Keywords
Mobility Limitation; Muscle Weakness; Pancreas; Phosphorus; Vitamin D Deficiency
INTRODUCTION
Skeletal muscle weakness is a major health problem [1] and as many as 40% of individuals over 60 years of age may be affected [1]. The people affected are at high risk of falling and immobilization, which may lead to bone fractures, infection and death. Indeed, low gait speed and poor balance have been found to be associated with high mortality [2]. Thus, skeletal muscle weakness has a high impact on the quality of life of the affected individual and on health expenditures in the community.
Skeletal muscle weakness is a major feature of several conditions. These include primary muscle diseases, such as muscular dystrophy, or endocrine diseases, such as hypothyroidism, but also sarcopenia, the agerelated decline of muscle. Several neurological disorders (e.g. Guillain Barre) or amyotrophic lateral sclerosis give rise to muscle weakness. Peripheral artery disease is a common manifestation of systemic arteriosclerosis, which can present itself as skeletal muscle weakness and reduced walking distance in the form of intermittent claudication. Exocrine pancreatic insufficiency is also associated with low vitamin D levels, which is known to cause muscle weakness [3].
Identification of the modifiable causes of skeletal muscle weakness should have a high priority as this will lead to better treatment of patients. We present the case of a patient showing a slow decrease in ability to walk associated with low vitamin D and mineral levels due to pancreatic insufficiency which improved as the deficiencies were corrected.
CASE REPORT
A 62-year-old Caucasian male who was living by himself contacted the outpatient clinic due to severely reduced capacity of walking distances over the past 6 months. Quality of life was severely hampered and he had recently put his house up for sale, as he was no longer able to ascend the stairs to the first floor. Over approximately the same time period, there had been a 10 kg weight loss.
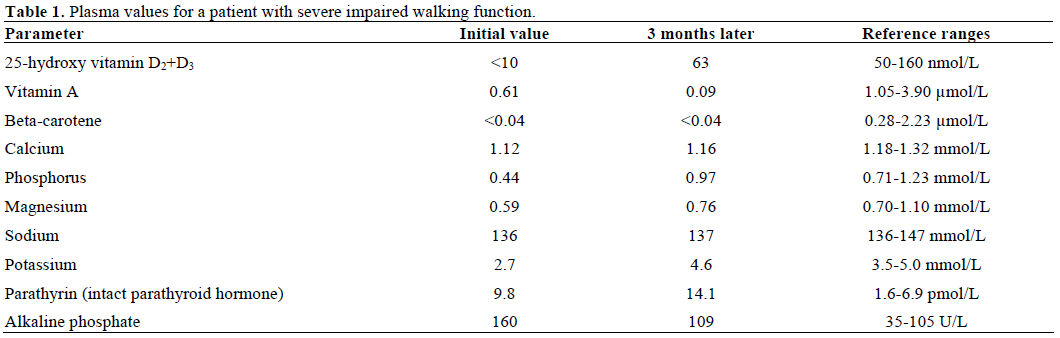
Peripheral arterial disease was suspected. Therefore, a walking test combined with measurement of the blood pressure in the toes, ankle and brachia, including the ankle-brachial index, was carried out and all blood parameters were found to be normal. However, the walking test confirmed that the patient had a severely impaired capacity of walking distances, which was less than 100 m. For the previous year, the patient had been taking calcium with vitamin D 400 mg/400 IU bid. Despite this, the laboratory findings showed severe vitamin D and calcium deficiency as well as low levels of vitamin A, phosphorus, magnesium and potassium (Table 1). Stool elastase was found to be less than 50 μg/g of stool (reference: greater than 200 μg/g of Peripheral arterial disease was suspected. Therefore, a walking test combined with measurement of the blood pressure in the toes, ankle and brachia, including the ankle-brachial index, was carried out and all blood parameters were found to be normal. However, the walking test confirmed that the patient had a severely impaired capacity of walking distances, which was less than 100 m. For the previous year, the patient had been taking calcium with vitamin D 400 mg/400 IU bid. Despite this, the laboratory findings showed severe vitamin D and calcium deficiency as well as low levels of vitamin A, phosphorus, magnesium and potassium (Table 1). Stool elastase was found to be less than 50 μg/g of stool (reference: greater than 200 μg/g of stool), suggesting exocrine pancreatic insufficiency as the cause of the hypovitaminosis and weight loss.
Peroral therapy with pancreatic enzymes (Creon®, Solvay Pharma, Herlev, Denmark) 40,000 IU for regular meals, vitamin A 50,000 IU od for 5 days followed by 50,000 IU weekly, magnesium 360 mg tid, zinc 100 mg tid and monthly i.m. injections of 300,000 IU ergocalciferol were initiated. However, after one month, the patient was admitted to the gastroenterological ward as a result of electrolyte deficiency and was treated with intravenous infusions of phosphorous and magnesium. On several occasions, he was asked to indicate his diet and medication in detail. The diet was considered to be a “normal diet” in regards to energy and nutrition content, his knowledge on how and when to take his medication (especially the pancreatic enzymes) was good and he said that there were no compliance issues. The intramuscular injections of ergocalciferol continued and the treatment with pancreatic enzymes was increased to 80,000 IU for regular meals and 40,000 IU for snacks.
Two months later, the vitamin D, phosphorous and magnesium values were normalized whereas vitamin A deficiency persisted, and calcium and parathyroid hormone values remained suboptimal. (Figure 1, Table 1). Body weight and walking distance gradually increased to near normal with a walking distance of 1,500-3,000 m.
Figure 1. Plasma values of 25-hydroxy vitamin D2+D3 for a patient
with severe impaired walking function due to pancreatic
insufficiency. The initial plasma 25-hydroxy vitamin D2+D3 value
was found to be less than 10 nmol/L. Treatment with monthly i.m.
injections of 300,000 IU of ergocalciferol was initiated at day 15.
Levels steadily rose and were found to be within the reference levels
at day 79.
DISCUSSION
We report the case of a patient with severe impaired waling function due to low vitamin D and mineral levels where walking distance improved upon treatment of the deficiencies. Although several treatments were initiated simultaneously, correction of the vitamin D deficiency was credited with the improvement in walking distance. In muscle cells, the action of vitamin D on its receptor promotes protein synthesis, uptake of inorganic phosphate and helps to regulate intracellular calcium concentrations. This affects a broad spectrum of chemical processes (e.g. the production of energy rich compounds, such as ATP), and the process of muscle contraction [4]. Vitamin D deficiency primarily causes atrophy of the type-2 muscle fibers [4], which are fast contracting and produce high power, and, as a result of this, can result in muscle weakness and impaired deambulation.
The main reason for the deficiencies in our case was found to be pancreatic insufficiency. Thus, fecal elastase was found to be less than 50 μg/g of stool (reference: greater than 200 μg/g of stool) which is considered diagnostic for exocrine pancreatic insufficiency. Low levels of vitamin D have previously been found in subjects with chronic pancreatitis and low fecal elastase [5]. An unbalanced diet could contribute to the hypovitaminosis; however, the diet reported by the patient was found to be sufficient.
Despite taking peroral calcium and vitamin D for the previous year, the patient had developed a severe vitamin D deficiency. Once i.m. injections of ergocalciferol were initiated, there was a steady increase in vitamin D. This is in accordance with a recent Cochrane review on vitamin D supplementation in children with exocrine pancreatic insufficiency due to cystic fibrosis, which concluded that there was no significant effect of peroral vitamin D treatment [6]. This may be in contrast to treatment of other patient groups. For example, vitamin D supplementation in the elderly has been well studied [7, 8, 9], and peroral treatment was found to be effective concerning the reduction in the number of falls as compared to the placebo group [10].
To our knowledge, no comparative studies exist on the use of parenteral or peroral vitamin D in patients with pancreatic insufficiency. Thus, clinicians have to rely on empirical knowledge when deciding for a peroral or parenteral regime, depending on the case at hand.
In our case, peroral treatment with pancreatic enzymes and minerals did not initially normalize the phosphorous and magnesium insufficiencies. Noncompliance was not suspected as the patient could account for his medication in detail. Only after the patient had received parenteral therapy with phosphorous and magnesium, and an increase in pancreatic enzyme therapy did the levels become acceptable. A study by Schubert et al. suggests that it is not the vitamin D deficiency per se but the simultaneous phosphorus deficiency, which causes the observed muscle weakness [11]. In our case, the patient’s walking distance seemed to improve upon normalization of the vitamin D and phosphorous deficiency; however, we were not able to differentiate between the two.
In conclusion, exocrine pancreas insufficiency and vitamin D deficiency should be kept in mind as a possible reason for impaired gait and skeletal muscle weakness; knowledge regarding optimal vitamin D treatment in cases of pancreatic insufficiency remains scarce.
Acknowledgements
We thank staff at the Information Department and Library of Viborg Regional Hospital, for their valuable assistance.
Conflicts of interests
We report no conflicts of interests
References
- Abellan van Kan G. Epidemiology and consequences ofsarcopenia. J Nutr Health Aging 2009; 13:708-12. [PMID 19657554]
- Blain H, Carriere I, Sourial N, Berard C, Favier F, Colvez A,Bergman H. Balance and walking speed predict subsequent 8-yearmortality independently of current and intermediate events in wellfunctioningwomen aged 75 years and older. J Nutr Health Aging2010; 14:595-600. [PMID 20818476]
- Teichmann J, Mann ST, Stracke H, Lange U, Hardt PD, BretzelRG, Klör HU. Parathormone levels and Vitamin D metabolism infemale patients with various grades of fecal elastase 1 deficiency.Eur J Med Res 2008; 13:563-7. [PMID 19073396]
- Ceglia L. Vitamin D and its role in skeletal muscle CurrOpinClinNutrMetab Care 2009; 12:628-33. [PMID 19770647]
- Teichmann J, Mann ST, Stracke H, Lange U, Hardt PD, KlörHU, Bretzel RG. Alterations of vitamin D3 metabolism in youngwomen with various grades of chronic pancreatitis. Eur J Med Res2007; 12:347-50. [PMID 17933711]
- Ferguson JH, Chang AB. Vitamin D supplementation for cysticfibrosis. Cochrane Database Syst Rev 2009; 4:CD007298. [PMID19821402]
- Leventis P, Kiely PD. The tolerability and biochemical effects ofhigh-dose bolus vitamin D2 and D3 supplementation in patients withvitamin D insufficiency. Scand J Rheumatol 2009; 38:149-53. [PMID 18991184]
- Pearce SH, Cheetham TD. Diagnosis and management ofvitamin D deficiency. BMJ 2010; 340:b5664. [PMID 20064851]
- van den Bergh JP, Bours SP, van Geel TA, Geusens PP. Optimaluse of vitamin D when treating osteoporosis. CurrOsteoporos Rep2011; 9:36-42. [PMID 21113692]
- Broe KE, Chen TC, Weinberg J, Bischoff-Ferrari HA, HolickMF, Kiel DP. A higher dose of vitamin d reduces the risk of falls innursing home residents: a randomized, multiple-dose study. J AmGeriatrSoc 2007; 55:234-9. [PMID 17302660]
- Schubert L, DeLuca HF. Hypophosphatemia is responsible forskeletal muscle weakness of vitamin D deficiency. Arch BiochemBiophys 2010; 500:157-61. [PMID 20515645]


