Keywords
Electronic health record; Navigation time; Health system; Primary health care; Secondary health care; Referral; Transition care; Emergency department; Outpatient care specialist
Abbreviations
HER: Electronic Health Record; HL7: Health Level Seven International Organization; IHE: Integrating the Healthcare Enterprise; LAB-Rep: Database of the Laboratory test reports; LDAP: Lightweight Directory Access Protocol; PHC: Primary health care; PIN: Personal Identification Number; RAD-Rep: Database of the Radiology Test Reports; RFID: Radio Frequency Identification; SAML: Security Assertion Markup Language; SD: Standard Deviation; SHC: Secondary Health Care; XDS.b: Cross-Enterprise Document Sharing IHE Integration Profile
Background and Significance
Electronic Health Record (EHR) is a term used to portray a “repository of information regarding the subject of care in machine-processable format” [1]. However, the meaning and representation of the EHR changes throughout the different reports in the literature [2,3].
This case study focuses on the concept of citizen’s EHR (National Patient Registry) [4], which is a repository of health data and information in electronic format, being referred to any user of a unified and universal health system, or rather, for all the residents of a health district.
Such health systems most commonly represented in Western European countries and in Brazil, are bound by law to provide all citizens with medical care under three referral levels, namely: Primary Health Care (PHC), Secondary Health Care (SHC), including hospital in-patient care and outpatient care and Tertiary Care (highly specialized care). Whenever the patient is referred or counter-referred from one level to another (transition care), the vulnerability to medical error increases, due to the loss of information on the past and present clinical situation [5].
The citizen’s (becoming the patient’s with illness) EHR is intended to be the source of updated health information of the highest degree of objective reliability and legal force, according to the national regulations [6]. Such a tool enables the acting health professional to become quickly aware altogether of the clinical history, of the clinical tests reports (laboratory, radiology, pathology, etc.) and of the previous therapeutic prescriptions with poor or no support from the patient’s often uncertain memory. Thus, the databases, feeding into the citizen’s EHR in real time, must be fully interoperable, cleaned, updated and legally cleared by authorized health system officials [7]. Afterwards, the health professional can provide a diagnostic and therapeutic strategic approach, according to a holistic vision of the patient, minimize the probability of mistakes and maximize the continuity of care.
In 2006, the government of Marche Region (Central Italy), which manages the public health system, launched a pilot project to develop and implement the citizen’s EHR throughout the health district of Ascoli Piceno.
All the identification codes that any information systems of health facilities were generating were abolished. The citizen’s unique fiscal code became the only identification tool for the EHR. The application of the citizen’s EHR became fully operational by 2008.
The present observational case study seeks to estimate the extent that medical doctors and citizens make use of the EHR application. The trends of some indicators were estimated over three years’ time (2013-2015), namely: 1) the number of citizens and medical doctors of several categories, grouped in levels of care, who opened a personal account and accessed the EHR application; 2) the total number of logins, the overall navigation time and the mean number of logins and navigation time per citizen and per group of medical doctors.
Materials and Methods
The environment of implementation of the EHR
The geographical and human context where the health services of this pilot project are set-up is shown in Figure 1.
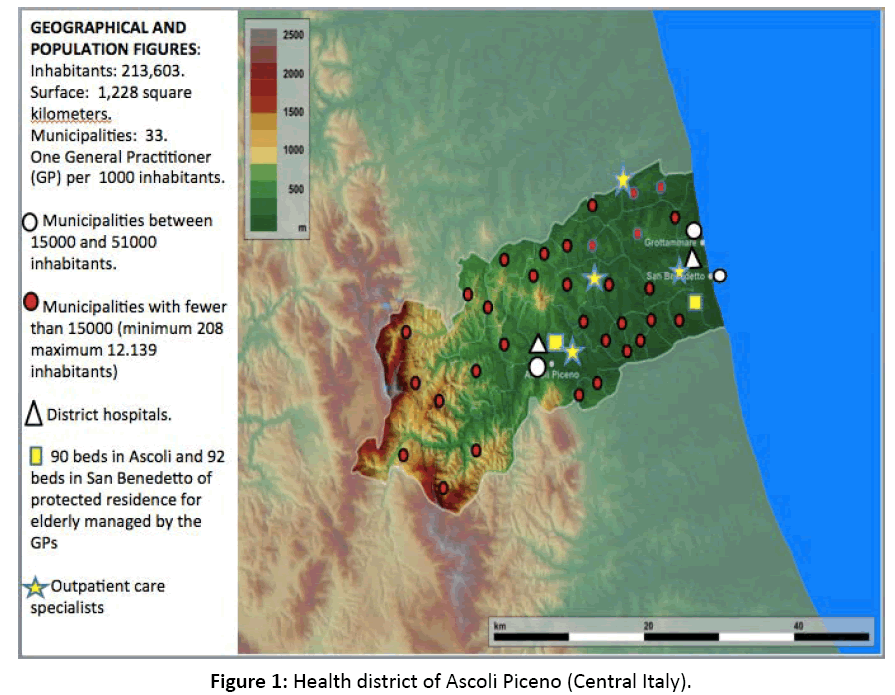
Figure 1: Health district of Ascoli Piceno (Central Italy).
The steadiness of the context over 2013-2015, regarding population, availability of health facilities, clinical services and medical doctors in force was confirmed through the Marche Region’s official reports.
Governance
The software company NBS finalized the EHR application in 2008. With the permission of the Directorate of the health district, NBS took over the responsibility of setting up rules for secure login to data by the users, according to the profile of the applicant.
Architecture
The application infrastructure meets the technical requirements and standards. The technology architecture is web native, homogeneous, distributed, and scalable, computing on three distinct levels in a classic web model "thin-client":
a) Presentation Layer with advanced graphical user interface;
b) Application Layer configured in Apache and Tomcat technology;
c) Level Data which hosts the database manager.
All software components are fully and natively integrated and supported by the same technology stack.
Interoperability
The proposed solution conforms to the HL7 IHE integration profiles, including the standard XDS.b for documents sharing [8]. The interoperability schema involving national, regional and departmental systems is shown in the Figure 2.
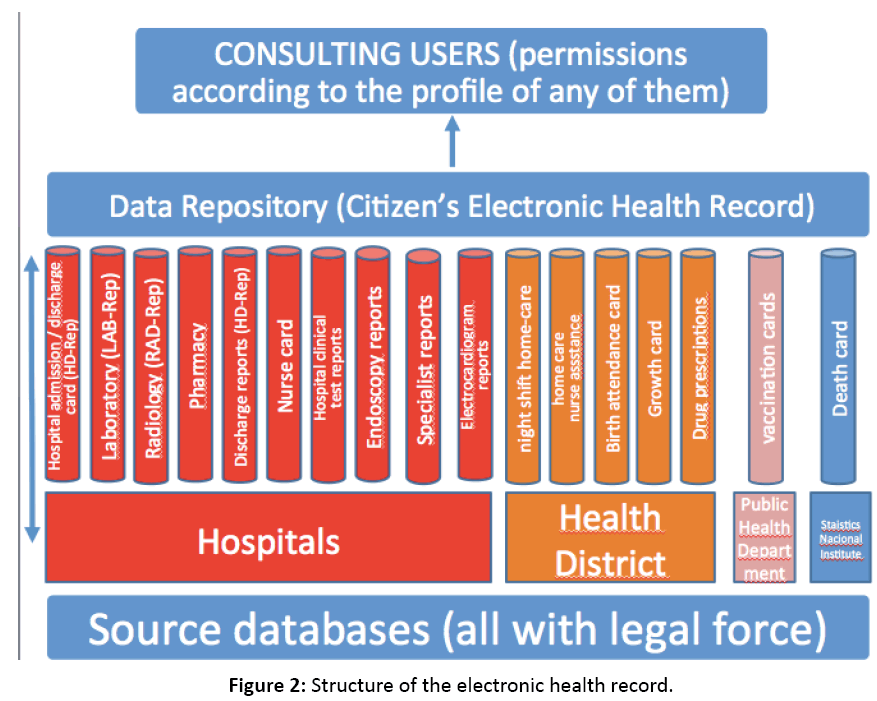
Figure 2: Structure of the electronic health record.
Technical requirements
The information system is designed in accordance with the technical and national safety regulations established by the Information Technology public administration.
The system adopts the following technologies:
a) Solutions as business continuity, disaster recovery and open source framework assure reliability and sustainability.
b) Usability and accessibility requirements are satisfied by graphic interface realized in compliance with international and national standards [9].
c) User authentication process compatible with Personal Identification Number (PIN), token, smart cards and certificates are issued by the Certification Authority through Lightweight Directory Access Protocol (LDAP) and Active Directory Technologies or Federated Applications protocols as Security Assertion Markup Language (SAML) 2.0, in compliance with national standards on safety and privacy.
d) User profiling permits and controls only the authorized operations.
e) Digital signature for signing reports and clinical documents.
f) Advanced Electronic Signature to dematerialize documents such as “informed consent”, “privacy consent”, etc, released by the citizens/patients.
g) Automatic identification of patients via Radio Frequency Identification (RFID).
Health Information in the EHR
The EHR assembles the entire physiological, family and past medical history of the citizen. It is assembled by collecting and storing single citizen related information from the records of source databases from hospital, health district, public health department, and National Institute of Statistics.
All data can be modified only through errata-corrige traceable proceedings.
Groups of medical doctors
The medical doctors were divided into PHC Doctors and SHC Doctors, since there was no third level of care. The SHC Doctors were divided into four sub-groups, namely: 1) Hospital Service Doctors; 2) Hospital Clinical Unit Doctors; 3) Hospital Emergency Department Doctors and 4) Outpatient Care Specialists.
In addition to the medical doctors, other groups of professionals may access the EHR, such as nurses of homecare nursing assistance, physiotherapists, pharmacists and psychologists; however, these were not considered for the purpose of this study.
Indicators of EHR use
Among all the groups and sub-groups of doctors and citizens, the indicators of satisfaction were evaluated in 2013, 2014, and 2015, in order also to estimate the trend. These indicators were: 1) Number and percentage of account subscribers among the entitled persons; 2) Number of account subscribers having logged in during the year (at least ten times if a doctor and once if a citizen); 3) Total number of logins per group and sub-group of doctors and per citizen per year; 4) Total number of hours of web navigation in the application per group and sub-group of doctors and per citizen per year; 5) Mean + SD of logins and navigation time per doctor and citizen.
Whenever feasible, based on the number of working hours established by the national job contract of any group and sub-group of doctors, the following indicators were also calculated: a) mean number of logins per working day; b) mean number of minutes of navigation time per working day; c) percentage of time of navigation within the total working time as determined by the job contract.
Results
According to the official records from the health district, the health facilities (hospitals, hospital beds, laboratories, radiology department, pathology departments, outpatient care specialist centers) and the number of the workforce of PHC doctors (221) and SHC doctors (290) remained unchanged over 2013-2015.
Use of the EHR by PHC doctors
The indicators of use of the EHR by the PHC doctors are displayed in Table 1.
| PHC doctors |
| |
2013 |
2014 |
2015 |
Delta 2013-15 or p |
| Credited PHC doctors (100% of account subscribers) |
221 |
221 |
221 |
0% |
| More than 10-time logging in PHC doctors and percentages on the total of credited PHC doctors |
218 (99%) |
216 (97%) |
209 (94%) |
-4% |
| Total number of logins |
77,942 |
71,968 |
65,272 |
-16% |
| Total number of hours of navigation time |
73,117 |
68,811 |
61,697 |
-16% |
| Mean navigation time in minutes per login |
56’ |
52’ |
56’ |
0% |
| Mean number of logins per doctor per year ± SD |
344 ± 336 |
318 ± 322 |
319 ± 341 |
ns |
| Mean number of hours of navigation time per doctor per year ± SD |
322 ± 363 |
305 ± 358 |
306 ± 392 |
ns |
| Mean number of logins per doctor on a working day base (250 working days per year) |
1,4 |
1,3 |
1,3 |
-7% |
| Number of minutes of navigation time on a working day base (250 working days per year) |
76’ |
72’ |
74’ |
-3% |
PHC doctors are: a) General Practitioners, who may have up to a maximum of 1500 patients over fifteen years old enrolled and are on duty from 8 a.m. to 8 p.m. from Monday to Friday; b) Paediatricians, who may have up to a maximum of 700 patients under fifteen years old enrolled and are on duty from 8 a.m. to 8 p.m. from Monday to Friday; c) The Night Shift Home-Care Doctors on duty from 8 p.m. to 8 a.m. from Monday to Friday and 12 a.m. to 12 a.m. on Saturdays, Sundays and national holidays
Table 1: Use of the EHR by the PHC doctors.
Most noteworthy is that: a) the account subscribers remained steady at 221; b) 94-99% of the account subscribers logged in throughout the year; c) mean navigation time per single login ranged from 52’ to 56’; d) the number of logins ranged from 1.3 to 1.4 per working day; e) the calculated mean time of navigation per single working day ranged from 72’ to 76’.
Use of the EHR by SHC doctors
Such results are summarized in Table 2.
| |
2013 |
2014 |
2015 |
Delta 2013-15 or p |
Hospital Services Doctors
(they input data into the databases LAB-Rep and RAD-Rep) |
| Total number |
44 |
44 |
44 |
- |
| Account subscribers |
2 |
2 |
3 |
+1 |
| Logins to the account |
881 |
656 |
458 |
-48% |
| Number of hours of navigation |
26,430 |
19,680 |
13,040 |
-51% |
| Hospital Clinical Unit Doctors (they input data into all the databases from hospitals with the exceptions of LAB-Rep and RAD-Rep) |
| Total number |
154 |
154 |
154 |
- |
| Number of doctors logging in and percentage over the total number |
89 (57%) |
99 (64%) |
116 (75%) |
+18% |
| Total number of logins |
22,260 |
20,671 |
22,474 |
+1% |
| Total number of hours of navigation |
11,097 |
10,305 |
11,199 |
+1% |
| Mean number of minutes of navigation time per login |
30’ |
30’ |
30’ |
- |
| Mean ± SD of number of logins per year among the doctors logging in |
186 ± 202 |
168 ± 191 |
158 ± 185 |
ns |
| Mean ± SD of navigation time hours per year among the doctors logging in |
84 ± 95 |
81 ± 91 |
78 ± 92 |
ns |
| Mean number of minutes of navigation time per working day (250 working days per year) |
21’ |
19’ |
19’ |
-2’ |
| Percentage of doctors’ working time taken by the navigation in the EHR (380 min make up the working day time) |
5.5 |
5.0 |
5.0 |
-0.5% |
Hospital Emergency Department Doctors
(They input data into the database HD-Rep) |
| Total number |
31 |
32 |
33 |
+2 |
| Number of doctors logging in and percentage over the total number |
24 (77%) |
27 (84%) |
28 (84%) |
+7% |
| Total number of logins |
12,890 |
14,483 |
14,374 |
+11% |
| Total number of hours of navigation |
37,687 |
39,236 |
38,517 |
+2% |
| Mean number of minutes of navigation time per login |
175’ |
162’ |
161’ |
-8% |
| Mean ± SD of number of logins per year among the doctors logging in |
537 ± 227 |
536 ± 201 |
513 ± 199 |
ns |
| Mean ± SD of navigation time hours per year among the logging-in doctors |
1,168 ± 536 |
1,075 ± 393 |
1,064 ± 411 |
ns |
| Mean number of logins in a working day (250 working days per year) |
2.1 |
2.1 |
2.0 |
-5% |
| Mean number of minutes of navigation time per working day (250 workings day per year) |
280’ |
258’ |
255’ |
-9% |
| Percentage of doctors’ working time taken by the navigation in the EHR (380 min make up the working day time) |
74 |
68 |
67 |
-7% |
| Outpatient Care Specialists |
| Total number |
58 |
58 |
58 |
- |
| Number of logging-in doctors and percentage over the total number |
31 (52%) |
33 (56%) |
33 (56%) |
+4% |
| Total number of logins |
5297 |
5900 |
6175 |
+17% |
| Total number of navigation time hours |
2642 |
2943 |
3079 |
+16% |
| Minutes of navigation time per login |
30’ |
30’ |
30’ |
- |
| Mean ± SD of logins per year |
184 ± 131 |
190 ± 135 |
192 ± 136 |
ns |
| Mean ± SD of navigation time hours per year |
94 ± 66 |
95 ± 67 |
96 ± 68 |
ns |
| Percentage of doctors’ working time taken by the navigation in the EHR out of the mean of the total yearly working time (1058 h) |
9 |
9 |
9 |
- |
The SHC doctors include four sub-groups: a) Hospital Service Doctors (Laboratory, Radiology, Pathology); b) Hospital Clinical Unit Doctors; c) Hospital Emergency Department Doctors; d) Outpatient Care Specialists (20 specialties)
Table 2: Use of the EHR by the SHC doctors.
Most noteworthy is that: a) Only two Hospital Service Doctors out of forty four subscribed to the account; b) total logins and total number of hours of navigation time by the Hospital Service Doctors decreased from 2013 to 2015 by 48% and 51% respectively; c) the number of Hospital Clinical Unit doctors who logged in increased from 89 to 116 over 2013-2015; d) logins by the Hospital Clinical Unit doctors increased from 20,671 times in 2014 to 22,474 in 2015, and their number of hours of navigation time increased as well from 10,305 to 11,119; e) on average, the Hospital Clinical Unit doctors remain logged in from 19’ to 21’ per day, which represents 5.0% and 5.5% of their daily working time; f) with regards to Hospital Emergency Department doctors, the number of logins and navigation time increased by 7%, 11%, and 2% from 2013 to 2015; g) the mean number of minutes the Hospital Emergency Department doctors remain logged in ranged from 280’ to 255’, which represents 74 and 67% of their daily working time; h) for the percentage of logging-in Outpatient Care Specialists, their total number of logins and number of hours of navigation increased by 4%, 11%, and 16%, respectively; i) on average, the mean number of minutes of navigation per single login by the Outpatient Care Specialists remained steady at 30’; j) the percentage of time spent in navigation out of the total number of yearly working hours of the Outpatient Care Specialists was maintained at 9%.
Use of the EHR by the citizens
The number of account subscribers increased from 12,873 in 2013 to 28,468 in 2015, representing only 6 and 13% of the resident population respectively, with an increase of 30% over two years’ time, yet only an increase of 7% within the whole resident population.
Over 2013-2015, 67, 59 and 37% of the account-subscribing citizens logged into their EHR.
Despite the increased number of account subscribers, the total number of logins decreased from 120,910 in 2014 to 76,518 in 2015, therefore the mean number of logins per citizen decreased as well from 10 to 7 per year.
Also the total number of hours of navigation decreased from 76,900 to 56,143.
However, the mean number of minutes of navigation per single login increased from 38’ to 44’ (19%).
Discussion and Conclusion
The PHC doctors have been consulting the EHR at a high rate, almost at 100%, with a daily navigation time of 72-76 minutes, but also with large standard deviations in the number of logins. Since they were never given incentive to encourage their use of the EHR application, we can state that they really seem to perceive the tool as supportive.
The Hospital Services Doctors feed some of the databases (LAB-Rep, RAD-rep), which make up the source of information of the EHR, through their reports. Thus, they do not need to log into the EHR application and do not make decision through it.
The increasing number of logins by Hospital Clinical Unit doctors seems to indicate that they are still exploring the benefits of having an EHR available. Moreover, the large standard deviations in logins and in navigation time suggest a high variability of interface with the EHR.
Roughly, we can state the same increasing trend with large variation within the sub-group of the Outpatient Care Specialists, whose use of the EHR still lags behind at 56%.
84% of the Hospital Emergency Department doctors log into the EHR, which is definitely a high percentage. Actually, all the results give evidence that this sub-group makes the strongest use of the EHR. Since the Emergency Departments are the border between PHC and SHC, such sustained use confirms that EHR is an important tool in transition care, as Wenger and Young already reported in elderly patients [10].
With regards to citizens, the coverage in account subscription is moving forward slowly. The citizen is rarely concerned with consulting his EHR. This data is confirmed by the survey of Patel et al., who realized that only 54% of the people seek to consult their online health records and that 73% of the group logging-in does so merely to check health test reports or medications. Moreover, 37% of these continue experiencing some kind of gap in retrieving and handling information from their health records [11].
In literature, we recall the experience of the Department of Veterans Affair, which made available an EHR (Blue Button application) to be downloaded by the customer/owner and, upon his consent, made available to health providers. The benefit is reportedly enjoyable only by the customer/owner when achieving a better understanding of his clinical situation in that the personal health information is in one place [12].
Although it is undisputable that the ownership of health data, being retrievable out of the citizen’s EHR, belongs to the citizen, we emphasize that the EHR application of our experience was created within the health system and must be managed by health professionals as a tool for improving the performance of health care providing.
Acknowledgement
The authors acknowledge the government of Marche Region who funded the implementation of the EHR.
Funding Sources
The government of Marche Region funded the implementation of the EHR through a grant in 2006.
References
- Kohl LF, Crutzen R, de Vries NK. Online prevention aimed at lifestyle behaviors: A systematic review of reviews. J Med Internet Res 2013; 15: e146.
- Adaji A, Schattner P, Jones K. The use of information technology to enhance diabetes management in primary care: A literature review. Inform Prim Care 2008; 16: 229-237.
- vanPoelgeest R, Heida JP, Pettit L, de Leeuw RJ, Schrijver G. The association between eHealth capabilities and the quality and safety of health care in the Netherlands: Comparison of HIMSS analytics EMRAM data with Elsevier’s ‘The Best Hospitals’ data. J Med Syst 2015; 39: 90.
- Gubbels S, Nielsen KS, Sandegaard J, Mølbak K, Nielsen J. The development and use of a new methodology to reconstruct courses of admission and ambulatory care based on the Danish National Patient Registry. Int J Med Inform 2016; 95: 49-59.
- Campanella N, Morosini P, Sampaolo G, Catozzo V, Caso A, et al. Medical teleconsultation to general practitioners reduces the medical error vulnerability of internal medicine patients. Eur J Intern Med 2015; 26: 675-679.
- Civile C. The electronic health card being edited by a public health system officer (art.357 CP) or an in-charge of public health service is a public act. Italian law reference.
- van Velthoven MH, Mastellos N, Majeed A, O’Donoghue, Car J. Feasibility of extracting data from electronic medical records for research: an international comparative study. BMC Med Inform Decis Mak 2016; 16: 90.
- https://www.hl7.org
- https://www.w3.org/TR/WCAG20
- Wenger NS, Young RT. Quality indicators for continuity and coordination of care in vulnerable elders. J Am Geriatr Soc 2007; 55: S285-S292.
- Patel V, Barker W, Siminerio E. Individuals’ Access and use of their online medical record nationwide. The office of the National Coordinator for health information technology. ONC Data Brief 2016; 20.
- Turvey C, Klein D, Fix G, Hogan TP, Woods S. Blue button use by patients to access and share health record information using the department of veteran’s affairs’ online patient portal. J Am Med Inform Assoc 2014; 21: 657-663.

