Oliver Neuhaus*, Marina Graf, Jan Ritter, Heinz Ober
Department of Neurology, SRH Kliniken Landkreis Sigmaringen, Sigmaringen, Germany
*Corresponding Author:
Oliver Neuhaus
Department of Neurology, SRH Kliniken Landkreis Sigmaringen, Sigmaringen, Germany
Tel: +4975711002483
E-mail: o.neuhaus@klksig.de
Received date: September 11, 2017; Accepted date: September 11, 2017; Published date: September 13, 2017
Citation: Neuhaus O, Graf M, Ritter J, Ober H (2017) See the Status Epilepticus. Neurosci Brain Imaging. Vol. 1 No. 1: 1.
Copyright: © 2017 Neuhaus O, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
A 50-year-old man with a medical history of epilepsy so far treated with levetiracetam was admitted to our department of neurology with an unprovoked complex focal status epilepticus. He had turned his head first to the right side followed by an adversive movement of the head to the left side. During this period, he was unresponsive to verbal or mechanical stimuli. EEG showed continuous focal sharp wave complexes indicating epileptic activity of the right occipital lobe (Figure 1A). Consistently, MRI made the status epilepticus visible by a region of reduced diffusion at the right occipital lobe (Figure 1B). Only upon treatment escalation to four antiepileptic drugs, levetiracetam, clonazepam, phenytoin, and lacosamide, the status epilepticus could be terminated. EEG as well as MRI normalized subsequently (Figure 1C). No structural MRI abnormalities could be detected at the region of the focal status epilepticus. EEG is the gold standard in capturing epileptic activity in patients especially in nonconvulsive status epilepticus. MRI techniques including diffusion-weighted imaging provide additional information [1,2].
Clinical Image
A 50-year-old man with a medical history of epilepsy so far treated with levetiracetam was admitted to our department of neurology with an unprovoked complex focal status epilepticus. He had turned his head first to the right side followed by an adversive movement of the head to the left side. During this period, he was unresponsive to verbal or mechanical stimuli. EEG showed continuous focal sharp wave complexes indicating epileptic activity of the right occipital lobe (Figure 1A). Consistently, MRI made the status epilepticus visible by a region of reduced diffusion at the right occipital lobe (Figure 1B). Only upon treatment escalation to four antiepileptic drugs, levetiracetam, clonazepam, phenytoin, and lacosamide, the status epilepticus could be terminated. EEG as well as MRI normalized subsequently (Figure 1C). No structural MRI abnormalities could be detected at the region of the focal status epilepticus.
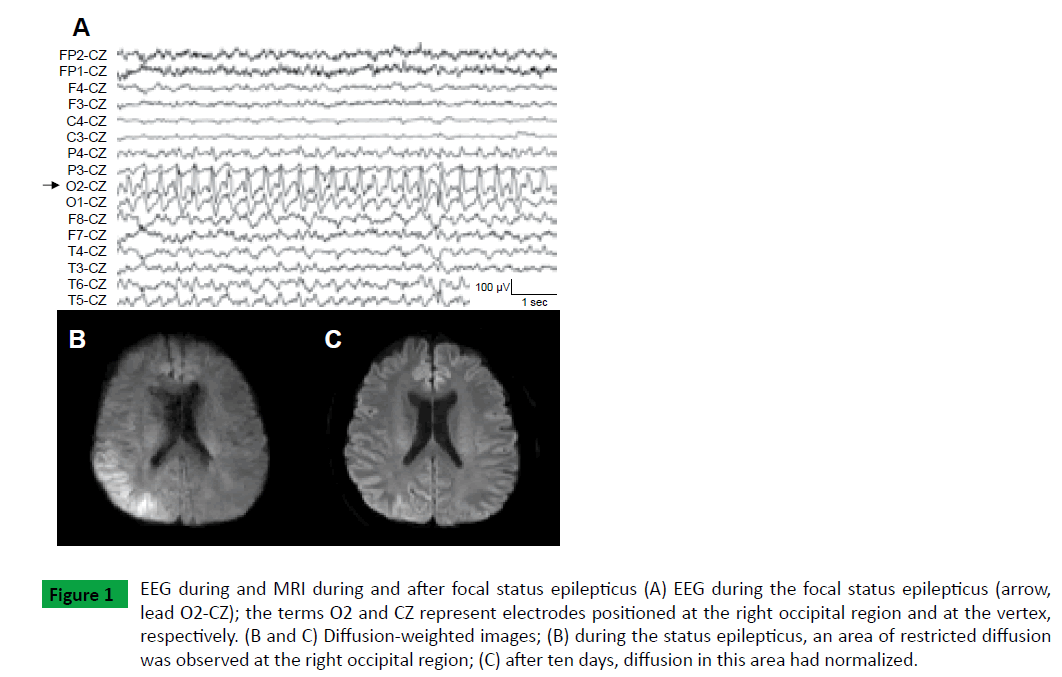
Figure 1: EEG during and MRI during and after focal status epilepticus (A) EEG during the focal status epilepticus (arrow, lead O2-CZ); the terms O2 and CZ represent electrodes positioned at the right occipital region and at the vertex, respectively. (B and C) Diffusion-weighted images; (B) during the status epilepticus, an area of restricted diffusion was observed at the right occipital region; (C) after ten days, diffusion in this area had normalized.
EEG is the gold standard in capturing epileptic activity in patients especially in nonconvulsive status epilepticus. MRI techniques including diffusion-weighted imaging provide additional information [1,2].
References
- Shimogawa T, Morioka T, Sayama T, Haga S, Kanazawa Y, et al. (2016) The intial use of arterial spin labeling perfusion and diffusion-weighted magnetic resonance images in the diagnosis of nonconvulsive partial status epileticus. Epilepsy Res 129: 162-173.
- Mendes A, Sampaio L (2016) Brain magnetic resonance in status epilepticus: A focused review. Seizure 38: 63-67.