Keywords
Arthritis, Rheumatoid; Diarrhea; Flushing; Neuroendocrine Tumors; Pancreatic Neoplasms
INTRODUCTION
Sandostatin® LAR® depot is a synthetic analogue of the naturally occurring hormone somatostatin. Sandostatin® LAR® depot is indicated for long-term maintenance therapy in acromegalic patients for whom medical treatment is appropriate and who have been shown to respond to and can tolerate immediate release Sandostatin® (octreotide acetate) injection, or those patients who have had an inadequate response to surgery or in those for whom surgical resection is not an option, or in patients who have received radiation and have had an inadequate therapeutic response [1]. Sandostatin® LAR® depot is also indicated for longterm treatment of the severe diarrhea and flushing episodes associated with metastatic carcinoid tumors (neuroendocrine) and for the long-term treatment of the profuse watery diarrhea associated with VIP-secreting tumors in patients in whom initial treatment with immediate release Sandostatin® injection has been shown to be effective and tolerated [2].
Most recently, a randomized clinical trial has showed that Sandostatin® LAR® depot significantly lengthens time to tumor progression compared with placebo in patients with functionally active and inactive metastatic midgut neuroendocrine tumors [3].
The most frequently reported drug-related adverse events were biliary disorders (62%), gastrointestinal disorders (14% to 38%), and injection-site pain (20% to 50%). Hypoglycemia (4%), hyperglycemia (27%), sinus bradycardia (19%), conduction abnormalities (9%), and arrhythmias (3%) have been reported. The medical literature does not describe rheumatoid arthritis or similar toxicities associated with Sandostatin® LAR® depot. We would like to present a case of a Caucasian female who developed rheumatoid arthritis like complaints after chronic treatment with Sandostatin® LAR® depot [4].
CASE REPORT
Our patient is a 53-year-old female with a history of neuroendocrine tumor of the pancreas with metastasis to the liver, lung. An octreotide scan done at that time suggested tracer avid disease in the posterior mediastinum, liver, and the upper abdomen, foci of abnormal activity in the upper abdomen that corresponded to bilateral adrenal glands. Her symptoms included facial flushing (4-5 times/week), and diarrhea (3-4 per day). She was initially given subcutaneous Sandostatin® followed by Sandostatin® LAR® depot 20 mg i.m. with some relief facial flushing (2 times/week), and diarrhea (1-2 per day). We escalated the dose to 30 mg i.m. after two initial doses of 20 mg i.m. that improved to symptoms dramatically: facial flushing (none), and diarrhea (occasional). She then remained on Sandostatin® LAR® depot 30 mg intramuscularly in June 2006. Her CT scan was performed every three months showed stable disease and serum serotonin and chromogranin-A remained within normal limits.
She presented for her 45th cycle of Sandostatin® LAR® depot at 30 mg and complained of joint pains in the hands as well as feet (more pronounced on the hands) that she noticed over the last 2 months. Her morning stiffness in and around joints lasted 1-2 hours. Her joint pain was associated intermittent swelling in the morning that resolved spontaneously with time. She denied any redness with it. Physical examination was normal with no clubbing, cyanosis or edema or rash. The pain was indicated to involve the proximal interphalangeal, metacarpophalangeal, wrist joints and ankles.
Laboratory data showed: white blood cell count 9.4 x1,000/μL (reference range: 4.0-10.0 x1,000/μL), hemoglobin 12.7 g/dL (reference range: 12.0-16.0 g/dL), hematocrit 38.0% (reference range: 37.0- 47.0%), platelet count 256 x1,000/μL (reference range: 150-350 x1,000/μL), glucose 334 mg/dL (reference range: 70-100 mg/dL), creatinine 0.8 mg/dL (reference range: 0.5-1.2 mg/dL), albumin 4.4 g/dL (reference range: 3.5-5.0 g/dL), and normal liver function tests.
CT of the chest, abdomen and pelvis showed no pulmonary masses, no pleural or pericardial effusions, a stable 1.5x1.1 cm para-aortic posterior mediastinal mass, unchanged compared to most recent examination, multiple pancreatic cystic lesions associated with pancreatic body and tail which appear stable; the largest lesion measures 8.4x8.0 cm, unchanged. Multiple hepatic metastases were again seen and appeared grossly stable in size and configuration. A previously described right hepatic lobe index lesion measuring 1.8x2.4 cm was stable. There were stable bilateral adrenal nodules. The spleen, gallbladder, and kidneys were unremarkable. There was no ascites or bowel obstruction. There were no pelvic masses. There was no free air or free fluid. There was no acute or aggressive osseous pathology.
Therefore, she was referred to a rheumatologist. All the work-up, including rheumatoid factor (1:21; reference range: less than 1:20), anti nuclear antibody and cryoglobulins, was within normal limits. Her erythrocyte sedimentation rate was elevated: 51 millimeters per hour (reference range in females is 0- 20 millimeters per hour). Symptomatic joints (wrist and hand joints) were imaged and no abnormalities were noticed.
Therefore, we decided to reduce the dose of Sandostatin® LAR® depot to 20 mg i.m. and patient noticed 50% improvement in her pain and noticed minimal swelling. Since her carcinoid symptoms were in control and the reduced dose improved her rheumatologic complaints also, we kept her at the same dose. She remained on the present dose for the last five months and no exacerbation of her pain has been noticed. The development of her joint symptoms after chronic use of Sandostatin® LAR® depot and then improvement after reducing the dose suggests that her rheumatoid-like symptoms are possibly related to Sandostatin® LAR® depot.
To further assess this association, we used the Naranjo algorithm, Naranjo scale, or Naranjo nomogram, which is a questionnaire designed by for determining the likelihood of whether an adverse drug reaction is actually due to the drug rather than the result of other factors [5] (Table 1). Probability of adverse drug reaction is assigned via a score termed definite (total score greater than 9), probable (total score ranging 5- 8), possible (total score ranging 1-4) or doubtful (total score equal to 0) (Naranjo nomogram).
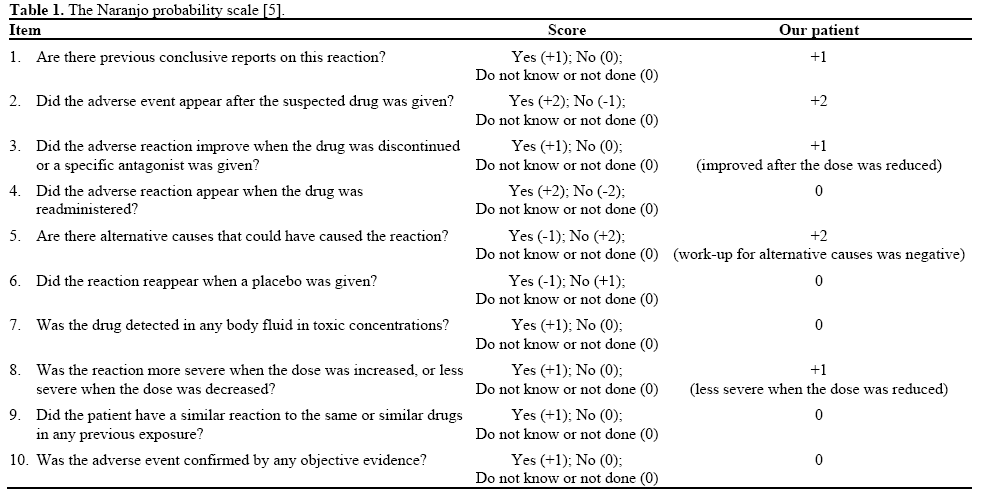
Our patient’s total score was 7. Based on the Naranjo nomogram our patient had probable adverse drug reaction.
DISCUSSION
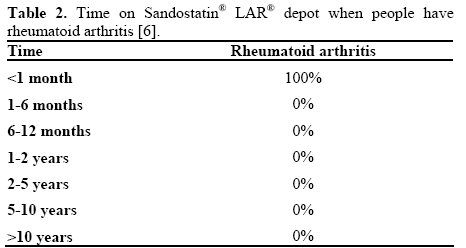
We reviewed the medical literature and did not find any relevant literature. Web review showed that such an association between rheumatoid arthritis and Sandostatin® LAR® depot has been reported rarely [6]. We reviewed a study of 12 people who have rheumatoid arthritis while taking Sandostatin® LAR® depot based on reports from FDA and community. Based on this study, 3,557 people reported to have side effects when taking Sandostatin® LAR® depot [6]. Among them, 12 people (0.34%) have rheumatoid arthritis. Among the patients who developed rheumatoid arthritis, 46.7% were female and 53.3% were male. Time on Sandostatin® LAR® depot when people have rheumatoid arthritis is shown in Table 2. Age of people who have rheumatoid arthritis when taking Sandostatin LAR® depot is shown in Table 3.

Rheumatoid arthritis is a chronic systemic disease affecting approximately 0.5-1% of the adult population with an estimated annual incidence of 12.0-24.5 males and 23.9-54.0 females per 100,000. Rheumatoid arthritis occurs two to three times more often in women than in men [7]. The incidence is largely consistent racially and geographically, and the peak age of onset lies between the ages of 45 and 65 years [8].
The etiology of rheumatoid arthritis is not known and thought to be multifactorial. There is a certain genetic susceptibility. As many as 70% of patients with rheumatoid arthritis express human leukocyte antigen DR4 [9]. Environmental factors (smoking) or infectious agents are suggested to play a role in the etiology, but their contribution has yet to be defined [10].
The diagnosis of rheumatoid arthritis requires a spectrum of disease manifestations as defined by the American College of Rheumatology [11]. The American College of Rheumatology identified seven diagnostic criteria for rheumatoid arthritis. Four of the following seven criteria must be met:
1. Morning stiffness in and around joints lasting 1 hour or more before maximal improvement (must have been present for at least 6 weeks);
2. Soft tissue swelling (arthritis) of three or more joint areas (must have been present for at least 6 weeks);
3. Swelling (arthritis) of the proximal interphalangeal, metacarpophalangeal, or wrist joints (must have been present for at least 6 weeks);
4. Symmetrical arthritis (must have been present for at least 6 weeks);
5. Subcutaneous nodules;
6. Positive test for rheumatoid factor;
7. Radiographic erosions and/or periarticular osteopenia in hand and/or wrist joints.
Our patient fulfilled the criteria by having the first four signs and symptoms as required by the American College of Rheumatology for the diagnosis of rheumatoid arthritis. Although our patient was seronegative, akin to many other patients with rheumatoid arthritis. Literature also suggests that approximately 80% seronegative seroconvert and become positive later. Disease severity is often worse in those who are seropositive. “Improvement after reducing the dose suggests relation to the drug intake”; that is true, but we cannot formally exclude the possibility of an “idiopathic” rheumatoid arthritis, or a paraneoplastic polyarthritis, which is also seronegative and non-erosive [12]. Analysis of data from FDA showed a prevalence of 0.34% of rheumatoid arthritis in patients under Sandostatin®, which is comparable to recent reports on rheumatoid arthritis prevalence in general American population, and no new rheumatoid arthritis case has been declared during therapy, that means that our report is the first to discuss the triggering of a rheumatoid arthritis after Sandostatin® initiation.
The association of the rheumatoid arthritis with Sandostatin® LAR® depot seems to be a rare complication. Because of its widespread distribution within the nervous system and gastroenteropancreatic system, and its diverse physiological inhibitory actions on various gastrointestinal functions, this association may be speculated.
The use of Sandostatin® has extended beyond acromegaly and carcinoid to acute esophageal variceal bleeding, pancreatic pseudocysts, gastrointestinal, and pancreatic external fistulae, short bowel syndrome, a dumping syndrome and acquired immunodeficiency syndrome-related refractory hypersecretory diarrhea. We encourage other investigators to publish such reports and further research is warranted to understand this association.
Conflict of interest
The author has no potential conflict of interest
References
- Yang LP, Keating GM. Octreotide long-acting release (LAR): areview of its use in the management of acromegaly. Drugs 2010;70:1745-69.
- Modlin IM, Pavel M, Kidd M, Gustafsson BI. Review article:somatostatin analogues in the treatment of gastroenteropancreatic neuroendocrine (carcinoid) tumours. Aliment Pharmacol Ther 2010;31:169-88.
- Rinke A, Müller HH, Schade-Brittinger C, Klose KJ, Barth P, Wied M, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 2009;27:4656-63.
- Novartis Oncology. Sandostatin LAR. https://www.sandostatin.com/ (Last accessed on 12/11/10).
- Naranjo CA, Busto U, Sellers EM, et al. A method forestimating the probability of adverse drug reactions. Clin Pharmacol Ther 1981; 30 : 239-45.
- eHealthMe. Sandostatinlar side effect: Rheumatoid arthritis. https://www.ehealthme.com/ds/sandostatin+lar/rheumatoid+arthritis (Last accessed on 12/11/10).
- GabrielSE. The epidemiology of rheumatoid arthritis. Rheum Dis Clin North Am 2001; 27:269-82.
- DugowsonCE, Koepsell TD, Voigt LF, Bley L, Nelson JL, Daling JR. Rheumatoid arthritis in women: incidence rates in group health cooperative, Seattle, Washington, 1987-1989. Arthritis Rheum1991; 34:1502-7.
- DeightonCM, Cavanagh G, Rigby AS, Lloyd HL, Walker DJ. Both inherited HLA-haplotypes are important in the predisposition to rheumatoid arthritis. Br J Rheumatol 1993; 32:893-8.
- HeliovaaraM, Aho K, Aromaa A, Knekt P, Reunanen A. Smoking and risk of rheumatoid arthritis. J Rheumatol 1993;20:1830-5.
- ArnettFC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988; 31:315-24.
- Morel J, Deschamps V, Toussirot E, Pertuiset E, Sordet C,Kieffer P, et al. Characteristics and survival of 26 patients with paraneoplastic arthritis. Ann Rheum Dis 2008; 67:244-7.

