Keywords
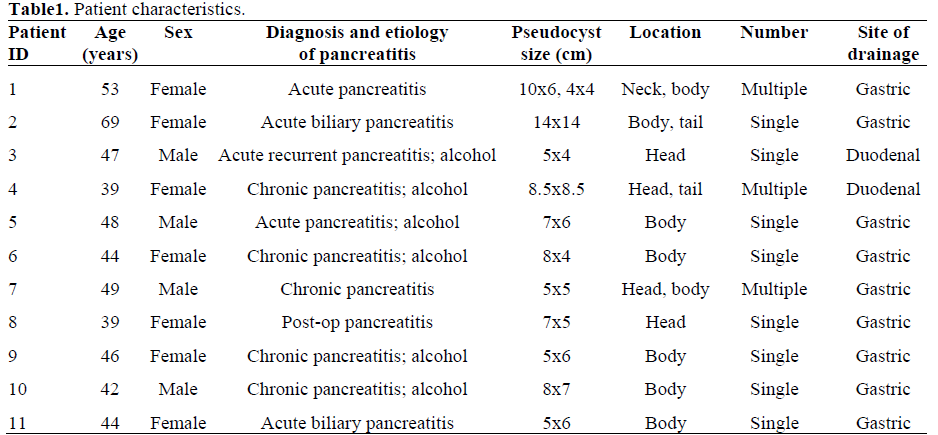
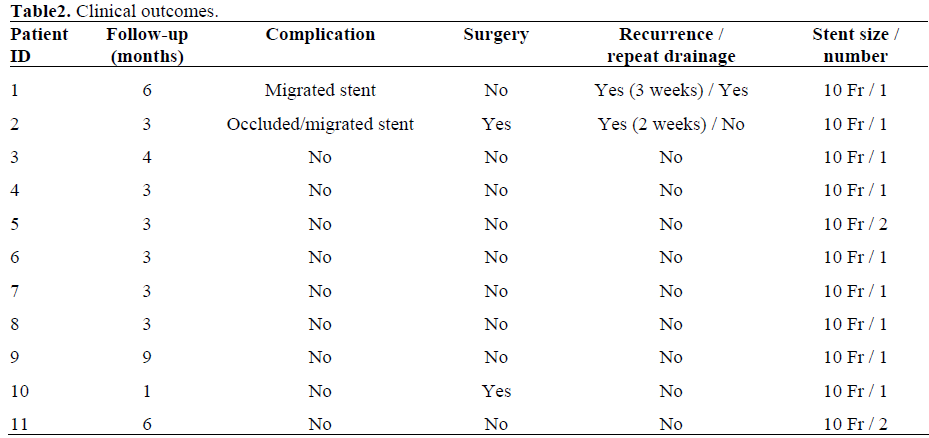
Cysts; Drainage; Endosonography; Pancreas;Pancreatitis
INTRODUCTION
Endoscopic transmural drainage is a widely reported treatment modality for pancreatic pseudocysts [1, 2, 3, 4, 5]. Reported outcomes with this technique are favorable. However, a major limitation has been the relatively “blind” approach that carries a significant risk of bleeding and perforation [1, 2]. The ideal approach for pancreatic pseudocyst puncture combines endoscopy with real time endosonography. Several authors have described successful use of radial or linear array echoendoscope for guiding transmural puncture and drainage procedures [6, 7, 8, 9, 10, 11].
EUS-guided pancreatic pseudocyst drainage traditionally involved a two-step approach [12, 13, 14, 15, 16, 17, 18]. First step was to identify an optimal puncture site with radial or linear array echoendoscope. The second step involved an exchange of echoendoscope with a duodenoscope for puncturing the identified site using a needle knife followed by placement of stent. A single-step approach using only echoendoscope (without duodenoscope) became feasible once the large channel (2.4 to 3.2 mm) linear array echoendoscope became available [6, 7, 8, 10, 11]. However, limited diameter of the working channel of linear echoendoscope prevented placement of large stents such as a10 Fr stent. Larger stents or multiple stents have been shown to improve outcomes [19].
New therapeutic large channel linear echoendoscopes have now become available from different manufacturers (Olympus, Melvile, NY, USA; Pentax, Montvale, NJ, USA). These scopes have larger (3.7 to 3.8 mm) working channel (permits 10 Fr stent delivery) and an elevator control for accessories. Additionally, newer accessories such as cystotome (Wilson Cook, Winston-Salem, NC, USA) have also become available for transmural puncture of pancreatic cysts. Cystotome is used to electrosurgically cannulate the transgastric or transduodenal wall into a pancreatic pseudocyst. We describe a simple one-step approach for pancreatic pseudocyst drainage using a 3.8 mm working channel linear array echoendoscope (Pentax, Montvale, NJ, USA) and a new accessory device cystotome (Wilson Cook, Winston-Salem, NC, USA). Clinical outcomes in 11 patients with this approach are presented.
PATIENTS AND METHODS
A total of 15 consecutive patients with symptomatic pancreatic pseudocysts were evaluated for EUS-guided pseudocyst drainage from August 2004 to May 2005. Four patients were considered ineligible for EUS-guided pseudocyst drainage because of the presence of a large intervening vessel, greater than 10 mm thick gastric wall or debris. Eleven patients underwent EUS-guided pancreatic pseudocyst drainage. All patients were symptomatic and their pseudocyst had failed to resolve in six weeks. A total of 12 procedures were performed in 11 patients. Patient characteristics are described in Table 1. Endoscopic therapy was preceded by abdominal imaging such as computerized tomography (CT) or transabdominal ultrasonography in all patients. All procedures were performed using a new large channel therapeutic linear array echoendoscope (EG-3830UT, Pentax, Montvale, NJ, USA) (Figure 1a), ultrasound processor (EUB 6500, Hitachi Medical Systems America Inc., Twinsburg, Ohio, USA) and a new accessory device cystotome (Wilson Cook, Winston-Salem, NC, USA) (Figure 1b). Therapeutic linear arrays echoendoscope has a 3.8 mm working channel that permits 10 Fr stent delivery. It has an increased 120 degree angle of view and an elevator control for accessories. The cystotome is a modified needle knife papillotome that consists of an inner wire with a needle knife tip, a 5 Fr inner catheter, and a 10 Fr outer catheter equipped with a diathermy ring at its distal tip. The proximal end of this device includes a handle with connectors for active cords and a fitting to provide for injection of contrast material.
Figure 1. a. Therapeutic linear echoendoscope (Pentax, Montvale, NJ, USA). b. Cystotome (Wilson Cook, Winsston-Salem, NC, USA).
Technique of EUS-Guided Pancre Pseudocyst Drainage (Videoclip 1).
All procedures were performed in the fluoroscopy suite after obtaining an informed consent from each patient. Patients were given conscious sedation using intravenous propofol (Diprivan® AstraZeneca Pharm-aceuticals LP, Wilmington, DE, USA) by an Figure 2. a.Endosonographic view of pancreatic pseudocyst. b. Fluorscopic view showing guidewire in the pancreatic cyst. c.Cystotome outer catheter with metal ring enlarging the initial puncture site. Videoclip 1. EUS-guided pancreatic pseudocystdrainage. JOP. Journal practitioner under the supervision of an anesthesiologist. All patients were kept in the left lateral position during the procedure. All patients were given a broad-spectrum antibiotics during and after the procedure to reduce the risk of secondary infection. Following steps were used to perform EUS-guided pseudocyst drainage.
Figure 2. a. Endosonographic view of pancreatic pseudocyst. b. Fluorscopic view showing guidewire in the pancreatic cyst. c. Cystotome outer catheter with metal ring enlarging the initial puncture site.
1. Using the video endoscopic function of the therapeutic linear gastroduodenoscopy was performed and the cystic lesion was identified as a bulge in the gastric or duodenal lumen. The cystic lesion was examined ultrasonographically (Figure 2a).
2. The optimal puncture site was determined using assessment of the gastric or duodenal wall at the puncture site was also obtained. Intervening vessels, gastric or duodenal wall thickness at the puncture site greater than 10 mm, and the presence of debris or organized material in the cyst were considered not suitable for EUS-guided pancreatic pseudocyst drainage. Four patients were found unsuitable out of a total of 15 that were evaluated for EUS-guided pseudocyst drainage.
3. After determination of the optimal site for puncture, punctured with cystotome using the knife tip of the inner catheter and then entered with the inner catheter. Electrocautery (ERBE generator, ERBE USA Inc., Marietta, GA, USA) was performed with needle knife settings (coag power 25-30 W and autocut to 80-100 W). The metal part of the inner catheter was then withdrawn leaving the Teflon® catheter in the pancreatic cyst. A sample of cyst contents was then aspirated and submitted for biochemical, cytological and tumor markers analysis. A 0.035 inch guidewire was passed through the inner catheter into the cyst cavity. The guidewire position was confirmed using fluoroscopy (Figure 2b.)
4. The outer 10 Fr sheath of cystotome is equipped with advanced through the puncture site using electrocautery (ERBE generator, ERBE USA Inc., Marietta, GA, USA) with needle knife settings (coag power 25-30 W and autocut to 80-100 W), thus enlarging the puncture site (Figure 2c). The cystotome was then removed leaving the guidewire in the cyst cavity.
5. The puncture site was dilated using an 8 mm dilator balloon over-the-wire (Figure 3)
Figure 3. Balloon dilation of cystostomy. a. Endoscopic view. b. Fluroscopic view.
6. A 10 Fr double pigtail stent was placed over-the-wire under endoscopic and fluoroscopic monitoring (Figure 4a). The puncture site and the pancreatic pseudocyst were cannulated with a guidewire using a standard papillotome (Figure 4b) and then a second double pig tail stent was placed into the cyst cavity under endoscopic and fluoroscopic control (Figure 5). Pancreatic pseudocyst was then reassessed endosonographically.
Figure 4. a. Fluoroscopic view showing double pig tail 10 Fr stent placed in to the pancreatic pseudocust. b. Cannulation of cystostomy using sphincterotome
Figure 5. a. Endoscopic view of transgastric stents into the pancreatic pseudocyst. b. Fluoroscopic view showing transgastric stents in to the pancreatic pseudocyst.
All patients were observed for 24-48 hours post procedure. A CT 24 hours of the pseudocyst drainage, at two-week follow-up, and periodically thereafter until complete resolution was confirmed on serial scans. An upper endoscopy was done to remove the stents once pancreatic pseudocyst had resolved.
ETHICS
An inform consent was obtained from each patient and the study protocal conforms to the
ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004, as reflected in a priori approval by the review committee of our institution.
STATISTICS
Because of this is an uncontrolled and small sample size series ,only descriptive statistics
are used (men, median, range, and frequencies).
RESULTS
Successful
Placement of one or two 10 Fr double pigtail stents was successful in all patients who were considered eligible for EUS-guided pseudocyst drainage. One patient underwent surgery (cystogastrostomy) following day after the EUS guided drainage because of complete stent migration into the pseudocyst that was noted on repeat imaging. This patient had a single 5 cm long 10 Fr double pigtail stent. Two recurrences of pseudocysts were noted over a mean follow-up period of 4 months (range 3-6 months). Both patients who had recurrence were found to have migrated stents. One patient underwent surgical cystogastrostomy because of organized cyst contents and possible pseudocyst infection. The second patient was successfully managed with EUS-guided repeat drainage of pseudocyst with a 10 Fr double pigtail stent.
EUS-guided stent placement was successful in all 11 patients
patients required surgery (cystogastrostomy) because of stent migration and suspected infection. Overall, 9 out of 11 patients (82%) patients were successfully managed with EUS-guided pseudocyst drainage. Except one, all patients required one EUS-guided drainage procedure. The mean interval to resolution of pseudocyst or removal of stent was 4.4 months (median 3 months). No bleeding or perforation occurred over the study period.
DISCUSSION
Endosonography is used increasingly in the treatment of pancreatic psedocyst [6, 7 ,8 ,9 , 10 ,11] This technique allows the operator to locate areas of contact between the cyst and gastric or duodenal wall. The need for EUS before or during the transmural intervention has not been evaluated in controlled trials, and is a matter of controversy. However, bleeding rate up to 6-10% has been reported with transmural drainage without EUS guidance [1, 2]. EUS also enables drainage of pancreatic pseudocyst without apparent luminal bulge [20].
A time consuming and cumbersome two-step approach has been
[12, 13, 14, 15, 16, 17, 18]. In comparison only a few case series of one-step EUS-guided pancreatic pseudocyst drainage are reported [6, 7, 8, 10, 11]. Reported success rate with one-step approach varies between 50 to 100%. Largest series by Giovannini et al. [10] described 88.5% success rate with a single-step approach using a 3.2 mm channel linear array echoendoscope in placing 8.5 Fr stent or nasocystic drain. Heterogeneity in patient characteristics likely account for the difference in outcomes reported between studies. Outcomes also vary according to the experience of the endoscopist and the type of pancreatic fluid collections [21, 22]. We were successful in placing a large diameter (10 Fr) stent in all 11 patients. However, 2 patients required surgical cystogastrostomy because of stent migration into the pseudocyst and suspected infection. Our long-term success rate of 82% is comparable to that reported in the literature [6, 7, 10].
Most authors have used needle knife catheter but the needle can be
endosonographically, and diathermy is usually required to puncture the cyst. A standard fine needle aspiration (FNA) needle is well visualized sonographically and can be used for pseudocyst puncture but the drawback of the needle is its small caliber (22 gauge) which will accept only 0.018 inch guidewire. Using a 19-gauge FNA needle (Wilson Cook, Winston-Salem, NC, USA) a 0.035 inch guidewire can be inserted into the pseudocyst. Recently Seifert et al. [6, 7] described a “one-step” instrument for EUS-guided pancreatic pseudocyst stenting. The 19-gauge stainless steel puncture needle is loaded with a modified 7 Fr or 10 Fr stent and a pusher catheter. The stent is 6 cm long and has two side holes and four flaps to prevent migration. The success rate was 8/10 patients. This system is not available in the USA. Wiersema et al. [23] reported successful use of a large channel (3.7 mm) echoendoscope with an elevator in draining pancreatic pseudocyst using needle knife to puncture pseudocyst. We used cystotome to puncture pseudocyst because it has the advantage of enlarging initial point of entry by its 10 Fr outer catheter that is equipped with a diathermy ring. It makes easier to pass accessories such as a dilator catheter through the puncture site. Additionally, this device is easier to use and enables a large transmural puncture in one step.
Therapeutic echoendoscope is mechanically similar to therapeutic
allows the use of accessories that have been designed for use in biliary endoscopy. Although smaller stents may be adequate for drainage of pseudocysts that do not contain debris; however, this may carry a greater risk of infection caused by premature stent clogging [2]. Placement of multiple stents will decrease the risk but repeated access to the cyst cavity can be difficult, prolongs the procedure and will not achieve the same degree of drainage provided by larger stent [19]. In our series, stent migrated in 3 patients. In all 3
diameter and 5 cm length) was placed. A number of factors may contribute to the migration of stents. Stent design is an important consideration; however, there are no comparative trials establishing the superiority of one stent design to the other in terms of migration rates (i.e. straight vs. pigtail). The size of endoscopic cystogastrostomy is another factor that may have contributed to stent migration in our patients. We dilated cystogastrostomy orifice to 8 mm using a dilator balloon; 8 mm orifice may have provided poor stent anchorage particularly when only one stent was placed. Among patients who had two stents placed, none migrated. Stent length is a consideration that may not directly influence the risk of migration but may have bearing on whether migration becomes clinically significant particularly with straight stents. However, we used only double pigtail stents.
In summary, a single-step approach using a large channel (3.8 mm)
echoendoscope with an elevator is feasible because its wider working channel permits 10 Fr stent delivery without exchanging the echoendoscope with a therapeutic duodenoscope. The use of cystotome allows one-step cyst puncture and its enlargement that enables easier passage of balloon dilator catheter. EUS-guided placement of 10 Fr stent was successful in all 11 patients in our series; however, pseudocyst drainage was effective in 82% of patients. This approach appears useful in managing selected patients with symptomatic pancreatic pseudocysts.
References
- Sahel J, Bastid C, Pellat B, Schurgers P, Sarles H. Endoscopic cystoduodenostomy of cysts of chronic calcifying pancreatitis: a report of 20 cases. Pancreas 1987; 2:447-53. [PMID 3628239]
- Cremer M, Deviere J, Engelholm L. Endoscopic management of cysts and pseudocysts in chronic pancreatitis: long-term follow-up after 7 years of experience. Gastrointest Endosc 1989; 35:1-9. [PMID 2920879]
- Lehman GA. Pseudocysts. Gastrointest Endosc 1999; 49:S81-4. [PMID 10049456]
- Vitale GC, Lawhon JC, Larson GM, Harrell DJ, Reed DN Jr, MacLeod S. Endoscopic drainage of the pancreatic pseudocyst. Surgery 1999; 126:616-21. [PMID 10520906]
- Cahen D, Rauws E, Fockens P, Weverling G, Huibregtse K, Bruno M. Endoscopic drainage of pancreatic pseudocysts: long-term outcome and procedural factors associated with safe and successful treatment. Endoscopy 2005; 37:977-83. [PMID 16189770]
- Seifert H, Dietrich C, Schmitt T, Caspary W, Wehrmann T. Endoscopic ultrasound-guided one-step transmural drainage of cystic abdominal lesions with a large-channel echo endoscope. Endoscopy 2000; 32:255-9. [PMID 10718392]
- Seifert H, Faust D, Schmitt T, Dietrich C, Caspary W, Wehrmann T. Transmural drainage of cystic peripancreatic lesions with a new large-channel echoendoscope. Endoscopy 2001; 33:1022-6. [PMID 11740644]
- Wiersema MJ. Endosonography-guided cystoduodenostomy with a therapeutic ultrasound endoscope. Gastrointest Endosc 1996; 44:614-7. [PMID 8934175]
- Binmoeller KF, Soehendra N. Endoscopic ultrasonography in the diagnosis and treatment of pancreatic pseudocysts. Gastrointest Endosc Clin N Am 1995; 5:805-16. [PMID 8535629]
- Giovannini M, Pesenti C, Rolland AL, Moutardier V, Delpero JR. Endoscopic ultrasound guided drainage of pancreatic pseudo-cyst and pancreatic abscess using a therapeutic echoendoscope. Endoscopy 2001; 33:473-7. [PMID 11437038]
- Giovannini M, Bernardini D, Seitz JF. Cystogastrotomy entirely performed under endosonography guidance for pancreatic pseudocyst: results in six patients. Gastrointest Endosc 1998; 48:200-3. [PMID 9717789]
- Chan AT, Heller SJ, Van Dam J, Carr-Locke DL, Banks PA. Endoscopic cystgastrostomy: role of endoscopic ultrasonography. Am J Gastroenterol 1996; 91:1622-5.[PMID 8759673]
- Savides TJ, Gress F, Sherman S, Rahaman S, Lehman GA, Hawes RH. Ultrasound catheter probe-assisted endoscopic cystgastrostomy. Gastrointest Endosc 1995; 41:145-8. [PMID 7721002]
- Norton ID, Clain JE, Wiersema MJ, DiMagno EP, Petersen BT, Gostout CJ. Utility of endoscopic ultrasonography in endoscopic drainage of pancreatic pseudocysts in selected patients. Mayo ClinProc 2001; 76:794-8. [PMID 11499818]
- Gerolami R, Giovannini M, Laugier R. Endoscopic drainage of pancreatic pseudocysts guided by endosonography. Endoscopy 1997; 29:106-8. [PMID 9101147]
- Ardengh JC, Della Libera E, Ferrari AP. Endosonography-guided drainage of pancreatic pseudocyst without gastric or duodenal compression. Endoscopy 1998; 30:S71-2. [PMID 9746177]
- Fuchs M, Reimann FM, Gaebel C, Ludwig D, Stange EF. Treatment of infected pancreatic pseudocysts by endoscopic ultrasonography-guided cystogastrostomy. Endoscopy 2000; 32:654-7. [PMID 10935798]
- Vosoghi M, Sial S, Garrett B, Feng J, Lee T, Stabile BE, Eysselein VE. EUS-guided pancreatic pseudocyst drainage: review and experience at Harbor-UCLA Medical Center. MedGenMed 2002; 4:2. [PMID 12466745]
- Baron TH, Morgan DE. Current concepts: acute necrotizing pancreatitis. N Engl J Med 1999; 340:1412-7. [PMID 10228193]
- Sriram PV, Kaffes AJ, Rao GV, Reddy DN. Endoscopic ultrasound-guided drainage of pancreatic pseudocysts complicated by portal hypertension or by intervening vessels. Endoscopy 2005; 37:231-5. [PMID 15731938]
- Harewood GC, Wright CA, Baron TH. Impact on patient outcomes of experience in the performance of endoscopic pancreatic fluid collection drainage. Gastrointest Endosc 2003; 58:230-5. [PMID 12872091]
- Baron TH, Harewood GC, Morgan DE, Yates MR. Outcome differences after endoscopic drainage of pancreatic necrosis, acute pancreatic pseudocysts, and chronic pancreatic pseudocysts. Gastrointest Endosc 2002; 56:7-17. [PMID 12085029]
- Wiersema MJ, Baron TH, Chari ST. Endosonography-guided pseudocyst drainage with a new large-channel linear scanning echoendoscope. Gastrointest Endosc 2001; 53:811-3. [PMID 11375600]






