Ravi Ranjan Tripathi*
Department of Pediatric Cardiology, CHL Hospital, Indore, Madhya Pradesh, India
*Corresponding Author:
Ravi Ranjan Tripathi
Department of Pediatric Cardiology
CHL Hospital, AB Road, Near LIG Square, Indore,
Madhya Pradesh
India
Tel: 919425314455
E-mail: drravirt@gmail.com
Received date: October 14, 2017; Accepted date: November 15, 2017; Published date: November 22, 2017
Citation: Tripathi RR (2017) Simultaneous Transcatheter Device Closure of ASD, VSD and PDA in an Infant with Down Syndrome. Interv Cardiol J. Vol.3 No.3:69
Incidence of congenital heart defects in Down syndrome varies from 40% to 60%. Atrioventricular septal defect is most common defect seen, followed by isolated Ventricular Septal Defect (VSD). Multiple defects can be found in 5% to 10% of Down syndrome babies. Such patient usually presents with Pulmonary Hypertension (PAH) early in life and can develop rapid progression. An infant with Down syndrome weighing 6.5 kg presented with recurrent lower respiratory tract infections. A Transthoracic echocardiogram showed 10 mm secundum Atrial Septal Defect (ASD), 5 mm peri membranous Ventricular Septal Defect (VSD) and 3.5 mm conical shaped Patent Ductus Arteriosus (PDA) with Pulmonary Arterial Hypertension (PAH). As all the defects were suitable for transcatheter closure, patient underwent successful device closure of VSD by 6/4 mm Amplatzer duct occluder II (ADO II) device, PDA closure by 6/4 mm Amplatzer duct occluder (ADO) device and ASD closure by 12 mm Amplatzer septal occluder device. PA pressures of patient reduced significantly after the procedure and possible post-operative morbidity was avoided by transcatheter intervention.
Keywords
Simultaneous device closure; Down syndrome; Multiple defects; Transcatheter interventions.
Introduction
Congenital heart defects (CHD) in Down’s syndrome varies from 40% to 60% in various studies. Atrioventricular septal defect (AVSD) is most common defect followed by isolated ventricular septal defect (VSD). Presence of multiple left to right shunts in a child with Down’s syndrome is possible in about 5% to 10% [1]. Results of corrective surgery for various heart defects in Down syndrome are comparable to normal population however postoperative morbidity is common [2]. Transcatheter interventions are suitable alternative to surgery for various heart defects. Although there are no weight criteria for smaller babies, improving hardware and interventional technique have led to successful treatment of infants with lesser weight using device closures [3]. Multiple defects are usually treated with surgery, we describe a case of an infant with Down’s syndrome with ASD, VSD and PDA who was treated with simultaneous transcatheter device closure of all the defects as all the defects were suitable for interventional procedure (Figure 1).

Figure 1: Echo images of shunts before and after the procedure.
Case Presentation
A 1-year-old male child weighing 6.5 kg was referred to our hospital for cardiac evaluation. He was a known case of Down syndrome. He had repeated episodes of lower respiratory tract infections, slow weight gain, and systolic murmur. Auscultation revealed loud pulmonary component (P2), soft long systolic murmur and bilateral wheeze and mild crepitations over the chest. His thyroid function was normal. His cardiac radiograph (chest X-ray) revealed mild cardiomegaly with prominent pulmonary vascular markings (Figure 2). ECG showed heart rate of 110 per minute with sinus rhythm, QRS axis +100, biventricular dominance. Transthoracic echocardiography (TTE) showed 10 mm secundum atrial septal defect (ASD), 5 mm perimembranous ventricular septal defect (VSD) and conical patent ductus arteriosus (PDA) measuring 3.5 mm at pulmonary end. All shunts were shunting predominantly left to right. His pulmonary artery (PA) pressures were raised to about 60 mmHg with normal biventricular function. All rims around ASD were adequate for device closure. VSD margin had 3 mm distance from aortic valve and away from inlet septum. Patient was advised diuretics and bronchodilator therapy and chest signs improved in next 48 hours. It was decided to take the patient for transcatheter device closure of multiple defects as lesions were suitable for the procedure and presence of Down syndrome increased likelihood of rapid progression of pulmonary hypertension. His pre-procedure hemodynamic assessment during the transcatheter procedure showed high pulmonary artery (PA) pressures (60/25 mm Hg) against systemic arterial pressures of 75/35 mmHg. First VSD device closure was performed from arterial route using 6/4 Amplatzer duct occluder II (ADO II) device by 5 French guiding catheters. Then PDA was closed using standard technique by 6/4 Amplatzer duct occluder device. Finally, ASD device closure was performed using 12 mm Amplatzer Septal occluder device with 7 French delivery systems. Post procedure PA pressures reduced to 45/15 mmHg against systemic pressures of 80/45 mmHg. Electrocardiogram (ECG) showed sinus rhythm with heart rate of 110/min. Post procedure TTE showed stable device positions, some foaming across the devices and good biventricular function. Patient was discharged from hospital after 72 hours of observation. After one month, patient is asymptomatic with normal TTE findings, no residual shunts, reduced PA pressures (estimated PA systolic pressures of 40 mmHg by TR jet method) and good biventricular function (Figure 3).
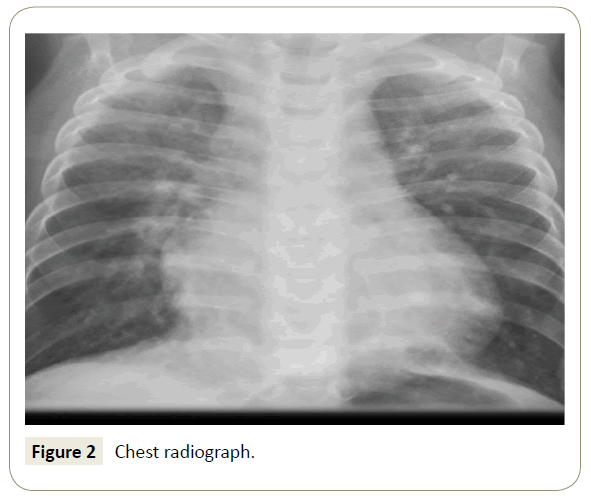
Figure 2: Chest radiograph.
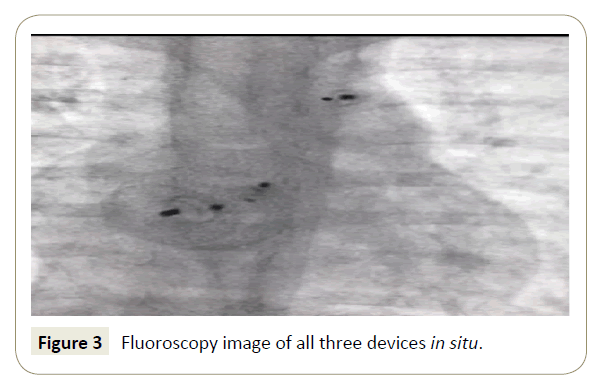
Figure 3: Fluoroscopy image of all three devices in situ.
Discussion
Traditionally multiple shunts in a child have been closed by surgical procedures with excellent results. But in recent years, there has been shift towards transcatheter approach for suitable lesions [4]. Use of improved hardwares, smaller sheath sizes and newer techniques have made it possible to simultaneously treat multiple cardiac lesions in children using interventional methods. Infants under one year of age are successfully treated with such procedures [5]. Increased incidence and rapid progression of pulmonary hypertension in children with Down syndrome has been well known [6]. Hence, we decided for simultaneous closure of three defects in our patient. I do not recommend regular use of transcatheter interventions for multiple defects in infants, however carefully selected patients can be offered such procedures.
Conclusion
To best of my knowledge, this is first case report of an infant with Down syndrome undergoing simultaneous closure of ASD, VSD and PDA using transcatheter approach in a single procedure.
References
- SB Freeman, Taft LF, Dooley KJ, Allran K, Sherman SL, et al. (1998) Population based study of congenital heart defects in Down syndrome. Am J Med Genet 80: 213- 217.
- Fudge JC, Li S, Jaggers J, O'Brien SM, Peterson ED, et al. (2010) Congenital heart surgery outcomes in Down syndrome: Analysis of a national clinical database. Pediatrics 126: 315-322.
- Cardenas L, Panzer J, Boshoff D, Malekzadeh-Milani S, Ovaert C (2007) Transcatheter closure of secundum atrial defect in small children. Catheter Cardiovasc Interv 69: 447-452.
- Atiq M, Khan SA, Tipu FA, Amin Z (2008) Combined treatment for multiple cardiac defects with interventional techniques. Pediatr Cardiol 29: 890-893.
- Prada F, Mortera C, Bartrons J, Rissech M, Jiménez L, et al. (2009) Percutaneous treatment of atrial septal defects, muscular ventricular septal defects and patent ductus arteriosus in infants under one year of age. Rev Esp Cardiol 62: 1050-1054.
- Cua CL, Blankenship A, North AL, Hayes J, Nelin LD (2007) Increased Incidence of idiopathic persistent pulmonary hypertension in Down syndrome neonates. Pediatr Cardiol 28: 250-254.

