Keywords
Cotinine; NHANES; Chronic pain
Introduction
Exposure to tobacco smoke is a significant public health issue as there are approximately 4700 chemicals present in tobacco smoke of which 250 are known to be toxic or carcinogenic [1]. Most notably, tobacco smoke has nicotine, tar, nitric oxide, carbon monoxide, aromatic amines [2], formaldehyde, benzene, hydrogen cyanide, acetone, and Polonium-210 [3]. Although the prevalence of smoking cigarettes has decreased since the release of the U.S. Surgeon General's Report on Smoking and Health in 1966, there remains approximately 13.4% of the U.S. population who smoke daily and 5.4% who smoke some days [4]. Smoking is associated with approximately 480,000 deaths annually in the U.S., including 42,000 deaths from secondhand smoke (SHS) exposure [5]. The cost of smoking in the U.S. is $300 billion per year ($170 billion in medical care, $156 billion in lost productivity due to premature death) [5]. Even limited or light smoking has health risks. Tobacco usage has been associated with lung diseases, cancers, cardiovascular disease, stroke, mood disorders, rheumatoid arthritis, headache, and fibromyalgia among other diseases and conditions [6,7]. Smoking also has the potential to be a risk factor for chronic pain [6,7].
The conceptual framework of chronic pain is that it is a situation in which a person has an ongoing negative subjective experience with many biopsychosocial factors and interactions (any of which may have clinical significance) [8]. Researchers have varying definitions of the cut-point at which pain is defined as chronic. Typical cut-points are 3 months, 6 months, and 12 months pain duration. In a recent U.S. study, the prevalence of chronic pain, defined as lasting at least 6 months, was 30.7% [9]. Researchers using 2008 Medical Expenditure Panel Survey data estimated 100 million adults in the U.S. had chronic pain and the total costs were from $560 to $635 billion in 2010 dollars [10].
The purpose of this study is to determine the relationship of chronic pain with smoking, SHS exposure, tobacco smoke exposure of unknown source, and non-smoking using serum cotinine (and self-report of living with or not living with someone who smokes in the home) to identify the tobacco exposure groups. The theoretical framework is the biopsychosocial model of health as explained by Ditre, et al. [6] in which, for smoking and chronic pain, there is an interplay or positive feedback loop with greater pain, increased smoking, and maintenance of the tobacco addiction through biomedical, behavioral, cognitive/ affective, and physiological/sensory phenomena in social context. The research hypothesis is that smoking is more strongly associated with chronic pain than non-smoking as measured by serum cotinine level.
Methods
Participants
Data from the National Health and Nutrition Examination Survey (NHANES) 2003-2004 was used for this study. Researchers from the Centers for Disease Control and Prevention conduct surveys of non-institutionalized U.S. civilians using a multistage, stratified probability design. The study design is representative of the U.S. population. All participants provide verbal and written consent. Details of the sampling strategy are available from the NHANES website: https://www.cdc.gov/nchs/nhanes.htm.
This study is a cross-sectional, secondary data analysis of the publicly available, de-identified NHANES 2003-2004 data. The sample for the study of chronic pain and smoking was limited to participants who had no missing data concerning chronic pain, cotinine level, sex, age, race/ethnicity, and responses concerning living with someone who smoked in the home. Participants were also limited to the ages of 20 years and above as the NHANES questions concerning pain were presented to participants who were at least age 20 years. The final sample size was 4429 participants.
Outcome variable: Chronic pain
Chronic pain was the outcome variable. It was derived from 2 NHANES questions. The first question asked of participants was if they had pain that lasted more than 24 hours in the previous month. The second question asked of participants who endorsed the first question, was the length of time that the pain was experienced. Options for the second question were: less than a month; one to less than 3 months; 3 months to less than a year; and greater than a year. For this study, pain lasting at least 3 months was defined as chronic pain, based on the definition of the American College of Rheumatology and previous research [11,12].
Key independent variable: Tobacco smoke exposure (Serum cotinine levels)
Serum cotinine level was the key independent variable. Based upon previous definitions using serum cotinine levels [2,13], a participant was defined as a smoker if he or she had a serum cotinine level above10 ng/mg. A participant was defined as having SHS exposure if he or she self-identified as living in a home in which someone smoked and had a cotinine level greater than 0.011 ng/mg but less than or equal to 10 ng/mg. A participant was defined as having tobacco smoke exposure of unknown source if he or she indicated he or she did not live in a home in which someone smoked and had a cotinine level greater than 0.011 ng/mg but less than or equal to 10 ng/mg. Individuals with nondetectable serum cotinine levels were defined as non-smokers.
Other important variables
Variables considered in the study were selected to address the biopsychosocial theoretical framework: age (20 years to less than 45 years, 45 years to less than 60 years, and 60 years and above); sex (male, and female); race/ethnicity (Non-Hispanic white, Non- Hispanic black, Mexican American, and other); income to poverty ratio (less than 1.25, 1.25 to less than 2.00, 2.00 to less than 4.00, and 4.00 and above); education (less than High School, High School graduate, more than High School); marital status (married and not married); body mass index (less than 25, 25 to less than 30, 30 and above); insurance (yes and no); exercise (yes and no); and alcohol use (heavy, moderate, and none). Heavy alcohol use was defined as an average of more than 2 drinks a day on the days in which the participant drank, and moderate alcohol use was defined as an average of 1 or 2 drinks a day on the days in which the participant drank.
Statistical analysis
The data were analyzed with SAS 9.3® (Cary, NC). Variable frequencies were determined for the characteristics of the study participants. Bivariate associations of the serum cotinine levels and other important variables with chronic pain were conducted with Chi square analyses. Significant variables in the bivariate analyses were included in the logistic regression model development for the association of serum cotinine levels on chronic pain. Due to the complex study design of the NHANES data, considerations were made for the selected eligible sample, masked variance pseudo-stratum (SDMVSTRA), masked variance pseudo-primary sampling unit (SDMVPSU) and full sample 2 year Mobile Examination Center exam weight (WTMEC2YR) in the bivariate analyses and logistic regressions. The alpha for the analysis was established, a priori, as 0.05.
Results
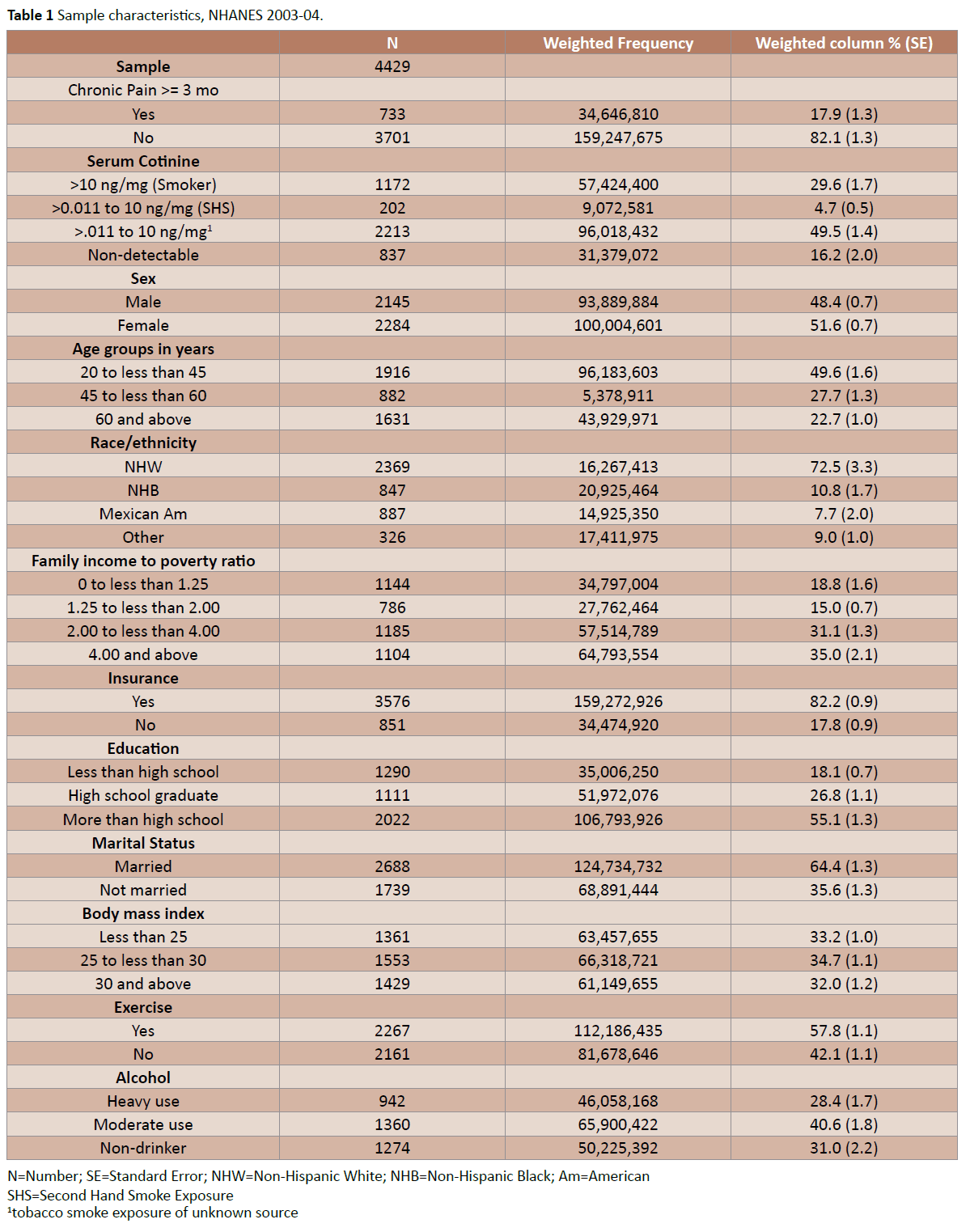
The sample had 17.9% (n=733) of participants reporting chronic pain and 29.6% (n=1172) of participants having serum cotinine levels >10 ng/mg. There were 51.6% (n=2284) females; 49.6% (n=1916) ages 20-45 years, and 55.1% (n=2022) who had more than a high school education. Most of the participants were non- Hispanic white (72.5%; n=2369); insured (82.2%; n=3576); and married (64.4%; n=2688). Details of the study characteristics are presented in Table 1.
N=Number; SE=Standard Error; NHW=Non-Hispanic White; NHB=Non-Hispanic Black; Am=American
SHS=Second Hand Smoke Exposure
1tobacco smoke exposure of unknown source.
Table 1: Sample characteristics, NHANES 2003-04.
N=Number; NHW= Non-Hispanic White; NHB= Non-Hispanic Black; Am=American
SHS=Secondhand Smoke Exposure
1tobacco smoke exposure of unknown source.
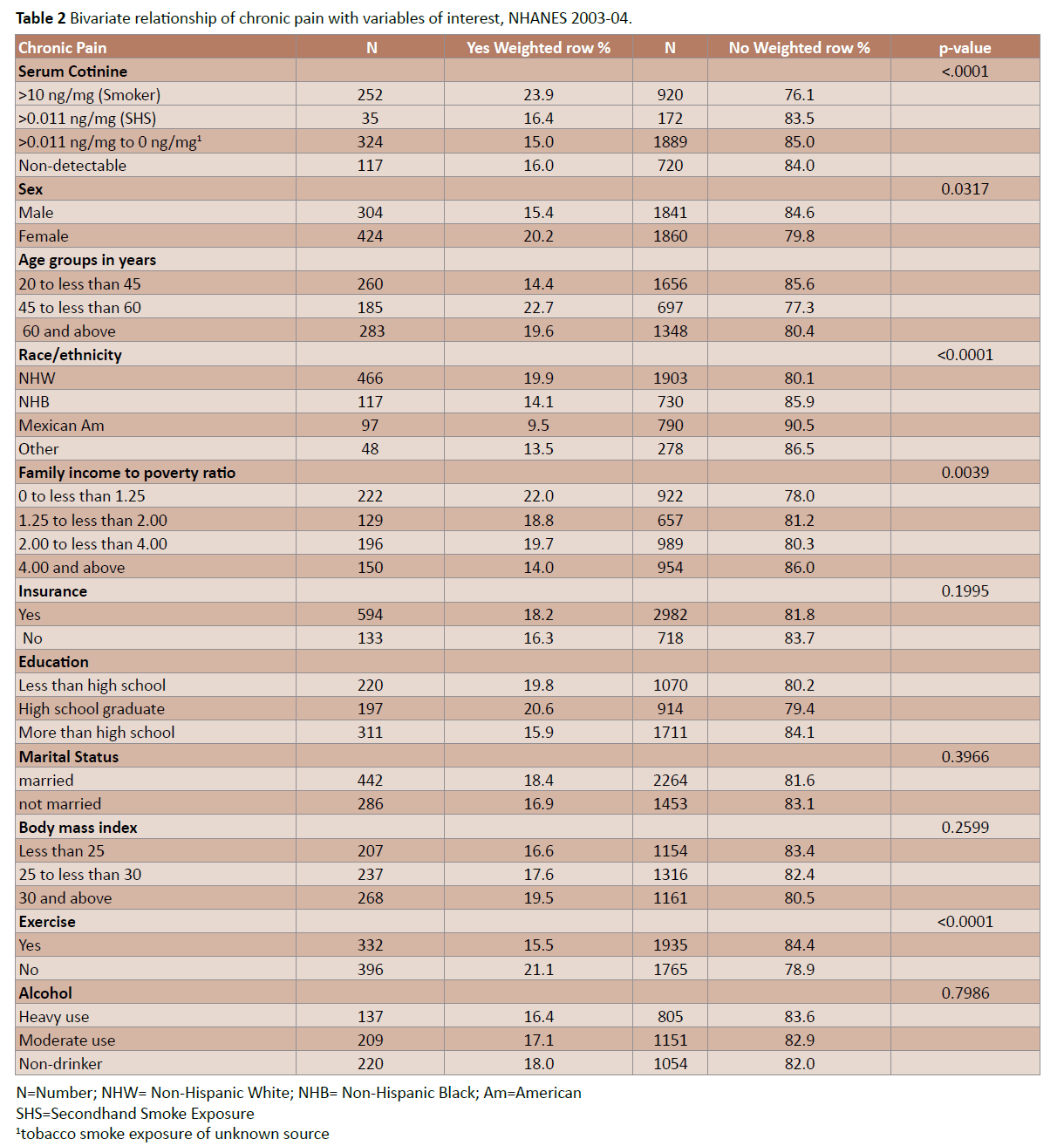
Table 2: Bivariate relationship of chronic pain with variables of interest, NHANES 2003-04.
Abbreviations: CI: Confidence Interval; ← less than; NHB: Non-Hispanic Black; NHW: Non-Hispanic White; Am: American; SHS: Second Hand Smoke Exposure. 1tobacco smoke exposure of unknown source.
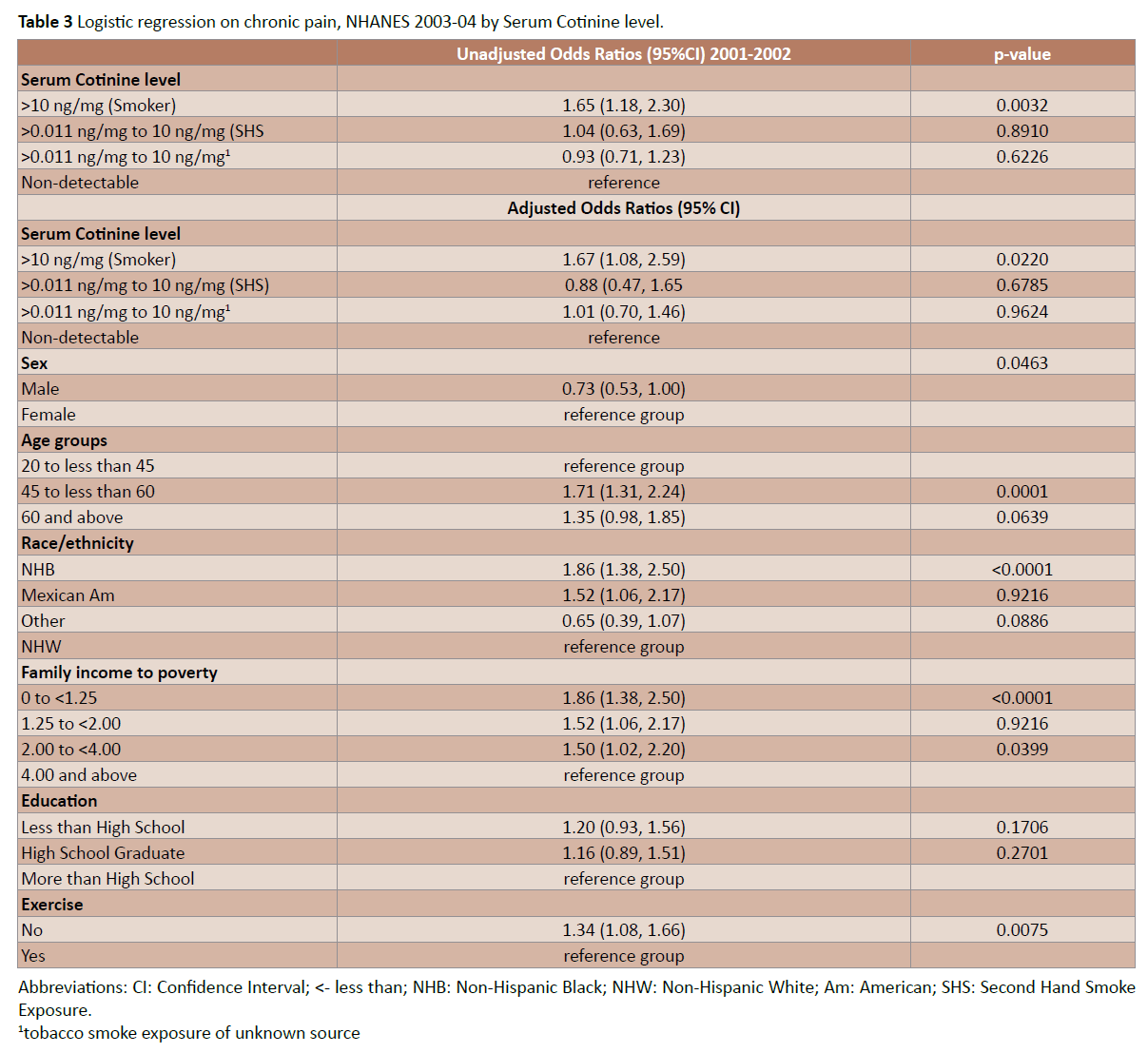
Table 3: Logistic regression on chronic pain, NHANES 2003-04 by Serum Cotinine level.
The results of the bivariate relationships with chronic pain are presented in Table 2. The key variable, tobacco smoke exposure (serum cotinine level), was significantly associated with chronic pain (p<0.0001). Other significant variables were sex, age, race/ ethnicity, family income to poverty ratio, education, and exercise. Marital status, body mass index, and alcohol use failed to reach significance.
The logistic regression models are presented in Table 3. The unadjusted odds ratio of tobacco smoke exposure (serum cotinine level) on chronic pain was 1.65 (95% CI: 1.18, 2.30; p=0.0032) for participants with a serum cotinine level >10 ng/mg (smokers) as compared with individuals who had a non-detectable serum cotinine level. For individuals with a serum cotinine level greater thand.011 ng/mg but less than or equal to 10 ng/mg who identified as living with someone who smoked in the home, the unadjusted odds ratio was 1.04 (95% CI: 0.63, 1.69; p=0.8910) as compared with individuals who had a non-detectable serum cotinine level. For individuals who reported that they did not live with someone who smoked in the home and who had a serum cotinine level greater than .011ng/mg but less than or equal to 10 ng/mg, the unadjusted odds ratio was 0.93 (95% CI: 0.71, 1.23; p=0.6226) as compared with individuals who had a nondetectable serum cotinine level.
The adjusted odds ratio of tobacco smoke exposure (serum cotinine level) on chronic pain was 1.67 (95% CI: 1.08, 2.59; p=0.0220) for participants with a serum cotinine level >10 ng/ mg (smokers) as compared with individuals who had a nondetectable serum cotinine level. For individuals with a serum cotinine level greater than.011 ng/mg but less than or equal to 10 ng/mg who identified as living with someone who smoked in the home, the adjusted odds ratio was 0.88 (95% CI: 0.47, 1.65; p=0.6785) as compared with individuals who had a nondetectable serum cotinine level. For individuals who reported that they did not live with someone who smoked in the home and who had a serum cotinine level greater than.011 ng/mg but less than or equal to 10 ng/mg, the adjusted odds ratio was 1.01 (95% CI: 0.70, 1.46; p=0.9624) as compared with individuals who had a non-detectable serum cotinine level.
Discussion
Research associated with nationally representative data concerning chronic pain is limited. The purpose of this study was to determine the relationship of chronic pain with smoking, SHS exposure and non-smoking using serum cotinine (and self-report of living with someone who smokes in the home) to identify the tobacco exposure groups. There were 17.9% of participants endorsing having chronic pain lasting 3 or more months. There were 29.6% of participants having serum cotinine levels greater than 10 ng/mg. The adjusted odds ratio for smokers as compared with non-smokers on chronic pain was 1.65 (95% CI: 1.18, 2.30; p=0.0032). Results did not reach significance for individuals with cotinine levels greater than.011 ng/mg but less than or equal to 10 ng/mg for chronic pain as compared with non-smokers. This study adds to the literature results indicating smoking, as defined with cotinine levels, is a risk factor for chronic pain.
Other studies
• Similar results for the association of chronic pain and tobacco smoke exposure were reported concerning a rural population in which current smoking was associated with chronic musculoskeletal pain (odds ratio 1.60; 95% CI: 1.04, 2.46) and chronic back pain (odds ratio 1.58; 95% CI: 1.13, 2.20) [13].
• In a U.S. nationally representative study, researchers found self-reported chronic pain and nicotine dependence (diagnosed using the World Health Organization Composite International Diagnostic Interview for trained non-clinicians) to be associated. Participants who endorsed current chronic neck or back pain were 2.30 (95% CI: 1.71, 3.11) times more likely to have current nicotine dependence than participants without current chronic neck or back pain [14].
• In a large, representative sample in Canada in which participants were asked about current cigarette use and pain lasting 6 months or longer, participants who had chronic back pain or arthritis were 1.54 (95% CI: 1.44, 1.65) times more likely to be daily cigarette smokers [15]. The results were adjusted for sociodemographic variables, mood disorders, and anxiety [15].
• In a large survey conducted in Britain, smokers had higher risk for regional pain lasting 24 hours or more in the past 12 months than non-smokers (prevalence ratio 1.3, 95% CI: 1.2, 1.4 for low back pain) [15,16].
Biological plausibility
From the late 1970’s, there was research on the effect of smoking on pain in which nicotine was shown to release endogenous opiates that relieve pain; additionally, dysphoric states such as pain were also determined to be cues to smoke by providing the situation (discriminative stimulus) for smoking reinforcement with beta-endorphin release [17]. Much of the research involved acute pain (cold water, pressure, etc.) [17]. Nicotine activates nicotinic acetylcholine receptors (nAChRs) throughout the central nervous system to release dopamine, noradrenaline, acetylcholine, glutamate and GABA [18]. Endogenous enkephalins and betaendorphins have roles in the rewarding effects of nicotine [18]. It is therefore biologically plausible that chronic pain is temporarily relieved by smoking, and the addiction cycle is strengthened in a feedback loop.
Strengths and limitations
The study does have limitations. It is a cross-sectional study, and by nature does not imply causality or temporality. Misclassification of people exposed to SHS was possible since the definition was dependent upon correct self-report of living with someone who smoked. Misclassification is also possible in that the blood sample may have been taken on a day in which a smoker had not smoked for several days. (The half-life of plasma cotinine is 15-20 hours) [19]. Additionally, the cut-point for cotinine is not firmly established in the literature. Researchers from Britain have suggested a cut-point of 12ng/ml as an overall cut-point for salivary cotinine levels [20].
A study strength is the use of the large representative NHANES sample which was publicly available from the CDC. The data collection, verification and representative study design of the original NHANES 2003-2004 also are strengths for this study. Additionally, cotinine, a biomarker for tobacco smoke exposure, was used to identify smokers. Its use has the potential to correctly identify individuals who smoke avoiding the social desirability bias that may be associated with a self-report. The large national nature of the study increases its potential for generalizability.
Conclusion
Chronic pain is a complex situation with many factors affecting it. Similarly smoking is a complex addiction. The interplay of chronic pain and smoking were significant in this study. Additional research is needed to understand the relationship more fully.
Acknowledgement
Research reported in this publication was supported by the National Institute Of General Medical Sciences of the National Institutes of Health under Award Number U54GM104942. The content is solely the responsibility of the author and does not necessarily represent the official views of the National Institutes of Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- Anon, CDC 2013 Biomonitoring Summary: Cotinine, CAS No. 486-56-6: Metabolite of nicotine (a component of tobacco smoke).
- Wong LS, Green HM, Feugate JE, Yadav M, Nothnagel EA, et al. (2004) Effects of “second-hand” smoke on structure and function of fibroblasts, cells that are critical for tissue repair and remodeling. BMC Cell Biology 5: 13.
- Talhout R, Schultz T, Florek E, van Benthem J, Wester P, et al. (2011) Hazardous Compounds in Tobacco Smoke. J Environ Res Public Health 8: 613-628.
- Anon BRFSS (2013)Nationwide (States, DC and Territories) Topic: Smoker Status.
- Anon CDC (2015) Fact Sheet-Fast Facts-Smoking and Tobacco Use.
- Ditre JW, Brandon TH, Zale EL, Meagher MM (2011) Pain, Nicotine, and Smoking: Research Findings and Mechanistic Considerations. Psychol Bull 137: 1065-1093.
- Wiengarten TN, Shi Y, Mantilla CB, Hooten WM, Warner DO (2011) Smoking and chronic pain: A real-but-puzzling relationship. Minn Med 94: 35-37.
- Turk DC, Monarch ES (2002) Biopsychosocial perspective on chronic pain. In: Denis C Turk, Robert J Gatchel (edr) Psychological Approaches to Pain Management, The Guilford Press, New York.
- Johannes CB, Le TK, Zhou X, Johnston JA, Dworkin RH (2010) The prevalence of chronic pain in United States adults: Results of an Internet-based survey. J Pain 11: 1230-1239.
- Gaskin DJ, Richard P (2012) The economic costs of pain in the United States. J Pain 13: 715-724.
- Riskowski JL (2014) Association of Socioeconomic Position and Pain Prevalence in the United States: Findings from the National Health and Nutrition Examination Survey. Pain Medicine 1: 1508-1521.
- Shargorodsky J, Garcia-Esquinas E, Navas-Acien A, Lin SY (2015) Allergic sensitization, rhinitis, and tobacco smoke exposure in U.S. children and adolescents. Int Forum Allergy Rhinol 5: 471-476.
- Andersson H, Ejlertsson G, Leden I (1998) Widespread musculoskeletal chronic pain associated with smoking. An epidemiological study in a general rural population, Scand J Rehabil Med 30: 185-191.
- Zvolensky MJ, McMillan K, Gonzalez A, Asmundson GJG (2009) Chronic pain and cigarette smoking and nicotine dependence among a representative sample of adults. Nicotine and Tobacco Research 11: 1407-1414.
- Zvolensky MJ, McMillan K, Gonzalez A, Asmundson GJG (2010) Chronic Musculoskeletal Pain and Cigarette Smoking among a Representative Sample of Canadian Adolescents and Adults. Addict Behav 35: 1008-1012.
- Palmer KT, Syddall H, Cooper C, Coggon D, (2003) Smoking and musculoskeletal disorders: Findings from a British national survey. Ann Rheum Dis 62: 33-36.
- Pomerleau OF, Turk DC, Fertig JB (1984) The Effects of Cigarette Smoking on Pain and Anxiety. Addictive Behaviors 9: 265-271.
- Berrendero F, Robledo P, Trigo JM, Martín-García E, Maldonado R (2010)Neurobiological mechanisms involved in nicotine dependence and reward: participation of the endogenous opioid system.NeurosciBiobehav Rev 35: 220-231.
- Anon NHANES (2003-2004)Data Documentation, Codebook, and Frequencies: Cotinine-Serum (L06COT_C).
- Jarvis MJ, Fidler J, Mindell J, Feyerabend C, West R (2008) Assessing smoking status in children, adolescents and adults: C otinine cut-points revisited. Addiction 103: 1553-1561.

