Keywords
Diabetes Mellitus; India; Pancreatitis, Chronic
Abbreviations
ACP: alcoholic chronic pancreatitis; FCPD: fibrocalculous pancreatic diabetes; HDL: high density lipoprotein; LDL: low density lipoprotein; WHO: World Health Organization
INTRODUCTION
The most common forms of diabetes worldwide are type 2 and type 1, but about 1-5 percent of patients with diabetes seen at many centers are due to diabetes secondary to other diseases, of which disorders of the pancreas are the most common [1]. Various pancreatic disorders can cause diabetes including infections, inflammation, neoplasms, post pancreatic surgery, cystic fibrosis or hemochromatosis, but chronic pancreatitis is the commonest pancreatic disorder associated with diabetes [2].
Alcohol abuse is reported to be the most common cause of chronic pancreatitis worldwide, especially in the west [3]. However, in tropical countries like India, there is an idiopathic variety of juvenile onset chronic, calcific, non-alcoholic pancreatitis called ‘tropical chronic pancreatitis’ which is associated with undernutrition [4, 5]. The diabetes secondary to tropical chronic pancreatitis was termed ‘fibrocalculous pancreatic diabetes’ (FCPD) by a World Health Organization (WHO) Study Group [6, 7]. We have earlier described the clinical features of FCPD [8, 9, 10]. The diabetes is severe and about 80% require insulin for control, but ketosis and ketoacidosis are rare [8, 9, 10, 11]. This has been attributed to partially preserved beta cell function [12], low glucagon levels [13], low fat mass [11] and carnitine deficiency [14]. Till date, only 5 cases of diabetic ketoacidosis have been reported among FCPD patients [9]. There are only two population based studies on this condition: both in India, one on tropical chronic pancreatitis from Kerala [15] and the other on FCPD from Chennai [16]. Recent studies from India suggest that tropical chronic pancreatitis may be on the decline due to improved nutrition, while alcoholic chronic pancreatitis (ACP) might be increasing because of increase in alcohol use [17]. However, there are no reports on the prevalence of diabetes secondary to chronic pancreatitis in developing countries. This study reports on the secular trends in prevalence of FCPD and diabetes secondary to ACP, seen at a diabetes centre in southern India.
METHODS
The study was carried out at Dr. Mohan’s Diabetes Specialties Centre, a large tertiary care centre for diabetes at Chennai (formerly Madras) city in Southern India. Records of all patients registered at the centre are maintained in a diabetes electronic medical record (DEMR) from 1991, one of the largest on diabetes in the world [18]. For purposes of this study, we specifically extracted data on all patients with diabetes secondary to chronic pancreatitis. Patients with type 1 diabetes, type 2 diabetes, gestational diabetes and other forms of diabetes were excluded. A total of 1,079 patients with diabetes secondary to chronic pancreatitis were identified. We excluded 47 patients in whom the diagnosis did not clearly fit into FCPD or diabetes secondary to ACP, because of short duration of alcohol abuse (less than 5 years) or intermittent use of alcohol. The remaining 1,032 subjects were then subclassified as FCPD (n=898; 87.0%) and diabetes secondary to ACP (n=134; 13.0%), based on criteria given below.
FCPD was diagnosed based on the following criteria [8]: i) occurrence in a tropical country; ii) evidence of diabetes mellitus; i.e., fasting plasma glucose greater or equal to 7.0 mmol/L (126 mg/dL) or 2-hour value in oral glucose tolerance test greater or equal to 11.1 mmol/L (200 mg/dL) or random plasma glucose greater than 11.1 mmol/L (200 mg/dL), or subjects on drug treatment for diabetes; iii) evidence of chronic pancreatitis: pancreatic calculi on X-ray abdomen or at least three of the following: 1) abdominal pain since childhood; 2) abnormal pancreatic morphology like ductal dilatation on ultrasonography; CT scan or endoscopic retrograde cholangiopancreatography; 3) steatorrhea; 4) abnormal pancreatic function test based on fecal chymotrypsin test [19]; and iv) absence of alcoholism or other known causes of chronic pancreatitis.
Diabetes secondary to ACP was diagnosed based on the following: i) evidence of diabetes mellitus as defined above; ii) evidence of chronic pancreatitis as defined above; and iii) history of consumption of alcohol equivalent to at least 50 g of ethanol per day for at least 5 years prior to the onset of the disease [20]. Patient details extracted included year of diagnosis of diabetes, demographics including age, sex, height and weight. Body mass index was calculated using the formula weight in kg divided by height in square meters. Biochemical tests included fasting plasma glucose, glycated hemoglobin and lipid profile. Exocrine pancreatic insufficiency was documented in all patients using fecal chymotrypsin test using the cut off value of 5.8 units/g which was the mean minus 2 standard deviations (SD) of the value in the normal people [19]. We calculated the frequency of FCPD and diabetes secondary to ACP as a percentage of all diabetic patients seen at the centre during a period of 20 years (between the years 1991 and 2010) in blocks of five years.
ETHICS
Written informed consent was obtained from all study subjects and the study was approved by the Institutional Ethics Committee of the Madras Diabetes Research Foundation. The study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008.
STATISTICS
The clinical and biochemical characteristics of the study population were described using absolute and relative frequencies for categorical variables and mean and SD for continuous variables. One-way ANOVA was used to compare means and to test the linear trend of continuous variables. The distribution of triglyceride data were significantly skewed (P<0.001) at the Shapiro-Wilk test and was log-transformed before analysis in order to reduce the positive skewness (P=0.003). The changes in prevalence of FCPD and diabetes secondary to ACP were tested using the linear-by-linear chi-square test. Dichotomic data were tested by means of the Fisher’s exact test. All statistical analyses were performed using SPSS version 15.0 for Windows SPSS Inc., Chicago, IL, USA).
RESULTS
Table 1 presents the clinical characteristics of the study population. FCPD subjects were younger than ACP subjects (P<0.001) and 100% of ACP were males. There were no other significant differences in clinical or biochemical factors except for serum triglycerides which were higher among the ACP group (P=0.003).
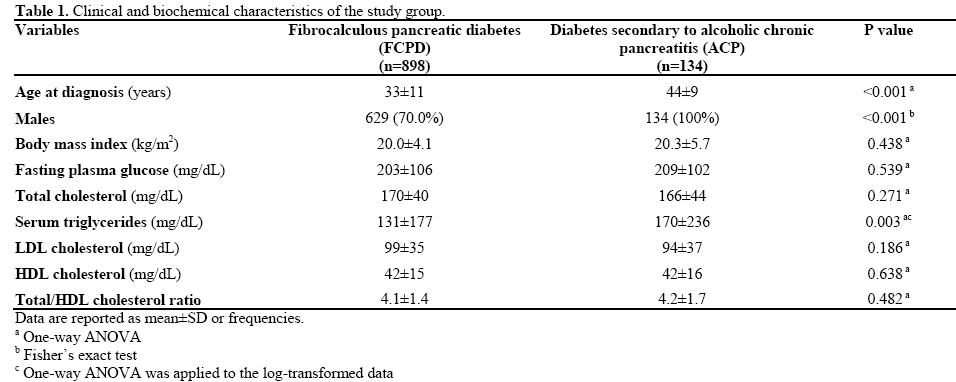
Table 2 shows the number and prevalence of FCPD and diabetes secondary to ACP patients seen at the centre between 1991 and 2010. The prevalence of FCPD decreased from 1.6% of the total diabetic patients seen at the centre during the years 1991-1995 to 0.2% during the years 2006-2010. The actual number of FCPD patients seen at the centre also significantly declined during this period. The prevalence of ACP remained the same (0.1%) throughout the 20 year period of study. However, the number of ACP cases seen at the centre showed a gradual increase, thus paralleling the increase of the number of total diabetes patients registered at the centre.
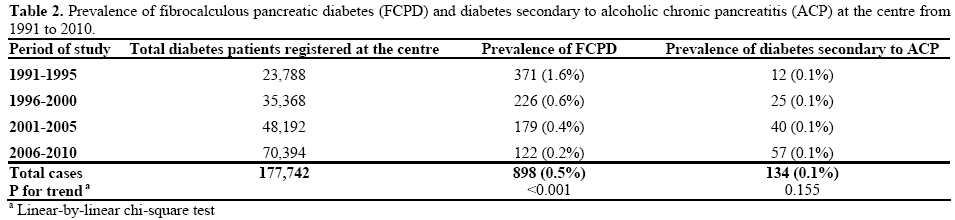
Table 3 shows that there was a significant increase in the BMI of the FCPD subjects from 19.4±3.6 kg/m2 during 1991-1995 to 21.2±3.8 kg/m2 between 2006 and 2010 (P<0.001). There was no significant increase in BMI of the ACP group.
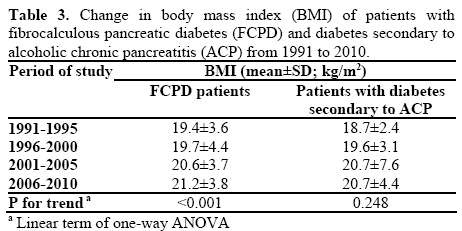
Figure 1 shows that there was a progressive increase in age at diagnosis of FCPD patients during the period of study (P<0.001) while there was a decrease in age at diagnosis of diabetes secondary to ACP (P=0.003).
Figure 1. Change in mean age at diagnosis of patients with
fibrocalculous pancreatic diabetes (FCPD) and diabetes secondary to
alcoholic chronic pancreatitis (ACP) during the years 1991 to 2010.
(Values shown are means and (SDs); the linear term of one-way
ANOVA was applied).
DISCUSSION
The clinical profile of FCPD and diabetes secondary to ACP has been extensively studied by various authors over the years including our group [20, 21, 22, 23, 24]. However, there are no reports to our knowledge on the secular trends in prevalence of diabetes secondary to these two forms of chronic pancreatitis from India. The present study conducted at a tertiary diabetes centre at Chennai in South India, shows the following findings: i) FCPD is still the most common form of chronic pancreatitis, accounting for 87% of the diabetes secondary to chronic pancreatitis seen at the centre; ii) the prevalence and number of FCPD patients has gradually decreased over the years, while the prevalence of ACP has remained constant with a slight increase in numbers; iii) the age at diagnosis of FCPD has increased while that of diabetes secondary to ACP has decreased; iv) the body mass index of FCPD patients has significantly increased during this period, while that of ACP patients has not.
India currently has 62.4 million people with diabetes [25]. While over 95% of these numbers are comprised of type 2 diabetes; South India also has the highest prevalence of FCPD in the world [8, 16]. In 1994, Balaji et al. [15] reported the prevalence of tropical chronic pancreatitis to be 1:793 (36 patients out of 28,567 inhabitants studied) in the South Western state of Kerala state. A study done in Chennai, the capital of Tamil Nadu, a South Eastern state of India, between 2001 and 2003 showed the prevalence of FCPD among self-reported diabetic patients in Chennai city to be 0.36 % (1:276) while it was 0.019% (1:5,200) among the general population [16]. Balakrishnan et al. [17] conducted a nation-wide, clinic based study on chronic pancreatitis and reported that tropical chronic pancreatitis in India was becoming less common. The majority of cases reported in that study comprised of idiopathic pancreatitis (60.2%), while alcoholic pancreatitis comprised 38.7%. However, it is possible that the use of very stringent criteria for labeling tropical chronic pancreatitis in their study (e.g., BMI less than 18 kg/m2, age less than 30 years etc.) could be the reason for the very small number of tropical chronic pancreatitis reported in that study. We [9] and others [21] have shown that there is considerable heterogeneity in the clinical presentation of tropical pancreatitis and the criteria used by Balakrishnan et al. are seen only in about 50% of patients with tropical pancreatitis. Thus the majority of the so called idiopathic pancreatitis in the series reported by Balakrishnan et al. [17] could indeed have had tropical pancreatitis. Moreover, the significant number of alcoholic pancreatitis reported in that study is noteworthy.
The male to female ratio (about 2.5:1) of FCPD patients in this report is similar to that reported by Chari et al. [20] in 1992. However, the mean age at diagnosis of our FCPD subjects appears to be showing a significant increase over the years. Moreover, there was a significant increase in the mean BMI of our FCPD patients over the years. It is thus possible that with improvement in nutritional status, not only is the prevalence of FCPD on the decline, but it is also now occurring at an older age.
Pancreatic enzyme supplements are routinely given to all our chronic pancreatitis patients. We have earlier reported that there was a significant improvement not only in the symptoms of chronic pancreatitis, but also in the quality of life, and indeed, even in control of diabetes after pancreatic enzyme supplementation [26]. About 80% of our FCPD patients need insulin for control of diabetes while the rest who have better preserved beta cell function respond to oral hypoglycemic agents [9]. The ketosis resistance of this group of patients has already been discussed.
Although chronic alcohol abuse is the most common cause of chronic pancreatitis in the West, it accounted for only 13% of diabetes secondary to ACP seen at our centre. Though there is no significant increase in the prevalence of ACP, the actual number of ACP cases appears to be gradually increasing. This has also been reported in the study by Balakrishnan et al. [17]. This can be accounted for by the increase in alcohol consumption in India, perhaps a reflection of the globalization and economic development. It is also possible that there could be some overdiagnosis of ACP. Even in the West, all chronic pancreatitis patients who consume alcohol are reported to have ACP and recent reports suggest that there could be some over diagnosis of this condition [27]. More worrisome is the fact that the mean age of diagnosis of diabetes secondary to ACP seems to be coming down over the years. This is likely because more young Indians are now consuming significant amounts of alcohol.
There are several limitations to this study. Firstly, being an outpatient clinic based study referral bias could have affected the results. In the 1990’s, the senior author (VM) was intensively researching FCPD in collaboration with gastroenterologists which could have led to more referrals to our centre at that time. Secondly, the results obtained in a diabetes centre cannot be extrapolated to the general population even if collected in the same region (South India). Besides, there are significant differences in the clinical profile of chronic pancreatitis even between Southern and Northern parts of India [17]. Finally, the age at diagnosis is based on occurrence of symptoms. Both FCPD and ACP have an insidious onset. Hence, it is possible that patients in both groups could have had a variable period of undiagnosed diabetes. However, the strengths of this study are represented by the large number of patients have been studied and the follow-up period extending to 20 years. Moreover, this is the first report of this kind from India on dealing with the trends in diabetes secondary to chronic pancreatitis.
In summary, this study reports on the secular trends in FCPD and diabetes secondary to ACP, seen at a diabetes centre in South India over a 20-year period from 1991 to 2010. While prevalence of FCPD is declining, that of diabetes secondary to ACP seems to be stable. There is an increase in age at diagnosis of FCPD while there is a decrease in age at diagnosis of ACP. Improved nutritional profile may account at least in part to these findings.
Conflicts of interest
The authors have no potential conflicts of interest
References
- American Diabetes Association. Diagnosis and Classification of Diabetes. Diabetes Care 2010 Jan;33suppl 1:S62-9.
- Chen N, Unnikrishnan IR, Anjana RM, Mohan V, Pitchumoni CS. The complex exocrine-endocrine relationship and secondary diabetes in exocrine pancreatic diabetes. J Clin Gastroenterol 2011;45: 850-61.
- Gullo L Alcohol and chronic pancreatitis. Leading orsecondary etiopathogenic role? Journal of Pancreas 2005; 6(1 suppl):68-72.
- Geeverghese PJ. Calcific Pancreatitis. Bombay: Verghese Publishing House,1985.
- Mohan V, Premalatha G, Pitchumoni CS. Tropical chronic pancreatitis: an update. J Clin Gastroenterol 2003; 36 337-46.
- WHO Study Group Report on Diabetes Mellitus. WHO technical report series 727. WHO, Geneva, 1985, 21-23.
- Rajesh G, Nair AS, Narayanan VA, Balakrishnan V. Tropical pancreatitis and Fibrocalculous Pancreatic Diabetes-two sides of thesame coin? Trop Gastroenterol. 2008; 29:175-6.
- Mohan V, Nagalotimath SJ, Yajnik CS, Tripathy BB. Fibrocalculous pancreatic diabetes. Diab. Metab Rev 1998; 14:153-70.
- Mohan V, Mohan R, Susheela L, Snehalatha C, Barani G, Mahajan VK, et al. Tropical pancreatic diabetes in South India: heterogeneity in clinical and biochemical profile. Diabetologia 1985;28:229-32.
- Mohan V. Fibrocalculous pancreatic diabetes in India. Int. J.Diab. Dev. Countries. 1993;13:14-21.
- Yajnik CS, Sardesai BS, Bhat DS, Naik SS et al. Ketosis resistance in fibrocalculous pancreatic diabetes. Metabolism1997;46:1-4.
- Mohan V, Snehalatha C, Ramachandran A, et al. Pancreaticbeta cell function in tropical pancreatic diabetes. Metabolism1983;32:1091-1092.
- Mohan V, Snehalatha C, Ramachandran A, Chari S, Madanagopalan N, Viswanathan M. Plasma glucagon responses intropical fibrocalculous pancreatic diabetes. Diabetes Res Clin Pract 1990;9:97-101.
- Yajnik CS, Shelgikar KM, Naik SS, et al. The ketosis resistance in fibrocalculous pancreatic diabetes : clinical observations and endocrine and metabolic measurements during oral glucose tolerance test. Diabetes Res Clin Pract 1992;15:149-156.
- Balaji LN, Tandon RK, Tandon BN, Banks PA. Prevalence andclinical features of chronic pancreatitis in southern India. Int J of Pancreatol. 1994 Feb;15(1):29-34.
- Mohan V, Farooq S, DeepaM . Prevalence of fibrocalculous pancreatic diabetes in Chennai in South India ( CURES 61). JOP. JPancreas (Online) 2008; 9:489-492.
- Balakrishnan V, Unnikrishanan AG, Thomas V et al. Chronic pancreatitis: a prospective nationwide study of 1,086 subjects from India. JOP. J Pancreas (Online) 2008; 9: 593-600.
- Pradeepa R, Prabu AV, Jebarani S, Subhashini S, Mohan V.Use of a large diabetes electronic medical record system in India:clinical and research applications. J Diabetes Sci Technol. 2011; 5:543-52.
- Mohan V, Snehalatha C, Ahmed MR, Madanagopalan N, ChariS, Jayanthi V, et al. Exocrine pancreatic function in tropical fibrocalculous pancreatic diabetes. Diabetes Care. 1989;12:145-7.
- Chari ST , Mohan V, Jayanthi V , Snehalatha C, Malathi S,Viswanathan M, Madanagopalan N. Comparative study of the clinical profiles of alcoholic chronic pancreatitis and tropical chronic pancreatitis in Tamil Nadu, Southern India. Pancreas 1992;7:52-8.
- Pitchumoni CS. Special problems of tropical chronic pancreatitis. Clin Gastroenterology 1984: 13: 941-59.
- Mohan V, Chari ST, Viswanathan M, Madanagopalan N.Tropical chronic pancreatitis in Southern India. Proc R Coll Physicians. 1990; 20:34-42.
- Mohan V, Premalatha G, Padma A, Chari ST, Pitchumoni CS.Fibrocalculous pancreatic diabetes. Long-term survival analysis. Diabetes Care 1996;19: 1274-8.
- Balakrishnan V, Nair P, Radhakrishnan L, Narayanan VA. Tropical pancreatitis: a distinct entity or merely a type of chronic pancreatitis? Ind J Gastroenterol; 2006; 25:74-81.
- Anjana RM, Pradeepa R, Deepa M, Datta M, Sudha V, Unnikrishnan R, et al. Prevalence of diabetes and prediabetes (impaired fasting glucose or/ and impaired glucose tolerance) in ruraland urban India. Phase 1 results of the Indian Council of Medical Research - India Diabetes (ICMR-INDIAB) study. Diabetologia. 2011;54:3022-3027.
- Mohan V, Poongothai S, Pitchumoni CS. Oral pancreaticenzyme therapy in the control of diabetes mellitus in tropical calculous pancreatitis. Int J Pancreatology 1998;24:19-22.
- Yadav D, Timmons L, Benson JT, Dierkhising RA, Chari ST. Incidence, prevalence, and survivial of chronic pancreatitis: apopulation-based study. Am J Gastroenterol 2011; 106:2192-9.


