Stephen P Hoole*, Duncan C McNab, Bushra S Rana, William R Davies, Leonard M Shapiro
Department of Cardiology, Papworth Hospital, Cambridge, UK
*Corresponding Author:
Stephen Hoole
Tel: +44 1480 364119
Fax: +44 1480 364799
E-mail: stephen.hoole@papworth.nhs.uk
Citation: Hoole SP, McNab DC, Rana BS, et al. Room to Rotate Encourages Amplatzer Septal Occluder Cobra Head Configuration. Interv Cardiol J 2015, 1:1. DOI: 10.21767/2471-8157.10003
Cobra head configuration of the Amplatzer Septal Occluder (ASO) is a benign but potentially avoidable phenomenon, occurring in approximately 3% of implantations. The mechanism of deformation is thought to occur due to device rotation and twisting of the ASO nytinol wires either in the delivery catheter or following interaction with adjacent heart structures e.g. left atrial wall after delivery.
Cobra head configuration of the Amplatzer Septal Occluder (ASO) is a benign but potentially avoidable phenomenon, occurring in approximately 3% of implantations [1]. The mechanism of deformation is thought to occur due to device rotation and twisting of the ASO nytinol wires either in the delivery catheter or following interaction with adjacent heart structures e.g. left atrial wall after delivery [2,3]. Larger devices may be more prone to this phenomenon due to a greater length between disc margins and centre of the device that may twist. In our experience, deformation usually occurs prior to device exit from the catheter particularly when the delivery catheter diameter is larger than that recommended by the manufacturer.
In the case illustrated, implantation of a 16 mm ASO device was attempted using 10F delivery catheter rather than the 7F catheter recommended. Figure 1a clearly demonstrates that the left atrial (LA) disc is eccentric and deformed in the catheter prior to exiting and a cobra head configuration is subsequently seen (Figure 1b and Figure 1c) on attempting deployment. The same configuration could be induced by rotating the LA disc manually outside of the patient after retrieval (Figure 2). The defect was successfully closed using a 20 mm ASO using a 9F delivery catheter.
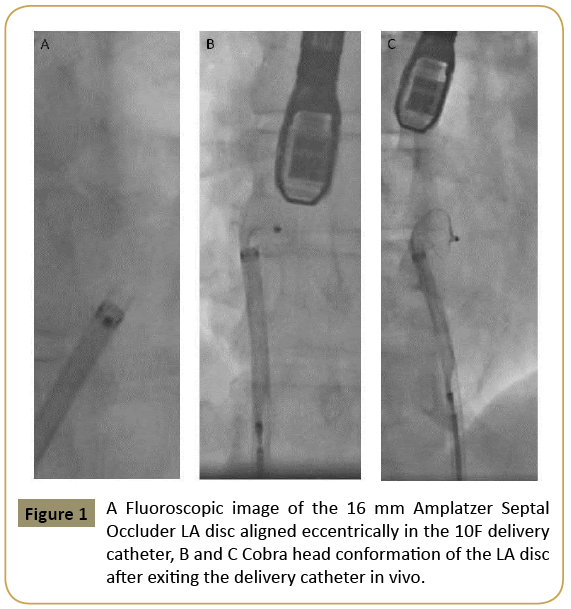
Figure 1: A Fluoroscopic image of the 16 mm Amplatzer Septal Occluder LA disc aligned eccentrically in the 10F delivery catheter, B and C Cobra head conformation of the LA disc after exiting the delivery catheter in vivo.
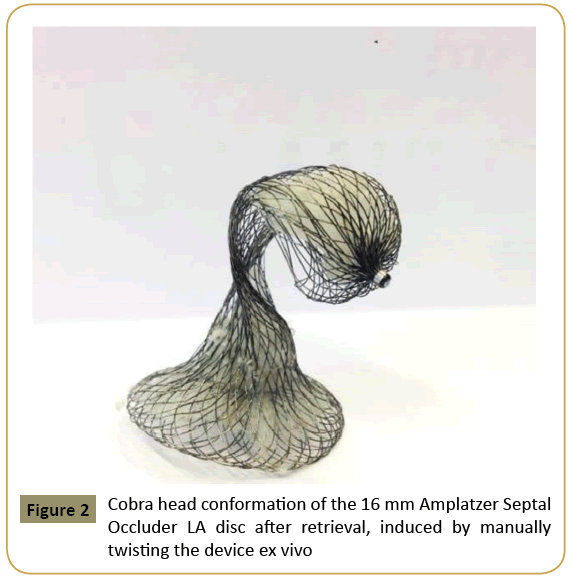
Figure 2: Cobra head conformation of the 16 mm Amplatzer Septal Occluder LA disc after retrieval, induced by manually twisting the device ex vivo
Two of the other three cobra head case reports in the literature also used larger than recommended catheters: 14F rather than 12F for a 40 mm device and a 13F rather than a 9F for a 24 mm device [4,5]. Larger catheters have lower compressive frictional forces that may allow device torsion particularly when negotiating tortuous iliac vessels where rotational forces on the device may be greater. Our case highlights the importance of following manufacturer recommended sheath sizes for optimal device implantation.
References
- Fischer G, StiehJ, Uebing A, Hoffmann U, Morf G, et al. (2003) Experience with transcatheter closure of secundum atrial septal defects using the Amplatzerseptaloccluder: a single centre study in 236 consecutive patients. Heart 89:199-204.
- Cooke JC, Gelman JS, Harper RW (2001) Cobrahead malformation of the Amplatzerseptaloccluder device: an avoidable compilation of percutaneous ASD closure. Catheter CardiovascInterv52:83-85.
- Waight DJ, Hijazi ZM (2001) Amplatzer devices: Benign Cobrahead formation. Catheter CardiovascInterv52:86-87.
- Trehan V, Mukhopadhyay S, Yusuf J, Gupta MD, et al. (2005) Cobra head deformity of Amplatzerseptaloccluder. Indian Heart J 57:78-79.
- Estevez-Loureiro R, Martinez-Bendayan I, Salgado-Fernandez J, Rueda-Nunez F (2010) Cobra-like deformation of amplatzer devices used for closing atrial septal defects: can it be avoided? Rev EspCardiol63:495-496.

