Marcos Vinicius Perini1,2, Fabiana Roberto Lima3, Nathan Elie Frenk3, Hilton Muniz Leão Filho3,
Fabricio Ferreira Coelho1, Jaime Arthur Kruger1, Manoel de Souza Rocha3, Paulo Herman1
Department of 1Gastroenterology, Surgical Division, University of Sao Paulo Medical School, Sao Paulo,
Brazil
Department of 2Surgery, University of Melbourne, Australia
Departments of 3Anatomical Pathology and 4Radiology, University of Sao Paulo Medical School, Sao Paulo,
Brazil
- *Corresponding Author:
- Marcos Vinicius Perini
Av Dr Eneas de Carvalho Aguiar, 255 (9th Floor)
São Paulo S.P.
Brazil
Phone : +61 03 422 493 101
E-mail : marcos.perini@usp.br
Received June 18th, 2015-Accepted August 31st, 2015
Keywords
Cystadenocarcinoma, Serous; Cystic Fibrosis; Liver; Neoplasm Metastasis; Pancreas
INTRODUCTION
With the advances in imaging technology, incidental pancreatic cystic lesions can be found in up to 13,5% of adult patients [1]. The majority of neoplastic cysts are classified as serous and mucinous [2]. Serous cystic adenomas are usually benign whereas mucinous cystadenomas have the potential of malignant transformation [3-5]. In 1989, George et al. described serous microcystic adenocarcinoma as a new entity that was pathologically indistinguishable from serous cystadenoma but that displayed malignant behavior [6].
After this preliminary report, others investigators have reported patients with malignant serous cystadenocarcinomas of the pancreas and in a recent retrospective multinational study including 2622 patients, only three serous cystadenocarcinomas (0.1%) were recorded [7].
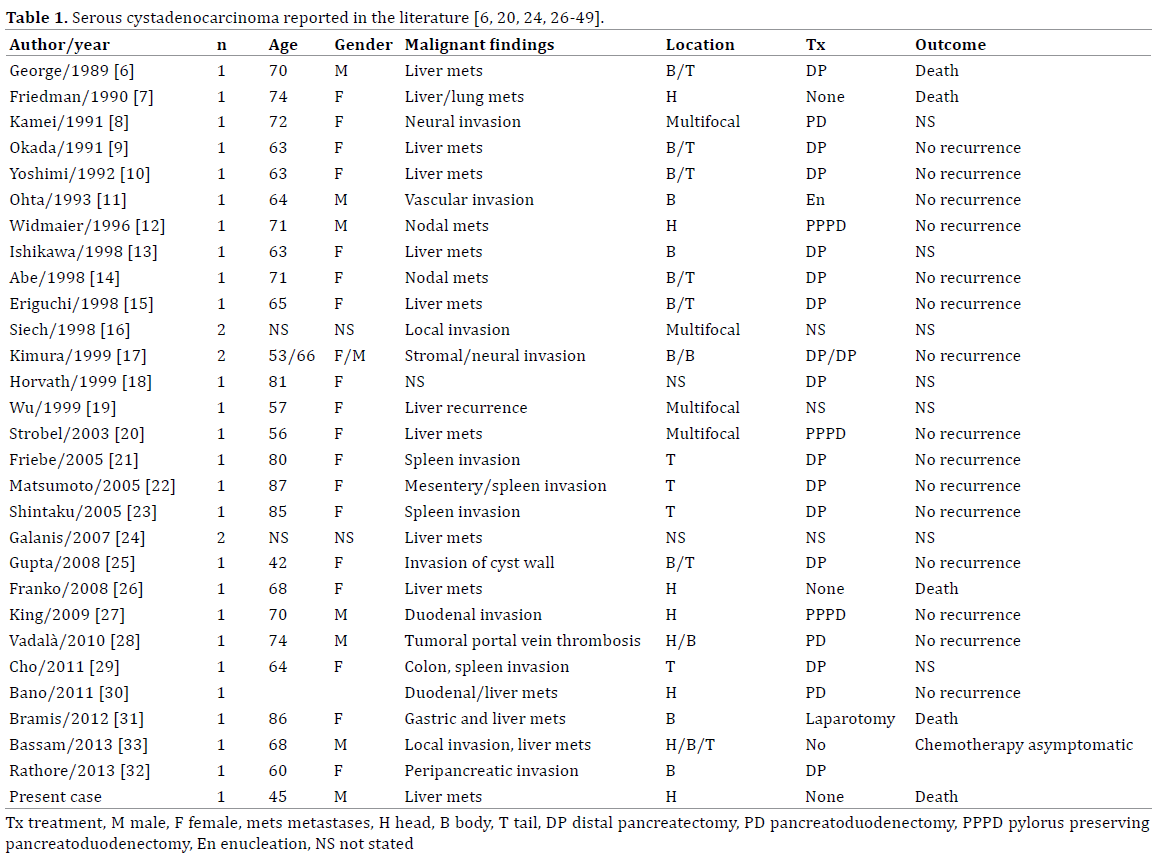
Until now thirty one cases of this very rare entity have been described (Table 1). We report here the clinical, imaging and pathological findings of a patient with a serous cystic neoplasm of the pancreas with malignant behavior, presenting with a pancreatic mass and liver metastases.
CASE REPORT
A forty-five year-old male was referred to our hospital with a 3-month history of weakness and weight loss. Physical examination revealed tenderness on liver palpation and no signs of jaundice.
Laboratory evaluation revealed normal bilirubin levels (1.0 mg/dL – normal <1.5 mg/dL), elevated gamma-GT (261 U/L) and alkaline phosphatase (124 U/l), and normal levels of tumor markers as follows: CA19-9 of 8.1 ku/L (<37), CEA of 0.8 ug/L (<5.0), and AFP of 1.3 ku/L (<10), chromogranin A of 4.1 u/L (0-17.2).
Contrast-enhanced computed tomography (CECT, Figure 1) identified a solid, heterogeneous and predominantly hypervascular mass involving and replacing most of the pancreatic body and tail, measuring 9.5 cm, associated with atrophy and ductal dilatation of the remaining pancreatic tail. The lesion showed strong enhancement in the arterial phase and washout in the portal and delayed phases. Thrombosis of the splenic and superior mesenteric veins and tapering of the celiac trunk branches were also observed. Several other hypervascular masses with the same enhancement pattern were seen throughout the liver, measuring up to 9.3 cm, as well as peripancreatic lymphadenopathy and minimal ascites.
Figure 1. (a.). Arterial phase CECT image shows an infiltrative, heterogeneous, predominantly hypervascular mass involving the pancreatic body (white
arrows) and several hypervascular lesions in the liver. (b.). Portal phase image shows ductal dilation and parenchymal atrophy in the pancreatic tail (black
arrow), as well as peripancreatic lymphadenopathy (black arrowhead) and collateral circulation (black arrow) secondary to splenic vein thrombosis. (c.). Portal phase image shows splenic vein (white arrow) thrombosis secondary to tumor infiltration by the pancreatic mass (black arrowhead); some of the
liver lesions are shown to have necrotic center (black arrow). (d.). Delayed phase shows contrast washout of the liver lesions (black arrows).
Imaging findings were strongly suggestive of a pancreatic primary neoplasm with multiple liver hypervascular metastases, most likely a neuroendocrine tumor. Since the findings were nevertheless inconclusive, an ultrasound-guided percutaneous liver lesion biopsy was performed.
Histology revealed a metastatic tumor composed of sparse fibrous septa and numerous small cysts lined by cuboidal cells with clear cytoplasm and round compact nuclei. The adjacent non-neoplastic hepatic tissue exhibited sinusoidal dilatation due to compression. On immunohistochemical analysis, the neoplastic cells showed diffuse positive staining for 35BH11 (keratin 8) and EMA (epithelial membrane antigen), whereas only rare cells demonstrated immunoreactivity for CEA (carcinoembryonic antigen). Other immunohistochemical markers such as keratins 7 and 20, CD10, TTF-1, chromogranin A, PSA and CDX-2 were negative (Figure 2). Such findings were suggestive of metastatic pancreatic serous cystadenocarcinoma.
Figure 2. Microscopically, (a.). the liver metastasis exhibited multiple cysts, (b.). lined by cells with clear cytoplasm, (c.). as well as fibrous septa.
The patient was referred to oncology and no chemotherapy regimen was offered after case discussion. CECT performed five months later showed disease progression with increased dimensions of the pancreatic mass and of the liver metastases, as well as the presence of ascites. The patient was referred to palliative care and died 18 months after diagnosis.
DISCUSSION
According to the World Health Organization Classification of Tumors, serous cystic neoplasms represent cystic epithelial lesions composed of glycogenrich cells that produce a watery fluid similar to serum. While the vast majority is benign (serous cystadenoma), in rare cases these tumors may be malignant (serous cystadenocarcinoma). Serous cystic neoplasms include serous microcystic adenoma, serous oligocystic and illdemarcated adenoma, von Hippel–Lindau-associated cystic neoplasm, the solid variant of serous cystic adenoma, and serous cystadenocarcinoma. The term serous cystadenoma refers to the serous microcystic type (the most frequent) of these neoplasms [2]. Although the vast majority of these lesions are benign, some of them can invade surrounding tissues and metastasize. In this rare situation it is named cystadenocarcinoma. Until now, 31 cases of serous cystadenocarcinoma have been reported in the English literature as shown in Table 1.
Although some authors refer no gender predilection others report a higher incidence in women. Serous cystadenocarcinoma are mainly located in the pancreatic head, as does its benign counterpart [8, 9].
CECT and magnetic resonance usually are capable to distinguish serous cystic neoplasms from pancreatic pseudocysts and from mucinous lesions if they show a typical microcystic appearance [9, 10]. Although imaging is useful for the differential diagnosis between serous and mucinous tumors, the assessment of tumor malignancy grade is not possible. On the other hand, hypervascular pancreatic lesions composed of a solid stroma and some small cystic lesions without signs of metastases or local invasion may be diagnosed as a benign lesion with an accuracy of 95% [11]. Moreover, imaging of cystic neuroendocrine tumors typically demonstrates a septated cyst with at least a rim of arterially enhancing tissue [12]. These tumors are generally well-circumscribed, and they may demonstrate variable levels of uptake on an indium 111 (111In) pentetreotide scan[13].
There are no radiologic criteria that allow the diagnosis of a malignant cystic lesion, unless tumor infiltration or metastases are present [2]. One study addressing pancreatic cystic lesion using 18-FDG PET found that a positive result strongly suggests malignancy and, therefore, radical resection should be proposed; a negative result indicates a benign tumor that may be treated with limited resection or, in selected high-risk patients, followup [14].
Endoscopic ultrasound-guided cyst fine needle aspiration may help determine the nature of pancreatic cystic lesions [15]. Some reports have shown that cystic fluid CEA levels have a sensitivity and specificity of 87.5% and 44%, respectively, and that high levels of this marker (>250 ng/mL) reliably identify a mucinous neoplasm, whereas values lower than 5 ng/mL can exclude it. High CA 19-9 levels in cyst fluid have been shown to be indicative of mucinous tumors [16]
Moreover, positive mucin staining identifies mucinsecreting lesions. Expression of mucin-like carcinoma associated antigen in the fluid can also be used to differentiate cystadenomas from cystadenocarcinomas and pseudocysts. Mucin staining in conjunction with CEA levels in the cyst fluid appears to be the best approach for the differential diagnosis of pancreatic cystic lesions [17-19].
Immunohistochemical study of serous cystadenoma shows expression of cytokeratins 7, 8, 18 and 19, with the predominance of cytokeratin 7 and 19 [20], and lack of p53 [21] and K-ras mutations [22]. Staining for CEA, trypsin, desmin, actin and factor XIII is also negative [22]. In about 40% of the cases, cells are positive for neuron-specific enolase, but immunostaining for neuroendocrine or islet cell differentiation, such as chromogranin, synaptophysin, insulin, glucagon, somatostatin andVIP is negative [23].
The potential for malignant degeneration of the serous cystic pancreatic lesion is low. Contrary to pancreatic adenocarcinoma that is considered highly aggressive, cystic neoplasms are slow growing and can reach a large size before diagnosis, yet they still have a favorable prognosis. However, there have been an increasing number of case reports describing serous cystadenomas that clinically behave in a malignant fashion. A serous cystadenoma of the pancreas is diagnosed as cystadenocarcinoma when invasion of the surrounding tissue or metastatic spread are present [6]. Since the first description of this malignant behavior, some authors raised concerns regarding “watch and wait” policies for cystic pancreatic lesions. While Hovarth et al. proposed resection for every cystic pancreatic lesion [24], others advocate that the chance of malignancy is lower than the morbidity rate after a pancreatic surgery [25]. Adopting this point of view, those who propose resection agree that close surveillance should be employed and in cases of doubt, resection should be indicated [8, 9, 25].
Although surgical treatment of pancreatic serous cystic lesions is driven by tumor location, growth rate, local complications (such as biliary obstruction), suspicion of malignancy and clinical conditions, the treatment of patients with cystadenocarcinoma is resection whenever possible. On the other hand, some surgeons argue that due to its slow rate of growing, suspicious lesions could be followed and resection offered in selected cases in which lesions increase more than 0.4 cm per year [26].
When dealing with pancreatic cystadenocarcinomas with limited and resectable liver metastases, surgical treatment could be an option in well selected cases. In these cases, where the complete tumor removal is possible, long term survival can be achieved. However in those patients with disseminated disease, as the case described, survival is dismal and depending mostly in empiric treatment and loco-regional complications.
CONCLUSION
Pancreatic cystadenocarcinoma is a rare entity and few cases have been described in the literature. Aggressive surgical treatment is still considered the main treatment option for this rare disease. More importantly, its existence accounts for controversy regarding management of its benign counterpart, the much more common and often incidentally discovered serous cystadenoma of the pancreas.
References
- Lee YT. Cystadenocarcinoma versus pseudocyst of the pancreas: a difficult differential diagnosis. Curr Surg 1989; 46: 202-6. [PMID: 2666031]
- Capella CSE, Klöppel G, Hruban RH. Serous cystic neoplasms of the pancreas, in Pathology and Genetics of Tumours of the Digestive System. WHO Classification of Tumors., A.L. Hamilton SR, Editor 2000; IARC Press: Lyon. 231-233.
- Compagno J, Oertel JE. Microcystic adenomas of the pancreas (glycogen-rich cystadenomas): a clinicopathologic study of 34 cases. Am J Clin Pathol 1978; 69: 289-98. [PMID: 637043]
- Fernández-del Castillo C, Warshaw AL. Cystic tumors of the pancreas. Surg Clin North Am 1995; 75: 1001-16. [PMID: 7660245]
- Warshaw AL, Compton CC, Lewandrowski K, Cardenosa G, Mueller PR. Cystic tumors of the pancreas. New clinical, radiologic, and pathologic observations in 67 patients. Ann Surg 1990; 212: 432-43; discussion 444-5. [PMID: 2171441]
- George DH, Murphy F, Michalski R, Ulmer BG. Serous cystadenocarcinoma of the pancreas: a new entity? Am J Surg Pathol 1989; 13: 61-6. [PMID: 2909198]
- Jais B, Rebours V, Malleo G, Salvia R, Fontana M, Maggino L, Bassi C, et al., Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2015. [PMID: 26045140]
- El-Hayek KM, Brown N, O'Rourke C, Falk G, Morris-Stiff G, Walsh RM. Rate of growth of pancreatic serous cystadenoma as an indication for resection. Surgery 2013; 154: 794-800; discussion 800-2. [PMID: 24074417]
- Valsangkar NP, Morales-Oyarvide V, Thayer SP, Ferrone CR, Wargo JA, Warshaw AL, Fernández-del Castillo C. 851 resected cystic tumors of the pancreas: a 33-year experience at the Massachusetts General Hospital. Surgery 2012; 152: S4-12. [PMID: 22770958]
- Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited. Part I: serous cystic neoplasms. Surg Oncol 2011; 20: e84-92. [PMID: 21237638]
- Maurea S, Fusari M, Imbriaco M, Camera L, Mainenti PP, Campione S, Santangelo M, Salvatore M. Pitfalls in diagnostic imaging of cystic pancreatic masses: a case of true cystic lesion mimicking a mucinous cystadenoma. JOP 2012; 13: 83-6. [PMID: 22233954]
- Bordeianou L, Vagefi PA, Sahani D, Deshpande V, Rakhlin E, Warshaw AL, Fernández-del Castillo C. Cystic pancreatic endocrine neoplasms: a distinct tumor type? J Am Coll Surg 2008; 206: 1154-8. [PMID: 18501813]
- Kalb B, Sarmiento JM, Kooby DA, Adsay NV, Martin DR. MR imaging of cystic lesions of the pancreas. Radiographics 2009; 29: 1749-65.
- Sperti C, Pasquali C, Chierichetti F, Liessi G, Ferlin G, Pedrazzoli S. Value of 18-fluorodeoxyglucose positron emission tomography in the management of patients with cystic tumors of the pancreas. Ann Surg 2001; 234: 675-80.[PMCID: PMC1422093]
- Sarr MG, Kendrick ML, Nagorney DM, Thompson GB, Farley DR, Farnell MB. Cystic neoplasms of the pancreas: benign to malignant epithelial neoplasms. Surg Clin North Am 2001; 81: 497-509. [PMID: 11459267]
- Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW, Fernandez-del Castillo C. Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg 2005; 242: 413-9; discussion 419-21. [PMID: 16135927]
- Sperti C, Pasquali C, Guolo P, Polverosi R, Liessi G, Pedrazzoli S. Serum tumor markers and cyst fluid analysis are useful for the diagnosis of pancreatic cystic tumors. Cancer, 1996. 78:237-43. [PMID: 8673998]
- Sperti C, Pasquali C, Pedrazzoli S, Guolo P, Liessi G. Expression of mucin-like carcinoma-associated antigen in the cyst fluid differentiates mucinous from nonmucinous pancreatic cysts. Am J Gastroenterol 1997; 92: 672-5. [PMID: 9128321]
- Crippa S, Fernández-Del Castillo C, Salvia R, Finkelstein D, Bassi C, Domínguez I, et al. Mucin-producing neoplasms of the pancreas: an analysis of distinguishing clinical and epidemiologic characteristics. Clin Gastroenterol Hepatol 2010; 8: 213-9. [PMID: 19835989]
- Ishikawa T, Nakao A, Nomoto S, Hosono J, Harada A, Nonami T, Takagi H. Immunohistochemical and molecular biological studies of serous cystadenoma of the pancreas. Pancreas 1998; 16:40-4. [PMID: 9436861]
- Fléjou JF, Boulange B, Bernades P, Belghiti J, Hénin D. p53 protein expression and DNA ploidy in cystic tumors of the pancreas. Pancreas 1996; 13: 247-52. [PMID: 8884845]
- Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms of the pancreas revisited. Part IV: rare cystic neoplasms. Surg Oncol 2012; 21: 153-63. [PMID: 21816607]
- Compton CC. Histology of cystic tumors of the pancreas. Gastrointest Endosc Clin N Am 2002; 12:673-96. [PMID: 12607779]
- Horvath KD, Chabot JA. An aggressive resectional approach to cystic neoplasms of the pancreas. Am J Surg 1999; 178:269-74. [PMID: 10587182]
- Allen PJ. Operative resection is currently overutilized for cystic lesions of the pancreas. J Gastrointest Surg 2014; 18:182-3. [PMID: 24165874]
- Friebe V1, Keck T, Mattern D, Schmitt-Graeff A, Werner M, Mikami Y, Adam U, Hopt UT. Serous cystadenocarcinoma of the pancreas: management of a rare entity. Pancreas 2005; 31:182-7. [PMID: 16025006]
- Friedman HD. Nonmucinous, glycogen-poor cystadenocarcinoma of the pancreas. Arch Pathol Lab Med 1990; 114:888-91. [PMID: 2375664]
- Kamei K1, Funabiki T, Ochiai M, Amano H, Kasahara M, Sakamoto T. Multifocal pancreatic serous cystadenoma with atypical cells and focal perineural invasion. Int J Pancreatol 1991; 10:161-72. [PMID: 1748829]
- Okada T, Nonami T, Miwa T, Yamada F, Ando K, Tatematsu A, Sugie S, Kondo T. [Hepatic metastasis of serous cystadenocarcinoma resected 4 years after operation of primary tumors--a case report]. Nihon Shokakibyo Gakkai Zasshi 1991; 88:2719-23. [PMID: 1758093]
- Yoshimi N, Sugie S, Tanaka T, Aijin W, Bunai Y, Tatematsu A, Okada T, Mori H. A rare case of serous cystadenocarcinoma of the pancreas. Cancer 1992; 69:2449-53. [PMID: 1568167]
- Ohta T, Nagakawa T, Itoh H, Fonseca L, Miyazaki I, Terada T. A case of serous cystadenoma of the pancreas with focal malignant changes. Int J Pancreatol 1993; 14:283-9. [PMID: 8113630]
- Widmaier U, Mattfeldt T, Siech M, Beger HG. Serous cystadenocarcinoma of the pancreas. Int J Pancreatol 1996; 20:135-9. [PMID: 8968870]
- Abe H, Kubota K, Mori M, Miki K, Minagawa M, Noie T, Kimura W, Makuuchi M. Serous cystadenoma of the pancreas with invasive growth: benign or malignant? Am J Gastroenterol 1998; 93:1963-6. [PMID: 9772066]
- Eriguchi N, Aoyagi S, Nakayama T, Hara M, Miyazaki T, Kutami R, Jimi A. Serous cystadenocarcinoma of the pancreas with liver metastases. J Hepatobiliary Pancreat Surg 1998; 5:467-70. [PMID: 9931400]
- Siech M, Tripp K, Schmidt-Rohlfing B, Mattfeldt T, Widmaier U, Gansauge F, Görich J, Beger HG. Cystic tumours of the pancreas: diagnostic accuracy, pathologic observations and surgical consequences. Langenbecks Arch Surg 1998; 383:56-61. [PMID: 9627172]
- Kimura W, Makuuchi M. Operative indications for cystic lesions of the pancreas with malignant potential--our experience. Hepatogastroenterology 1999; 46:483-91. [PMID: 10228848]
- Wu CM, Fishman EK, Hruban RK, Schlott WD, Cameron JL. Serous cystic neoplasm involving the pancreas and liver: an unusual clinical entity. Abdom Imaging 1999; 24:75-7. [PMID: 9933679]
- Strobel O, Z'graggen K, Schmitz-Winnenthal FH, Friess H, Kappeler A, Zimmermann A, Uhl W, Büchler MW. Risk of malignancy in serous cystic neoplasms of the pancreas. Digestion 2003; 68:24-33. [PMID: 12949436]
- Matsumoto T, Hirano S, Yada K, Shibata K, Sasaki A, Kamimura T, Ohta M, Kitano S, et al. Malignant serous cystic neoplasm of the pancreas: report of a case and review of the literature. J Clin Gastroenterol 2005; 39:253-6. [PMID: 15718870]
- Shintaku M, Arimoto A, Sakita N. Serous cystadenocarcinoma of the pancreas. Pathol Int 2005; 55:436-9. [PMID: 15982220]
- Galanis C, Zamani A, Cameron JL, Campbell KA, Lillemoe KD, Caparrelli D, Chang D, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 2007; 11:820-6. [PMID: 17440789]
- Gupta R, Dinda AK, Singh MK, Misra MC. Macrocystic serous cystadenocarcinoma of the pancreas: the first report of a new pattern of pancreatic carcinoma. J Clin Pathol 2008; 61:396-8. [PMID: 18305183]
- Franko J, Cole K, Pezzi CM, Montone KT, Redmond J. Serous cystadenocarcinoma of the pancreas with metachronous hepatic metastasis. Am J Clin Oncol, 2008. 31(6): p. 624-5. [PMID: 19060596]
- King JC, Ng TT, White SC, Cortina G, Reber HA, Hines OJ. Pancreatic serous cystadenocarcinoma: a case report and review of the literature. J Gastrointest Surg 2009; 13:1864-8. [PMID: 19459016]
- Vadalà S, Calderera G, Cinardi N, Manusia M, Li Volti G, Giannone G. Serous cystadenocarcinoma of the pancreas with portal thrombosis. Clin Ter, 2010; 161:149-52. [PMID: 20499029]
- Cho W, Cho YB, Jang KT, Kim HC, Yun SH, Lee WY, Chun HK. Pancreatic serous cystadenocarcinoma with invasive growth into the colon and spleen. J Korean Surg Soc 2011; 81: 221-4. [PMID: 22066125]
- Bano S, Upreti L, Puri SK, Chaudhary V, Sakuja P. Imaging of pancreatic serous cystadenocarcinoma. Jpn J Radiol 2011; 29:730-4. [PMID: 22009426]
- Bramis K, Petrou A, Papalambros A, Manzelli A, Mantonakis E, Brennan N, Felekouras E. Serous cystadenocarcinoma of the pancreas: report of a case and management reflections. World J Surg Oncol 2012; 10:51. [PMID: 22400805]
- Rathore MU, Arif A, Umair B. Serous cystadenocarcinoma of pancreas. J Coll Physicians Surg Pak 2013; 23:430-1. [PMID: 23763806]



