Yoshihiro Kikuchi1*, Tomoyuki Yoshikawa2, Takayoshi Asakawa1 and Masashi Takano2
1Ohki Memorial Kikuchi Cancer Center for Women, Japan
2Department of Clinical Oncology, National Defense Medical College Hospital, Japan
Corresponding Author:
Kikuchi Y
Ohki Memorial Kikuchi Cancer Center for Women, Japan
Tel: +81-4-2928-7311
E-mail: QWL04765@nifty.ne.jp
Received Date: December 21, 2018; Accepted Date: December 28, 2018; Published Date: January 04, 2019
Citation: Kikuchi Y, Yoshikawa T, Asakawa T, Takano M (2019) Serum IL-6 Can Be a Sentinel Biomarker for Sarcopenia and Cancer Cachexia. Biomark J. Vol.5 No.1: 3. doi:10.21767/2472-1646.100058
Copyright: © 2019 Kikuchi Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Editorial
Approximately 50%-80%of cancer patients have been reported to result in a devasting syndrome such as cancer cachexia (CC) and at least 20% patients reach the death [1]. Sarcopenia accompanying with muscle loss shows the most clinically relevant phenotypic feature of CC, such as asthenia, fatigue, impaired physiologic function, reduced tolerance to treatments, resulting in impaired quality of life and shorter survival. Such wasting syndromes as sarcopenia are shown in 20%-70% cases depending on the tumor type. Accordingly, reversion of CC and sarcopenia is of most importance and interest. In addition, high serum IL-6 has been reported to result in cancer metastases, invasion and resulting in CC [2,3]. Early detection of such sarcopenia syndromes is clinically most important. If sarcopenia can be precedently predicted, better treatment strategies will be possible. It is well-known that sarcopenia is accompanied by increased levels of inflammation factors TNF-alpha and IL-6 [4]. It has been reported that activation of the IL-6/STAT3 pathway also plays a causative role in the pathogenesis of cancer cachexia, one of the most distressing complications associated with the development of ovarian cancer [5]. Indeed, cachexia usually accompanies the development of ascites and chemoresistance in the most advanced stages of the disease [6]. The majority of advanced gynecologic cancer (GC) patients develop cachexia, which is a major contributor of morbidity and mortality in these patients. Cachexia is primarily responsible for body and muscle weight loss and correlates with tumor burden, increased proinflammatory cytokine levels, fatigue, and reduced response to chemotherapy and radio-therapy [7]. Patients presenting with advanced stage GC often show large tumor and ascites burden that, in turn, results into severe malnourishment because of decreased oral intake and compromised bowel functions. Despite its significant negative impact on quality of life, no effective treatment is currently available for GC-related cachexia. Indeed, muscle loss and low skeletal muscle attenuation are often detected in women undergoing primary debulking surgery for the treatment of GCs. Along the same line, recent evidence suggests that baseline sarcopenia represents one of the most accurate prognostic factors for survival in advanced GC and during chemotherapy treatment [8]. Clinically, we find out that elevation of serum IL-6 in patients with gynecologic cancers is varied by effect of the adjuvant chemotherapy.
Thus, we examined association between serum IL-6 and sarcopenia in patients with advanced GC. Measurement of serum IL-6 was assayed by the competitive inhibition of enzyme-linked immunosorbent assay [9]. Psoas muscle index (PMI) used CT was measured by methods of Prado et al. [10].
As shown in (Table 1), number of patients with more than 12.0 pg/ml serum IL-6 was 21 cases among of whom no patient had more than 6 (cm2/m2) PMI, while 66.7 % of patients with less than 5 PMI had more than 12.0 pg/ml serum IL-6. These results suggest that serum IL-6 could induce sarcopenia.
| |
serum IL-6 (pg/ml) |
|
|
| No. cases (<4.0) |
No. cases (4.0<,
<12.0) |
No. cases
(12.0<) |
PMI
(cm2/m2) |
|
|
|
| <5 |
9 (40.9%) |
3 (25.0%) |
14 (66.7%) |
| 5≤, ≤6 |
7 (31.8%) |
7 (31.8%) |
7 (58.3%) |
| 7 (33.3%) |
6 (27.5%) |
2 (16.7%) |
0 (0.0 %) |
| Total |
22 |
12 |
21 |
Table 1: Correlation between serum IL-6 and PMI in 56 patients with advanced gynecologic cancer.
In conclusion, smoking habit inducing inflammatory disease and less exercise cause elevation of serum IL-6 (TNF-alpha), resulting in sarcopenia and CC (Figure 1). Accordingly, serum IL-6 can be a sentinel biomarker in cancer sarcopenia and CC. Furthermore, it is possible that the treatments for targeting IL-6 signaling (or its downstream signaling) may contribute to and develop future immunotherapeutics [11-14].
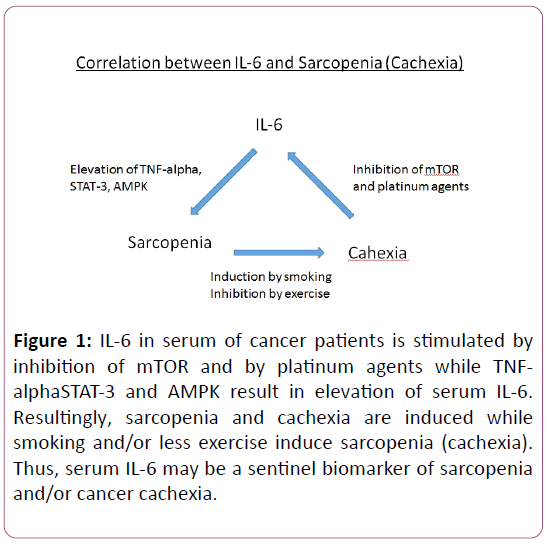
Figure 1: IL-6 in serum of cancer patients is stimulated by inhibition of mTOR and by platinum agents while TNFalphaSTAT-3 and AMPK result in elevation of serum IL-6. Resultingly, sarcopenia and cachexia are induced while smoking and/or less exercise induce sarcopenia (cachexia). Thus, serum IL-6 may be a sentinel biomarker of sarcopenia and/or cancer cachexia.
References
- Ryan AM, Power DG, Daly L, Cushen SJ (2016) Cancer-associated malnutrition, cachexia and sarcopenia: the skeleton in the hospital closet 40 years later. Proc Nutr Soc 75: 199-211.
- Beck JS, Chung C (1991) Serum interleukin-6 correlates with disease status in patents with epithelial ovarian cancer. Am J Obstete Gynecol 164: 1038-1043.
- Strassmann G, Jacob CO (1992) Mechanisms of experimental cancer cachexia. Interaction between mononuclear phagocytes and colon-adenocarcinoma and its relevance to IL-6 mediated cancer cachexia. J Immunol 148: 3674-3678.
- Nicolini A, Ferrari P, Masoni MC (2013) Malnutrition, anorexia and cachexia in cancer patients: a mini-review on pathogenesis and treatment. Biomed Pharmacother 67:807-817.
- Bonetto A, Ayggdu T, Jin X, Zhang Z, Zhan R, et al. (2012) JAK/STAT3 pathway inhibition blocks skeletal muscle wasting downstream of IL-6 and in experimental cancer cachexia. Am J Physiol Endocrinol Metab 303: E410-E421.
- Bronge H, Hederich P, Hapfelmeter A (2017) Sarcopenia in advanced serous ovarian cancer. International Journal of Gynecological Cancer: Official Journal of the Inter Gyn Cancer Soc 27: 223-232.
- Maccio A, Madeddu C (2012) Inflammation and ovarian cancer. Cytokine 58: 133-147.
- Kumar A, Moynaghi MR, Multinu F (2016) Muscle composition measured by CT scan is a measurable predictor of overall survival in advanced ovarian cancer. Gyn Onco 142: 311-316.
- Bian AL, Hu HY, Rong YD, Wang J, Wang JX, et.al. (2017) A study on relationship between elderly sarcopenia and inflammatory factors IL-6 and TNF-alpha. Eur J Med Res 22: 25-37.
- Bian AL, Hu HY, Rong YD, Wang J, Wang JX, et.al. (2017) A study on relationship between elderly sarcopenia and inflammatory factors IL-6 and TNF-alpha. Eur J Med Res 22: 25-37.
- Blum D, Omlin A, Barcus VE (2011) Cancer cachexia: A systematic literature review of items and domains associated with involuntary weight loss in cancer. Crit Rev Onco/ Hematol 80:114-144.
- Hess LM, Barakat R, Tien C (2007) Weight change during chemotherapy as a potential prognostic factor for stage III epithelial ovarian carcinoma: a gynecologic oncology group study. Gynecol Oncol 107: 260-265.
- Antoun S, Borget I, Lanoy E (2013) Impact of sarcopenia on the prognosis and treatment toxicities in patients diagnosed with cancer. Curr Opin Support Palliat Care 7: 383-389.
- Fearon KC, Strasser F, Anker SD (2011) Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 12: 489-495.

