Keywords
Carcinoma; Heparin; Neoplasms; Pancreas; Pancreatic Neoplasms; Thromboembolism; Thrombophilia; Thrombosis; Venous Insufficiency; Warfarin
Abbreviations
KRAS: v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog; VTE: venous thromboembolism; TP53: tumor protein p53
INTRODUCTION
Cancer and its treatments are well-recognized risk factors for venous thromboembolism (VTE). Although the incidence of VTE in cancer patients is not well documented, there is evidence that the absolute risk depends on the tumor type, the stage or extent of the cancer, and treatment with antineoplastic agents. The most common cancer types seen in patients with thrombosis are breast, colorectal and lung, reflecting the prevalence of these malignancies in the general population. When the underlying prevalence is taken into account, cancers of the pancreas, ovary and brain are the most strongly associated with thrombotic complications. Although idiopathic thrombosis can be the first manifestation of an occult malignancy, extensive screening for cancer in these patients has not been shown to improve survival and is not warranted. Despite treatment, cancer patients with thrombosis have a poor prognosis. This is likely due to premature deaths from recurrent VTE and to the aggressive nature of the underlying cancer. Further research is needed to address the many clinical questions in the management of thrombosis in patients with cancer.
History of Association between Pancreatic Cancer and VTE
French internist Trousseau suggested the relationship between thrombosis and gastrointestinal cancer [1]. It is believed that he himself developed thrombosis and died of a gastrointestinal cancer [2, 3] and Trousseau's syndrome has been studied extensively to determine whether thrombophlebitis really predicts the presence of a visceral tumor.
Sproul was the first who demonstrated the association between thromboembolism and pancreatic cancer in 1938 [4]. Since then it has become dogma that thromboembolism is associated with pancreatic carcinoma, despite the existence of several studies that have indicated that the relationship is neither unique to pa ncreatic carcinoma nor especially common in patients with this disease [5].
Virchow made important contribution in nineteenth century when he described the consequences of embolism in the pulmonary vasculature [6, 7]. Virchow's triad consists of stasis, vascular injury and hypercoagulability which later used to explain how venous thrombosis develops. These same factors seem to be involved in cancer tissue and cause the formation of local thrombi. As the tumor-specific causes of hypercoagulability have been reviewed already [4], we discuss here the main factors, and how to manage it.
How Common is Hypercoagulability in Pancreatic Cancer
Hypercoagulability in cancer is very common. Ovarian cancer is the most common cause of thrombotic event [8]. Hypercoagulability is more common in patient of pancreatic cancer than any other type of gastrointestinal tumors. It has been reported that incidences of disease range from 17% to 57% [9]. The chances of recurrence are high in pancreatic cancer than any other type. One study found that 13.6% of patients with pancreatic carcinoma experienced a thromboembolic event during therapy [10]. However, tumors such as bladder, esophagus and breast cancers are less likely than pancreatic carcinoma to be associated with thromboembolic events [11].
Why is Hypercoagulation Common in Pancreatic Cancer?
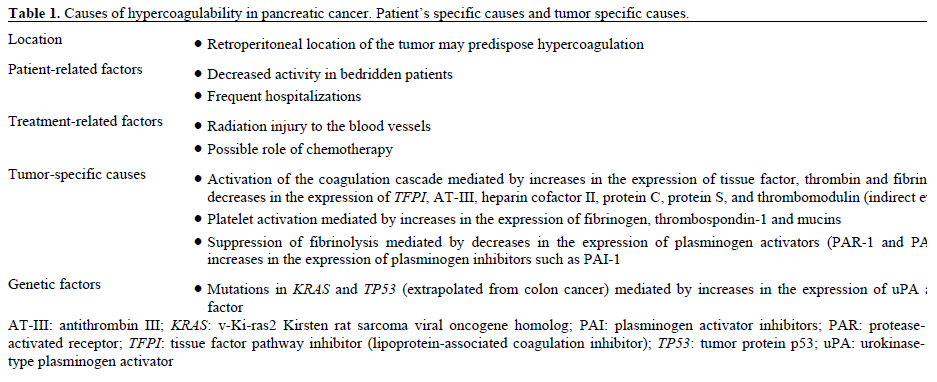
Location
It is common because the tumor is retroperitoneal in location, decrease activity in bedridden patients, patient’s frequent hospitalization and radiation injury to the vessels.
Increased Pro-Thrombotic Factors
In pancreatic cancer, tissue factor [12, 13], thrombin [14, 15] and fibrinogen [16] level are increased. Higher concentration of tissue factor in tumor tissue has been shown to be associated with the development of thromboembolic events [13]. Plasma levels of thrombin have also been found to be elevated in patients with pancreatic carcinoma [12]
Decreased Inhibitors of Anticoagulation
The inhibitors of anticoagulation is decreased with pancreatic carcinoma add another ingredient in the hypercoagulation. These factors include antithrombin III, heparin cofactor II, protein C, free protein S, and thrombomodulin [17, 18, 19].
Increased Platelet Aggregation
Increased platelet aggregation results from increased expression of fibrinogen and thrombospondin-1, as well as from the production of mucins by the tumor [20, 21, 22, 23]. Mucins interact with platelets and generate platelet-rich microthrombi without the involvement of thrombin. These platelet-rich aggregates are then more likely to cause microangiopathic disease [23]. A decrease in expression of plasminogen activator [24] and an increase in circulation levels of plasminogen activator inhibitor have been reported [25] (Figure 1).
Figure 1. Scheme of the coagulation cascade.
TF: tissue factor; TFPI: tissue factor pathway inhibitor; VIIa,
activated factor VII; X: factor X; Xa: activated factor X
Role of Inflammation
Transforming growth factor is upregulated in pancreatic carcinoma cell lines [26] and induces plasminogen activator inhibitor-1 (PAI-1), which has a procoagulatory effect [27]. Another inflammatory cytokine that is upregulated in patients with several types of cancer, tumor necrosis factor (TNF) [28] has also been shown to induce the expression of tissue factor and to downregulate the expression of the inhibitor of coagulation thrombomodulin in endothelial cells [29]. Currently, no data exists to show the direct effect of TNF expression on coagulation in patients with pancreatic carcinoma. However, inflammatory cells recruited to the tumor site do contribute to angiogenesis in patients with pancreatic carcinoma. This can be explained by the fact that proangiogenic growth factors such as VEGF are expressed by mast cells and macrophages [30].
Is There a Genetic Component Responsible for Hypercoagulation in Pancreatic Cancer Patients?
Activation of the v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS), which is associated in the70% of the cases of loss-of-function mutations in the tumor protein p53 (TP53) gene, which encodes the tumor suppressor P53 [31, 32]. Furthermore, both KRAS activation and loss-of-function for TP53 have been shown to have a cumulative effect on the expression of tissue factor in tumor cells and on circulating levels of tissue factor in mice with colon cancer [31] (Table 1).
Can Thromboembolism Predict the Presence of Pancreatic Carcinoma?
Sometime thrombotic event could be the first presentation of cancers. It has been reported that 3.3- 5.0% of patients with cancer present with a thrombotic event [33, 34].
There is 5.0-7.6% chance that the patients who present with thromboembolism develop cancer on follow-up [34]. There is, therefore, an odds ratio of 7.9 (95% CI: 3.14-20.09, P<0.01) for the presence of an occult cancer in patients who present with venous thromboembolic disease [35]. The standardized incidence ratio for the development of cancer within 1 year of venous thromboembolism was 1.3 (95% CI: 1.2-1.5), and the risk of pancreatic carcinoma was 2.6 (95% CI: 1.8-3.6), which was higher than for renal, stomach or lung cancer, but lower than for ovarian cancer [8]. The meta-analysis shows that the relative risk for the development of pancreatic carcinoma after an initial thromboembolic event was calculated to be 6.1 (95% CI: 3.8-9.7), compared with those who did not experience a thromboembolic event. The proportional incidence ratio was also 6.3 (95% CI: 3.8- 10.6) [11]. Patients who have thromboembolic event have a six-fold higher chance of developing pancreatic cancer than the general population. This suggests that a thromboembolic event is associated with an increased risk for the development of pancreatic cancer.
Is There a Role of Embolic Tumor in Tumor Progression?
Recent studies evidenced that malignant growth has also been linked to activity of heparin-like glycosoaminoglycans, to neoangiogenesis, to protease activity, to immune function and gene expression in addition with activation of coagulation and fibrinolysis [36]. Emboli from the tumor can cause stroke and pulmonary embolism. Pancreatic tumors are the common cause of deep venous thrombosis. But there is not much data available on the embolism of pancreatic tumor.
Does Thromboembolism or Recurrent Thromboembolism Predict Poor Outcome?
There seems to be a relationship between thromboembolic events and poor prognosis [37]. Patients who have a thromboembolic event are more likely to have advanced cancer diagnosed within 4-12 months [8]. A retrospective analysis of patients with pancreatic carcinoma who received different chemotherapy regimens (all of which included gemcitabine) shows that a synchronous thromboembolism was detected in 19.3% of patients associated with a higher probability of not responding to therapy(odds ratio 2.98; 95% CI: 1.42-6.27; P=0.004), but did not predict a shorter survival [10]. So it seems reasonable to say that the development of thromboembolic disease around the time of diagnosis might predict poor prognosis in patients with pancreatic carcinoma
Is There Any Potential Role of Anticoagulation in Pancreatic Cancer?
Warfarin
Warfarin, a vitamin K inhibitor, interferes with carboxylation of the hepatic coagulation factors II, VII, IX and X, which decreases their activity [38]. In a randomized, prospective study, patients were treated with warfarin for either 3 or 12 months after a first episode of thromboembolic disease. There was no significant difference in the number of newly diagnosed cancer cases between the groups after 5 years of follow-up. This finding suggests that there is no benefit of extending anticoagulation treatment from 3 to 12 months, but it does not resolve whether any anticoagulation with warfarin has a beneficial effect [39]. Only two studies have examined the use of warfarin in patients with pancreatic carcinoma - one retrospective and one prospective (Table 2). In the retrospective study [40], mean survival was increased from 2.3 to 5.0 months (addition of 2.7 months; i.e., extended from 2.3 to 5 months) upon addition of warfarin to chemotherapy in an unselected group of 280 patients receiving different combinations of chemotherapy plus warfarin. In a subgroup of patients receiving the same chemotherapy regimen, the increase in median survival was smaller (2 months; i.e., extended from 5.1 to 7.1 months), but the improvement was still significant (P=0.05). In this stu dy, patients were hospitalized every 2 weeks and all received low molecular weight heparin during their hospital stay at prophylactic doses. As low molecular weight heparin was administered to all patients irrespective of the use of warfarin, the increase in survival could be attributed to warfarin use. There was no significant increase in bleeding complications as a result of warfarin use. As the dose of warfarin was set at 2.5 mg without attempting to achieve a therapeutic prothrombin time, no laboratory monitoring was needed. Biases can result in over interpretation in retrospective analyses; therefore, Nakchbandi et al. [41] also examined prospectively whether administration of low-dose warfarin increased surviva l. The administration of low-dose warfarin resulted in a median survival of 6.8 months that compared favorably with historical controls not treated with warfarin, in whom median survival was 3.6 months, confirming the findings of the retrospective analysis.

Heparin
Heparin binds to the enzyme inhibitor antithrombin (AT) causing a conformational change those results in its activation through an increase in the flexibility of its reactive site loop. Because of its short biologic half life of approximately one hour, heparin must be given frequently or as a continuous infusion. However, the use of low molecular weight heparin (LMWH) has allowed once daily dosing, thus not requiring a continuous infusion of the drug. Two studies have examined whether low molecular weight heparin confers any advantage over no anticoagulation in patients with pancreatic carcinoma. Icli et al. [42] examined whether adding low molecular weight heparin to gemcitabine plus cisplatinum offered a survival benefit over the use of chemotherapeutic agents alone in a nonrandomized setting. They found a significant improvement in survival in the low molecular weight heparin group versus the control group (13.0 versus 5.5 months, P=0.0001). A retrospective analysis by von Delius et al. [43] revealed that the addition of low molecular weight heparin to chemotherapy prolonged survival by 2.8 months (i.e., extended from 3.8 to 6.6 months, P=0.006) in patients with metastatic disease, but not in those with localized disease. These data indicate that low molecular weight heparin might have a beneficial effect on the treatment of patients with pancreatic carcinoma; however, the results from two prospective, randomized, multicenter clinical trials of low molecular weight heparin plus chemotherapy have to be awaited. The first study was initiated in Germany (PROSPECT trial) [44] and the second in the UK (FRAGEM trial) [45]. The results of these studies will hopefully help to clarify whether treatment with low molecular weight heparin offers a survival advantage to patients with pancreatic carcinoma (Table 3).
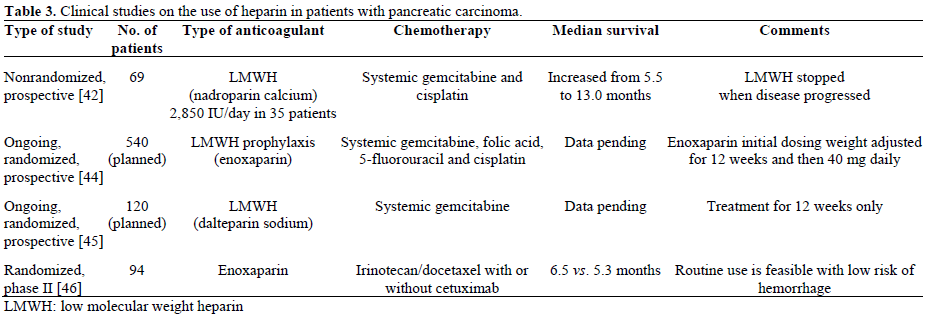
The Eastern Cooperative Oncology Group (ECOG 8200) conducted a randomized phase II trial of irinotecan/docetaxel with or without cetuximab in metastatic pancreatic cancer. Patients not receiving therapeutic anticoagulation received enoxaparin 40 mg/day. The results showed that the routine use of prophylactic low molecular weight heparin is feasible in patients with advanced pancreatic cancer, with a low risk of hemorrhage on study [46]. Progression free survival was 3.9 months in patients with baseline thrombosis versus 4.2 months in patients with no thrombosis.
How to Move Forward
Much work needs to be done in the future for cancer associated thrombosis. Although new studies and work is going on, it is unlikely that risk for cancer associated thrombosis will decline. Agents that target VEGF and other antiangiogenic therapies have been associated with high incidence of thromboembolic disease. The thrombogenicity of widely used non-cancer drugs, such as inhibitors of cyclo-oxygenase 2, is increasingly being recognized. Newer agents might change antithrombotic therapy. For example, there has been interest in the oral, direct inhibitor of thrombin ximelagatran, the first new oral anticoagulant since warfarin. Unlike warfarin, it exerts its anticoagulant effect almost immediately, and does not need frequent laboratory monitoring. It seems to be as effective as, or more effective than, heparins or warfarin in the treatment and prevention of thromboembolism, and might eventually replace warfarin [46, 47]. Clinical testing of this agent in patients with cancer is awaited.
Conflict of interest
The authors have no potential conflicts of interest
References
- Trousseau A. Phlegmasia alba dolens. Clinique Medicale de l'Hotel-Dieu 1865; 3:654-712.
- Bariety M. Trousseau, 1801-67. Geneva:Mazenod; 1947:234- 235.
- Khorana AA, Fine RL. Pancreatic cancer and thromboembolic disease. Lancet Oncol 2004; 5:655-63. [PMID 15522652]
- Sproul E. Carcinoma and venous thrombosis: the frequency of association of carcinoma in the body or tail of the pancreas with multiple venous thrombosis. Am J Cancer 1938; 34:566.
- Pinzon R, Drewinko B, Trujillo JM, Guinee V, Giacco G. Pancreatic carcinoma and Trousseau's syndrome: experience at a large cancer center. J Clin Oncol 1986; 4:509-14. [PMID 3958764]
- Virchow RLK. Thrombosis and Emboli 1856; 1846-56. In: Gesammelte Abhandlungen zur Wissenschaftlichen Medicin Frankfurt, Meidinger:Sohn & Co Reprint edition:Virchow R 1998; (AC Matzdorff, WR Bell transl Canton, MA:Science History Publications).
- Brotman DJ, Deitcher SR, Lip GY, Matzdorff AC. Virchow's triad revisited. South Med J 2004; 97:213-4. [PMID 14982286]
- White RH, Chew HK, Zhou H, Parikh-Patel A, Harris D, Harvey D, Wun T. Incidence of venous thromboembolism in the year before the diagnosis of cancer in 528,693 adults. Arch Intern Med 2005; 165:1782-7. [PMID 16087828]
- Khorana AA, Fine RL. Pancreatic cancer and thromboembolic disease. Lancet Oncol 2004; 5:655-63. [PMID 15522652]
- Mandalà M, Reni M, Cascinu S, Barni S, Floriani I, Cereda S, et al. Venous thromboembolism predicts poor prognosis in irresectable pancreatic cancer patients. Ann Oncol 2007; 18:1660-5. [PMID 17660490]
- Iodice S, Gandini S, Löhr M, Lowenfels AB, Maisonneuve P. Venous thromboembolic events and organ-specific occult cancers: a review and meta-analysis. J Thromb Haemost 2008; 6:781-8. [PMID 18284604]
- Haas SL, Jesnowski R, Steiner M, Hummel F, Ringel J, Burstein C, et al. Expression of tissue factor in pancreatic adenocarcinoma is associated with activation of coagulation. World J Gastroenterol 2006; 12:4843-9. [PMID 16937466]
- Khorana AA, Ahrendt SA, Ryan CK, Francis CW, Hruban RH, Hu YC, et al. Tissue factor expression, angiogenesis, and thrombosis in pancreatic cancer. Clin Cancer Res 2007; 13:2870-5. [PMID 17504985]
- Wojtukiewicz MZ, Rucinska M, Zimnoch L, Jaromin J, Piotrowski Z, Rózanska-Kudelska M, et al. Expression of prothrombin fragment 1 + 2 in cancer tissue as an indicator of local activation of blood coagulation. Thromb Res 2000; 97:335-42. [PMID 10709909]
- Rudroff C, Seibold S, Kaufmann R, Zetina CC, Reise K, Schäfer U, et al. Expression of the thrombin receptor PAR-1 correlates with tumour cell differentiation of pancreatic adenocarcinoma in vitro. Clin Exp Metastasis 2002; 19:181-9. [PMID 11964083]
- Wojtukiewicz MZ, Rucinska M, Zacharski LR, Kozlowski L, Zimnoch L, Piotrowski Z, et al. Localization of blood coagulation factors in situ in pancreatic carcinoma. Thromb Haemost 2001; 86:1416-20. [PMID 11776308]
- Lindahl AK, Odegaard OR, Sandset PM, Harbitz TB. Coagulation inhibition and activation in pancreatic cancer. Changes during progress of disease. Cancer 1992; 70:2067-72. [PMID 1394036]
- Wojtukiewicz MZ, Sierko E, Zimnoch L, Kozlowski L, Kisiel W. Immunohistochemical localization of tissue factor pathway inhibitor-2 in human tumor tissue. Thromb Haemost 2003; 90:140-6. [PMID 12876637]
- Chaturvedi P, Singh AP, Moniaux N, Senapati S, Chakraborty S, Meza JL, Batra SK. MUC4 mucin potentiates pancreatic tumor cell proliferation, survival, and invasive properties and interferes with its interaction to extracellular matrix proteins. Mol Cancer Res 2007; 5:309-20. [PMID 17406026]
- Marguerie GA, Thomas-Maison N, Ginsberg MH, Plow EF. The platelet-fibrinogen interaction. Evidence for proximity of the A alpha chain of fibrinogen to platelet membrane glycoproteins IIb/III. Eur J Biochem 1984; 139:5-11. [PMID 6230229]
- Isenberg JS, Romeo MJ, Yu C, Yu CK, Nghiem K, Monsale J, et al. Thrombospondin-1 stimulates platelet aggregation by blocking the antithrombotic activity of nitric oxide/cGMP signaling. Blood 2008; 111:613-23. [PMID 17890448]
- Tobita K, Kijima H, Dowaki S, Oida Y, Kashiwagi H, Ishii M, et al. Thrombospondin-1 expression as a prognostic predictor of pancreatic ductal carcinoma. Int J Oncol 2002; 21:1189-95. [PMID 12429967]
- Wahrenbrock M, Borsig L, Le D, Varki N, Varki A. Selectinmucin interactions as a probable molecular explanation for the association of Trousseau syndrome with mucinous adenocarcinomas. J Clin Invest 2003; 112:853-62. [PMID 12975470]
- Kakkar AK, Chinswangwatanakul V, Tebbutt S, Lemoine NR, Williamson RC. A characterization of the coagulant and fibrinolytic profile of human pancreatic carcinoma cells. Haemostasis 1998; 28:1-6. [PMID 9885363]
- Andrén-Sandberg A, Lecander I, Martinsson G, Astedt B. Peaks in plasma plasminogen activator inhibitor-1 concentration may explain thrombotic events in cases of pancreatic carcinoma. Cancer 1992; 69:2884-7. [PMID 1591681]
- Löhr M, Schmidt C, Ringel J, Kluth M, Müller P, Nizze H, Jesnowski R. Transforming growth factor-beta1 induces desmoplasia in an experimental model of human pancreatic carcinoma. Cancer Res 2001; 61:550-5. [PMID 11212248]
- Albo D, Berger DH, Vogel J, Tuszynski GP. Thrombospondin-1 and transforming growth factor beta-1 upregulate plasminogen activator inhibitor type 1 in pancreatic cancer. J Gastrointest Surg 1999; 3:411-7. [PMID 10482694]
- Fareed D, Iqbal O, Tobu M, Hoppensteadt DA, Fareed J. Blood levels of nitric oxide, C-reactive protein, and tumor necrosis factoralpha are upregulated in patients with malignancy-associated hypercoagulable state: pathophysiologic implications. Clin Appl Thromb Hemost 2004; 10:357-64. [PMID 15497022]
- Scarpati EM, Sadler JE. Regulation of endothelial cell coagulant properties. Modulation of tissue factor, plasminogen activator inhibitors, and thrombomodulin by phorbol 12-myristate 13-acetate and tumor necrosis factor. J Biol Chem 1989; 264:20705-13. [PMID 2555368]
- Esposito I, Menicagli M, Funel N, Bergmann F, Boggi U, Mosca F, et al. Inflammatory cells contribute to the generation of an angiogenic phenotype in pancreatic ductal adenocarcinoma. J Clin Pathol 2004; 57:630-6. [PMID 15166270]
- Yu JL, May L, Lhotak V, Shahrzad S, Shirasawa S, Weitz JI, et al. Oncogenic events regulate tissue factor expression in colorectal cancer cells: implications for tumor progression and angiogenesis. Blood 2005; 105:1734-41. [PMID 15494427]
- Redston MS, Caldas C, Seymour AB, Hruban RH, da Costa L, Yeo CJ, Kern SE. p53 mutations in pancreatic carcinoma and evidence of common involvement of homocopolymer tracts in DNA microdeletions. Cancer Res 1994; 54:3025-33. [PMID 8187092]
- Monreal M, Lafoz E, Casals A, Inaraja L, Montserrat E, Callejas JM, Martorell A. Occult cancer in patients with deep venous thrombosis. A systematic approach. Cancer 1991; 67:541-5. [PMID 1985747]
- Prandoni P, Lensing AW, Bülller HR, Cogo A, Prins MH, Cattelan AM, et al. Deep-vein thrombosis and the incidence of subsequent symptomatic cancer. N Engl J Med 1992; 327:1128-33. [PMID 1528208]
- Monreal M, Fernandez-Llamazares J, Perandreu J, Urrutia A, Sahuquillo JC, Contel E. Occult cancer in patients with venous thromboembolism: which patients, which cancers. Thromb Haemost 1997; 78:1316-8. [PMID 9408011]
- Castellei R, Porro F. Cancer and thromboembolism: from biology to clinics. Minerva Med 2006; 97:175-89. [PMID 16760856]
- Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med 2006; 166:458-64. [PMID 16505267]
- Hirsh J, Fuster V, Ansell J, Halperin JL; American Heart Association; American College of Cardiology Foundation. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. Circulation 2003; 107:1692-711. [PMID 12668507]
- Taliani MR, Agnelli G, Prandoni P, Becattini C, Moia M, Bazzan M, et al. Incidence of cancer after a first episode of idiopathic venous thromboembolism treated with 3 months or 1 year of oral anticoagulation. J Thromb Haemost 2003; 1:1730-3. [PMID 12911585]
- Nakchbandi W, Mülller H, Singer MV, Löhr M, Nakchbandi IA. Effects of low-dose warfarin and regional chemotherapy on survival in patients with pancreatic carcinoma. Scand J Gastroenterol 2006; 41:1095-104. [PMID 16938724]
- Nakchbandi W, Müller H, Singer MV, Lohr JM, Nakchbandi IA. Prospective study on warfarin and regional chemotherapy in patients with pancreatic carcinoma. J Gastrointestin Liver Dis 2008; 17:285-90. [PMID 18836621]
- Icli F, Akbulut H, Utkan G, Yalcin B, Dincol D, Isikdogan A, et al. Low molecular weight heparin (LMWH) increases the efficacy of cisplatinum plus gemcitabine combination in advanced pancreatic cancer. J Surg Oncol 2007; 95:507-12. [PMID 17192920]
- von Delius S, Ayvaz M, Wagenpfeil S, Eckel F, Schmid RM, Lersch C. Effect of low-molecular-weight heparin on survival in patients with advanced pancreatic adenocarcinoma. Thromb Haemost 2007; 98:434-9. [PMID 17721628]
- Pelzer U, Hilbig A, Stieler J, Roll L, Stauch M, Opitz B, et al. A prospective, randomized trial of simultaneous pancreatic cancer treatment with enoxaparin and chemotherapy (PROSPECT - CONKO 004). J Clin Oncol (Meeting Abstracts) 2006; 24:4110.
- Maraveyas A. A phase II randomized study of chemoanticoagulation (gemcitabine-dalteparin) versus chemotherapy alone (gemcitabine) for locally advanced and metastatic pancreatic adenocarcinoma (FRAGEM). ClinicalTrials.gov. U.S. National Institutes of Health.
- Burtness BA, Powell ME, Berlin JD, Liles DK, Chapman AE, Mitchell EP, Benson AB. Phase II ECOG trial of irinotecan/docetaxel with or without cetuximab in metastatic pancreatic cancer: updated survival and CA19-9 results. J Clin Oncol (Meeting Abstracts) 2008; 26:4642.
- Sinnaeve PR, Van de Werf FJ. Will oral antithrombin agents replace warfarin? Heart 2004; 90:827-8. [PMID 15253941]


