Keywords
Cytokines; Heart/ physiopathology; Pancreatitis/ physiopathology
INTRODUCTION
Acute pancreatitis (AP) is characterized by a local inflammation of the pancreas which may lead to a systemic response and progress to a multiple organ dysfunction syndrome (MODS), with high morbidity and mortality [1, 2].
Several mechanisms are involved in the development of the local and systemic response in AP as complement activation, activation of neutrophils and macrophages, trelease of inflammatory cytokines (TNF-α, IL-1β, IL- 6, IL-10 and TGF-β), chemokines, arachidonic acid metabolites (prostaglandins, platelet-activating factor and leukotrienes), proteolytic and lipolytic enzymes, as well as reactive oxygen species [3, 4]. The systemic lesions can result in respiratory, cardiovascular, renal, and immunological disorders similar to those seen in sepsis and severe trauma [5].
Cardiovascular system may be affected throughout the clinical course of AP with cardiac rhythm and contractility and vasomotor tone of peripheral vessels. The cardiac alterations could be explained by vasoactive peptides modulation and myocardial depressant factor [6, 7].
A few experimental studies that myocardial ultrastructural alterations including interstitial edema, hypertrophy and hypoxia of cardiac muscle cells, increase in muscle fiber contractile function and collagen deposit in myocardial stroma in AP [8, 9].
The aim of this study was to evaluate local myocardial cytokine production, as well as, functional and histological myocardial alterations in severe acute pancreatitis in rats.
MATERIAL AND METHODS
Experimental Protocol
The animals were divided into three main groups:
Group 1 (n=6): control; Group 2 (n=6): sham (2h after laparotomy without induction of AP); Group 3 (n=24): AP (sub-groups 2h, 12h and, 24h and 15 days)
Animals
Adult male Wistar rats (230 ± 30 g) were housed in individual cages in a 12-hour dark light-controlled environment with free access to standard rat chow diet and water. The experimental protocol was approved by the Ethics Committee for Animal Research from the Medical School of São Paulo University and received humane care according to the criteria outlined in the Guide for the Care and Use of Laboratory Animals, prepared by the National Academy of Sciences.
Induction of AP
Adult male Wistar rats were anesthetized with ketamine chloride (Ketalar, Park-Davis, São Paulo, Brazil), and a laparotomy was performed. Acute pancreatitis was induced by retrograde injection of 0. 5 mL of 4% sodium taurocholate (Sigma-Aldrich, St. Louis, MO, USA) transduodenally into the biliopancreatic duct at a constant infusion rate [10]. A clamp was applied across the proximal hepatic duct during the injection. After operation, animals were returned to their cages with free access to food and water. The rats were killed by exsanguination at predefined time points (2, 12, 24 hrs. , and 15 days).
Biochemical Analysis
Plasma amylase levels were determined spectrophotometrically, whereas TNF-α, IL-6 and IL-10 were quantified in accordance with the manufacturer’s instructions and guidelines using enzyme-linked immunosorbent assay (ELISA) kits (Biosource International CytoscreenTM, Nivelles, Belgium).
Cytokine mRNA Expression Analysis
Myocardial tissue was removed, snap frozen, and stored in liquid nitrogen. Total myocardial RNA was extracted using TRIzol reagent (Invitrogen, Life Technologies, Gaithersburg, USA) according manufacturer’s instructions. RNA integrity was assessed by analysis of 28S/18S rRNA ratios using a NanoDrop™ ND-1000 spectrophotometer (NanoDrop Technologies, Inc. Wilmington, EUA). RNA quality assessment was analyzed by agarose gel electrophoresis. Ratios equal to or greater than 1. 8 were considered satisfactory. Samples were kept at –80 °C until processing by qRT-PCR.
Quantitative RT-PCR Analysis
qRT-PCR analysis for TGF-β1, TNF-α, and IL-6 genes were performed in a RotorGene RG3000 thermal cycler (Corbett Research, Sidney, Australia) using a SuperScriptTM III Platinum SYBR Green One-Step qRT-PCR kit (Invitrogen, Life Technologies) according to the manufacturer’s recommendations. Amplification of specific transcripts was confirmed by melting curve profiles at the end of each PCR cycle. The following specific primers were used: IL-6 sense 5’CTTCACAAGTCGGAGGCTTAAT3’ and antisense 5’ACAGTGCATCATCGCTGTTC3’; TGF-β1 sense 5’CGGCAGCTGTACATTGACTT3’ and antisense 5’AGCGCACGATCATGTTGGAC3’; TNF-α sense 5’GCTTGGTGGTTTGCTACGAC3’ and antisense 5’TGCCTCAGCCTCTTCTCATT3’; β-actin sense 5’TGTCACCAACTGGGACGATA3’ and β-actin antisense 5’GGGGTGTTGAAGGTCTCAAA3’. Relative abundance of transcripts were calculated according to the ΔΔCt method, which reflects the differences in the threshold for each target gene relative to the housekeeping gene β-actin and expression in control myocardial tissue sample [11].
Echocardiographic Assessment of Cardiac Function
Rats were anesthetized with ketamine (50 mg/kg) and xylazine (10 mg/kg) and a transthoracic echocardiography of the left ventricle was performed using a 13-MHz linear array transducer (15L8) interfaced with a Sequoia 512 system (Acuson, Mountain View, CA, U. S. A. ) as previously described [12]. The following parameters were evaluated: left ventricular end diastolic diameter (LVEDD), left ventricular end systolic diameter (LVESD), fractional shortening (FS), ejection fraction (EF), isovolumetric relaxation time corrected by heart rate (IVRT), and myocardial performance index (MPI). All measurements were obtained according to the American Society of Echocardiography recommendations by the same experienced observer.
Histological Examination of Myocardial Tissue
Heart tissue samples were excised and fixed in 10% neutral buffered formalin for standard hematoxylineosin staining. Histological evaluation of myocardial sections was performed by a pathologist in a blinded way. Histopathological examination involved the evaluation of the following parameters: coagulation necrosis, vacuolar degeneration, edema, picnosis, and loss of nucleus, and lymphocytes surrounding necrotic cardiac fibers (spot necrosis). The intensity of cardiac damage was evaluated according to a scoring system that ranged from absence to severe lesions (0: absent, 1: mild, 2: moderate, and 3: severe).
STATISTICS
Data are expressed as mean ± standard deviation (SD). The multivariate ANOVA (fixed factor) was used to determine the overall difference between the independent groups for echocardiography results and Tukey and Dunnett tests for multiple comparisons (amylase levels, and IL-6, TGF-β and TNF-α mRNA levels). The Kruskal-Wallis test was used for comparison between groups for serum cytokines levels and histological analysis. A value of p<0. 05 was considered significant. Statistical analysis was carried out using SPSS software version 19. 0 and R-Program version 2. 11. 1.
RESULTS
Serum Amylase and Inflammatory Mediator Levels
The serum amylase levels were significant higher in AP 2h group in comparison with the other groups (p=0. 006) as well as the serum levels of TNF-α and IL-10 (p=0. 015). The plasma levels of cytokines (TNF-α, IL-6 and IL-10) were below the detection limits in control, sham, 24h and 15d (Table 1).

Inflammatory Cytokines Expression
• The mRNA IL-6 levels from group AP 2h were statistically higher in comparison with the other groups (Figure 1A).
• The mRNA TGF-β levels from group AP 12h were statistically higher in comparison with the other groups (Figure 1B).
• The mRNA TNF-α levels from sham group and AP 2h were statistically lower when compared to AP 12h (p=0. 022; p=0. 008) and AP 24h groups (p=0. 008; p=0. 008) (Figure 1C).
Figure 1. Expression of A. mRNA IL-6, B. TGF-β C. TNF-α in myocardial tissue.
Cardiac Function
No significant changes in heart rate neither fractional shortening were observed (p=0. 971 and p=0. 81, respectively). Significant changes in the LVEDD and LVESD were found in AP 2h and AP 12h groups (p<0. 001 and p=0. 012, respectively). There were no differences between groups for the following parameters: EF(%), IVRT, and MPI (p=0. 778; p=0. 248; and p=0. 251, respectively) (Table 2 and Figure 2).
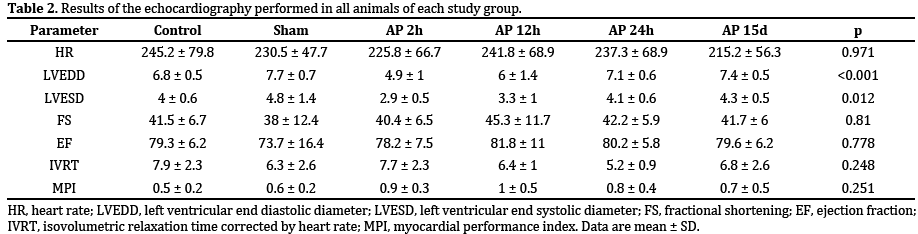
Figure 2. Boxplot of A. LVESD and B. LVEDD.
Histological Analysis of Cardiac Tissue
No significant difference was observed between coagulation necrosis, edema, and spot necrosis (p= 0. 099, p= 0. 207, and p= 0. 191, respectively) between all groups. There were statistical changes for vacuolar degeneration in AP 15d group (p=0. 048), picnosis and loss of nucleus in AP 2h group (p=0. 034), and lymphocytes in AP 12h group (p=0. 001) (Figure 3).
Figure 3. Histological results of cardiac tissue in AP 12h group. A. Cardiac fibers showed diffuse vacuolar degeneration. B. A few fibers were necrotic and
surrounded by lymphocytes and macrophages (spot necrosis) (HE - 400x).
DISCUSSION
The aim of this study was to investigate the myocardial cytokines production and its impairment in an experimental model of severe acute pancreatitis in rats.
We determined the circulating levels of cytokines, since they play an important role not only in the local inflammatory response as well as in systemic, such as the pro-inflammatory cytokine TNF-α, one of the modulators in circulatory collapse found in severe sepsis correlated with a worse prognosis [13].
We detected elevated serum levels of IL-6, IL-10 and TNF-α 2h after AP induction and not detected in AP 24h and 15 days groups. The differences in the response patterns of TNF-α and IL-6 after acute physiological stimuli may be related to the different release times and cross-regulation of these cytokines. Specifically, TNF-α appears at the beginning, followed by secretion of IL-6 and this causes suppressive effect on the expression of TNF-α [14]. In this context, after AP 12h we observed an increase in serum IL-6 levels and a decrease in TNF-α level (Table 1).
The serum levels of the anti-inflammatory cytokine IL- 10 maintains correlation with serum levels of TNF-α and IL-6 as observed in previous study [3]. Norman et al. [4] showed variable association of IL-10 with tissue injury and severity of AP, demonstrating that may be used as a predictor of severity. However, in another study, Dumont et al. showed conflicting results [15].
Hemodynamic changes related to AP occur in SAP, even without documented sepsis. Di Carlo et al. [16] observed that patients with SAP showed myocardial depression due to decreased left ventricular output similar to findings in other septic patients [2, 17].
The difficulty of performing experimental and clinical hemodynamic studies in SAP justifies the few published articles. However, in recent years, it has been demonstrated the role of transthoracic echocardiography, as minimally invasive method, to evaluate the morphology and function and left ventricular cardiac output determination or ventricular mass [18].
In this study, the echocardiographic findings regarding heart rate (HR) were similar between the groups showing the possibility of comparing the other results. The relative wall thickness (RWT), the interventricular septum (IVS) and posterior wall (PW), showed no significant difference, suggesting the absence of hypertrophy and / or myocardial ischemia (Table 2), although high concentrations of circulating IL-6 was associated with increased risk of coronary heart disease in prospective studies [19, 20].
The Fractional Shortening (FS) and the Ejection Fraction (FE) did not change significantly showing the stability of myocardial systolic function. The fact that the FS is normal does not mean, necessarily, that myocardial contractility is unchanged, because we did not make invasive measurements.
Likewise, the preservation of diastolic function demonstrated by the variable isovolumetric relaxation time (IVRT) and the relationship between early to late diastolic filling velocity (E/A), remained unchanged between groups. The myocardial performance index (MPI) did not change over time, demonstrating the preservation of global myocardial function.
Moreover, we found Decreased Diastolic (DD) and systolic (SD) diameters of the left ventricle (LV) that may be related to hypovolemia secondary to the intense inflammatory process caused by SAP (Figure 2).
According to Flierl et al. [21], cardiac dysfunction, wellrecognized complication of severe sepsis is characterized by ventricular dilatation, reduced ejection fraction and reduced contractility. Although cardiac alterations in SAP and sepsis may be related to, at the present study the echocardiographic measurements were markedly altered in group 2h and, at this time, no sepsis were present.
Circulating blood factors are involved in the progression of myocardial changes induced by septic shock, and the cellular and molecular events of myocardial tissue itself are targets of researchers in search for better understanding this process [22] In the experimental model applied significant increase in serum levels of interleukins group 2h, and consequently the myocardium may also respond by increasing or decreasing levels of mRNA of inflammatory factors.
Flores-Arredondo et al. [23] showed an increase in intracardiac pro-inflammatory cytokines production and decreased expression of anti-inflammatory cytokines, in particular, the IL-10 cytokine. These findings were associated with increased hypertrophy and fibrosis and decreased left ventricular ejection fraction.
In an experimental study of diabetes in mice was found an increased expression of TNF-α in myocardial tissue associated with induction of cell death through cardiac oxidative stress [24] Plenz et al. [25], studying advanced heart failure, found a close correlation between elevated IL-6 serum levels and acute cardiac dysfunction and could play an important role in the pathophysiology [23].
The gene expression of IL-6 was increased in group AP 2h in comparison to the other groups (Figure 1A). Apparently the cardiac tissue has the first reaction in the presence of SAP, the endogenous production of IL-6 that can be related to the functional and not histological.
The result of gene expression of TGF-β in our study demonstrates a late onset (AP 12 h) that may be related to cardiac changes after an inflammatory stimulus (Figure 1B). Increased expression of TGF-β was found in an experimental model of cardiac hypertrophy in rats with suprarenal aortic constriction. The detection of TGF-β in the interstitium, especially in places where fibroblasts demonstrate proliferative activity, is associated with the induction of collagen I and III and myocardial fibrosis [26].
Kuwahara et al. [27] observed that TGF-β plays a key role in myocardial fibrosis in rat hypertensive hearts through activation of fibroblast. These findings were also exemplified by other studies [25].
We found increased expression of TNF-α in groups 24h and 15 days compared to sham and AP 2h groups (Figure 1C). The late appearance of TNF-α may be related to histological features associated with cardiac cell death [28].
Experimental studies demonstrate a close correlation between structural changes and myocardial severe systemic inflammatory response, such as interstitial and mitochondrial edema and myocardial necrosis [29]. On the other hand, a decrease in myocardial contractility in the presence of sepsis was also found, even in the absence of tissue injury [30].
Rossi et al. [31], found increased expression of TNF-α and nonspecific myocardial changes such as slightly hypertrophied cardiomyocytes, mild to moderate interstitial edema, mild interstitial fibrosis and increased number of macrophage [32]. The elevated number of macrophages in association with expression of TNF-α can promote reduction of cardiac function in septic hearts.
In histological analysis, we found significant heart changes as vacuolar degeneration, picnosis and loss of nuclei and lymphocytes, which may be related to the inflammatory phenomena triggered by SAP (Figure 3A and 3B). These changes are mantained in histological studies and 15 days appear to be related to the increased expression of TNF-α, however, with no hemodynamic changes in echocardiography.
In summary, in the present study we showed that in the experimental SAP model utilized, the myocardium produces cytokines locally, whereas IL-6 production is an early event and could be correlated with the same period of echocardiographic left ventricular change. The production of TNF-alpha occurs in the same period of histological findings, whereas TGF-beta in the subsequent period.
CONCLUSION
We found cardiac and histological changes compatible with the inflammatory process triggered by SAP with the promotion of local myocardial cytokine production.
Acknowledgment
The authors thank Mrs. Sandra Nassa Sampietre for her expert technical assistance.
This research was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil.
Conflict of Interest
The authors declare that there is no conflict of interest that would prejudice the impartiality of this scientific work.
References
- Talukdar R, SwaroopVege S. Early management of severe acute pancreatitis. Curr Gastroenterol Rep. 2011; 13(2):123-30. [PMID: 21243452]
- Wu BU. Prognosis in acute pancreatitis. CMAJ. 2011; 183(6):673-7. [PMID: 21422134]
- Makhija R, Kingsnorth AN. Cytokine storm in acute pancreatitis. J Hepatobiliary Pancreat Surg. 2002; 9:401-10. [PMID: 12483260]
- Norman J. The role of cytokines in the pathogenesis of acute pancreatitis. Am J Surg. 1998; 175(1):76-83. [PMID: 9445247]
- Campos T, Deree J, Coimbra R. From acute pancreatitis to end-organ injury: mechanisms of acute lung injury. Surg Infect. 2007; 8(1):107-20. [PMID: 17381402]
- Yegneswaran B, Kostis JB, Pitchumoni CS. Cardiovascular manifestations of acute pancreatitis. J Crit Care. 2011; 26(2):225. [PMID: 21185146]
- Greer SE, BurchardK W. Acute pancreatitis and critical illness: a pancreatic tale of hypoperfusion and inflammation. Chest. 2009; 136(5):1413-9. [PMID: 19892682]
- Kanaian AS, Permiakov NK, Khandanian RK, Gevorkian GA. Combined pathology of the pancreas and myocardium in myocardial infarction and acute destructive pancreatitis. Arkh Patol. 1996; 58(5):56-61. [PMID: 9005827]
- Saulea A, Costin S, Rotari V. Heart ultrastructure in experimental acute pancreatitis. Rom J Physiol. 1997; 34(1-4):35-44. [PMID: 9653808]
- Lankisch PG, Koop H, Winckler K, Fölsch UR, Creutzfeldt W. Somatostatin therapy of acute experimental pancreatitis. Gut. 1977; 18(9):713-6. [PMID: 604191]
- Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2 (-Delta DeltaC(T)) method. Methods. 2001; 25:402-8. [PMID: 11846609]
- Salemi VM, Pires MD, Cestari IN, Cestari IA, Picard MH, Leirner AA et al. Echocardiographic assessment of global ventricular function using the myocardial performance index in rats with hypertrophy. Artif Organs. 2004; 28:332-7. [PMID: 15084191]
- Granger J, Remick D. Acute pancreatitis: models, markers and mediators. Shock. 2005; 24:45-51. [PMID: 16374372]
- Steptoe A, Hamer M, Chida Y. The effects of acute psychological stress on circulating inflammatory factors in humans: a review and meta-analysis. Brain Behav Immun. 2007; 21(7):901-12. [PMID: 17475444]
- Dumot JA, Conwell DL, Zuccaro G Jr, Vargo JJ, Shay SS, Easley KA et al. A randomized, double blind study of interleukin 10 for the prevention of ERCP-induced pancreatitis. Am J Gastroenterol. 2001; 96(7):2098-102. [PMID: 11467638]
- Di Carlo V, Nespoli A, Chiesa R, Staudacher C, Cristallo M, Bevilacqua G et al. Hemodynamic and metabolic impairment in acute pancreatitis. World J Surg. 1981; 5(3):329-39. [PMID: 7293195]
- Ito K, Ramirez-Schon G, Shah PM, Agarwal N, Delguercio LR, Reynolds BM. Myocardial function in acute pancreatitis. Ann Surg. 1981; 194:85-8. [PMID: 7247538]
- Burrell LM, Chan R, Phillips PA, Calafiore P, Tonkin AM, Johnston CI. Validation of an echocardiographic assessment of cardiac function following moderate size myocardial infarction in the rat. Clin Exp Pharmacol Physiol. 1996; 23(6-7):570-2. [PMID: 8800587]
- Ridker PM, Rifai N, Stampfer MJ, Hennekens CH. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation. 2000; 101:1767–72. [PMID: 10769275]
- Danesh J, Kaptoge S, Mann AG, Sarwar N, Wood A, Angleman SB et al. Long-term interleukin-6 levels and subsequent risk of coronary heart disease: two new prospective studies and a systematic review. PLoS Med. 2008; 5(4):78. [PMID: 18399716]
- Flierl MA, Rittirsch D, Huber-Lang MS, Sarma JV, Ward PA. Molecular events in the cardiomyopathy of sepsis. Mol Med. 2008; 14(5-6):327-36. [PMID: 18256728]
- Flynn A, Chokkalingam Mani B, Mather PJ. Sepsis-induced cardiomyopathy: a review of pathophysiologic mechanisms. Heart Fail Rev. 2010; 15(6):605-11. [PMID: 20571889]
- Flores-Arredondo JH, García-Rivas G, Torre-Amione G. Immune Modulation in Heart Failure: Past Challenges and Future Hopes. Curr Heart Fail Rep. 2011; 8:28-37. [PMID: 21221862]
- Zhang C, Jin S, Guo W, Li C, Li X, Rane MJ et al. Attenuation of diabetes-induced cardiac inflammation and pathological remodeling by low-dose radiation. Radiat Res. 2011; 175(3):307-21. [PMID: 21388274]
- Plenz G, Eschert H, Erren M, Wichter T, Böhm M, Flesch M et al. The interleukin-6/interleukin-6-receptor system is activated in donor hearts. J Am Coll Cardiol. 2002; 39(9):1508-12. [PMID: 11985915]
- Kai H, Kuwahara F, Tokuda K, Imaizumi T. Diastolic dysfunction in hypertensive hearts: roles of perivascular inflammation and reactive myocardial fibrosis. Hypertens Res. 2005; 28(6):483-90. [PMID: 16231753]
- Kuwahara F, Kai H, Tokuda K, Kai M, Takeshita A, Egashira K et al. Transforming growth factor-beta function blocking prevents myocardial fibrosis and diastolic dysfunction in pressure-overloaded rats. Circulation. 2002; 106(1):130-5. [PMID: 12093782]
- Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braunwald E. Elevation of tumor necrosis factor-alpha and increased risk of recurrent coronary events after myocardial infarction. Circulation. 2000; 101(18):2149-53. [PMID: 10801754]
- Solomon MA, Correa R, Alexander HR, Koev LA, Cobb JP, Kim DK et al. Myocardial energy metabolism and morphology in a canine model of sepsis. Am J Physiol. 1994; 266(2):757-68. [PMID: 8141377]
- Zhou M, Wang P, Chaudry IH. Cardiac contractility and structure are not significantly compromised even during the late, hypodynamic stage of sepsis. Shock. 1998; 9(5):352-8. [PMID: 9617885]
- Rossi MA, Celes MR, Prado CM, Saggioro FP. Myocardial structural changes in long-term human severe sepsis/septic shock may be responsible for cardiac dysfunction. Shock. 2007; 27(1):10-8. [PMID: 17172974]
- Azzawi M, Kan SW, Hillier V, Yonan N, Hutchinson IV, Hasleton PS. The distribution of cardiac macrophages in myocardial ischaemia and cardiomyopathy. Histopathology. 2005; 46(3):314-9. [PMID: 15720417]




