 72:2118-23. [PMID 8104092]
- Westerdahl J, Andren-Sandberg A, Ihse I. Recurrence of exocrine pancreatic cancer-Local or hepatic? Hepatogastroenterology 1993; 40:384-7. [PMID 8406311]
- Griffin JF, Smalley SR, Jewell W, Paradelo JC, Reymond RD, Hassanein RE, Evans RG. Patterns of failure after curative resection of pancreatic carcinoma. Cancer 1990; 66:56-61. [PMID 2354408]
- Koyama K, Okamura T, Kawabe J, Nakata B, Chung KH, Ochi H, et al. Diagnostic usefulness of FDG PET for pancreatic mass lesions. Ann Nucl Med 2001; 15:217-24. [PMID 11545191]
- Rose DM, Delbeke D, Beauchamp RD, Chapman WC, Sandler MP, Sharp KW, et al. 18Fluorodeoxyglucose-positron emission tomography in the management of patients with suspected pancreatic cancer. Ann Surg 1999; 229:729-37. [PMID 10235532]
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs. observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA 2007; 297:267-77. [PMID 17227978]
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 2004; 350:1200-10. [PMID 15028824]





