Keywords
Biopsy, Fine-Needle; Cytology; Pancreas; Solitary Fibrous Tumor
INTRODUCTION
Solitary fibrous tumor is an uncommon spindle cell tumor of mesenchymal origin with predominately benign behavior [1]. Solitary fibrous tumor is typically found in the pleura but can occur in non-pleural tissue [1]. Pancreatic solitary fibrous tumor is extremely rare with only four previously reported cases [2, 3, 4, 5]. Due to the rarity and nonspecific clinical presentation, this entity is diagnostically challenging [2, 3, 4, 5]. We describe a 78-year-old woman with a solitary fibrous tumor arising in the body of the pancreas along with a review of the literature [2, 3, 4, 5]. This is the first report of successful fine needle aspiration cytology on a pancreatic solitary fibrous tumor. Fine needle aspiration can be used as a less invasive diagnostic tool rather than biopsy.
CASE REPORT
A 78-year-old woman with a history of polymyalgia rheumatica presented to her primary care physician with chronic back pain. The patient reported increasing fatigue and loss of appetite with a 9 kg unintentional weight loss. Her serum laboratory results were only significant for decreased hemoglobin (9.6 g/dL; reference range: 11.6- 15.4 g/dL), hematocrit (27.6%; reference range: 34-45%), calcium (8.0 mg/dL; reference range: 8.5-10.5 mg/dL), total protein (4.1 g/dL; reference range: 6.0-8.0 g/dL), and albumin (2.1 g/dL; reference range: 3.5-5.0 g/dL). Serum tumor markers (chromogranin, CEA, CA 19-9) were within normal limits. Lumbar CT imaging revealed a pancreatic mass. A dynamic, contrastenhanced CT of the pancreas confirmed a 5 cm solid mass arising from the body of the pancreas with no other significant abnormalities identified (Figure 1a). The mass showed hyper-enhancement on arterial phase imaging. Based upon the tumor location, vascularity and well-circumscribed nature, an endocrine tumor was considered to be the most likely diagnosis.
Figure 1. a. Triphasic CT of the pancreas reveals a 5
cm solid mass arising from the body of the pancreas. b. Cell block H&E stain from the fine needle aspirate
specimen showed bland appearing spindle cells (40x). c. Vimentin immunohistochemical stain of the cell
block specimen with tumor cells that have strong
positivity (40x). d. Pancreatic resection specimen
demonstrated a 5.0x5.0x4.5 cm well circumscribed
non-encapsulated mass (arrow) present in the body of
the pancreas, which is shown bisected. e. H&E stain of
the resected tumor revealed spindle cells in a variably
collagenous background with minimal cytologic atypia
and rare mitotic activity (40x). f. Bcl-2 immunohistochemical
stain of the resected mass with tumor
cells that have strong positivity (40x).
An endoscopic ultrasound with fine needle aspiration was performed to confirm the radiographic findings. A cell block preparation demonstrated bland-appearing spindle cells and an immunohistochemical analysis was performed (Figure 1b). Tumor cells were positive for CD34 and vimentin, and negative for CAM 5.2, CD10, chromogranin, synaptophysin, CD117, desmin, and S100 (Figure 1c). Both cytologic appearance and immunohistochemistry were inconsistent with an endocrine tumor and a diagnosis of benign mesenchymal tumor was given. The patient was taken to surgery and a distal pancreatectomy was performed. The removed portion of pancreas measured 9.2x6.5x4.5 cm and contained a 5.0x5.0x4.5 cm well-circumscribed, non-encapsulated, white mass with a homogeneous, smooth cut surface 0.8 cm from the pancreatic surgical resection margin (Figure 1d).
Histologically, the tumor was composed of haphazardly arranged bland spindle cells (Figure 1e). A background of wispy collagen bands and occasional branched hemangiopericytoma-like vessels were seen. Cytologic atypia, necrosis, and vascular invasion were not identified. Mitotic figures were very rare (less than 1 mitosis per 10 per high-powered fields). No entrapped pancreatic tissue was identified in the tumor. Immunohistochemical stains on the resected tumor revealed lesional cells diffusely positive for CD99, vimentin, and bcl-2, focally positive for CD34, and negative for CD117, desmin, smooth muscle actin, CAM 5.2, CD10, chromogranin, synaptophysin, and S100 (Figure 1f). Based on histology and immunohistochemistry, a diagnosis of solitary fibrous tumor was rendered. Seven months post-operatively, the patient is disease free and has gained 5 kg.
DISCUSSION
The vast majority of primary pancreatic tumors are adenocarcinomas [6]. Endocrine tumors are uncommon and mesenchymal tumors are even more rare [6]. Mesenchymal tumors of the pancreas include lymphangioma, adenomatoid tumor, hemangioma, schwannoma, perivascular epithelioid cell tumor (PEComa), and solitary fibrous tumor [7]. These behave primarily in a benign manner [7]. Malignant pancreatic mesenchymal tumors such as liposarcoma, leiomyosarcoma, and malignant fibrous histocytoma have also been identified [7].
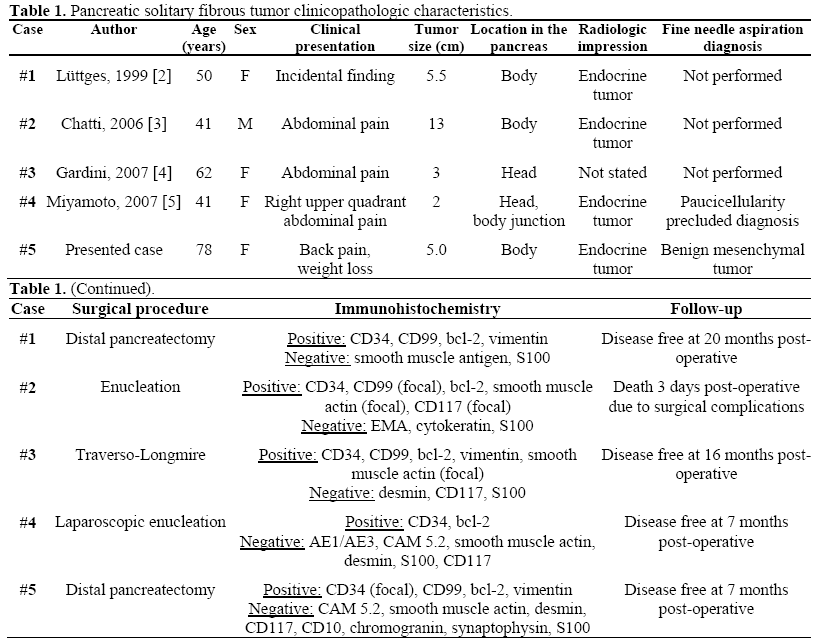
Including our patient, only five cases of pancreatic solitary fibrous tumor have been reported with the clinical findings summarized in Table 1 [2, 3, 4, 5]. The five patients ranged from ages 41-78 years with a mean age of 54.4 years, with our patient being the oldest described [2, 3, 4, 5]. Although solitary fibrous tumor has no gender bias reported, the current pancreatic cases have female to male ratio of 4:1 [2, 3, 4, 5]. Four patients presented with pain, either in the abdomen or back and the remaining tumor was detected incidentally during imaging for an unrelated condition [2, 3, 4, 5]. In four cases, the radiologic impression favored an endocrine tumor, as these tumors can appear similarly well-circumscribed and hypervascular on cross-sectional imaging studies [2, 3, 5]. All five cases of pancreatic solitary fibrous tumor were treated with surgical resection [2, 3, 4, 5]. The size of the tumors ranged from 2 to 13 cm with a mean of 5.7 cm [2, 3, 4, 5]. Four patients remain disease free during the stated follow-up period and one patient died three days postoperatively due to complications of surgery [2, 3, 4, 5]. The lack of metastases in patients with pancreatic solitary fibrous tumor supports the designation of this lesion as benign [2, 3, 4, 5].
It is significant to point out that our case was diagnosed as a benign mesenchymal tumor based on aspiration cytology. One prior case attempted fine needle aspiration, however, paucicellularity precluded a diagnosis [5]. Histologically, the surgical resection specimens from all five cases were described as being composed of bland appearing spindle cells within a variably collagenous background with benign features including minimal cellular pleomorphism and low mitotic activity (less than 4 mitoses per 10 high-powered fields) [2, 3, 4, 5]. Macroscopic necrosis was identified in one case in which the tumor was quite large (13 cm) [3]. Entrapped exocrine pancreatic tissue was present in two cases with one of those cases also containing endocrine tissue [2, 5].
Immunohistochemistry is an important part of the work-up in diagnosing solitary fibrous tumor, particularly if the tumor is in a rare location. Immunohistochemically, solitary fibrous tumor is usually positive for CD34 and CD99 and negative for desmin, CD117, chromogranin, synaptophysin, with variable positivity for epithelial membrane antigen, bcl-2, smooth muscle actin, and S100 [2]. The main diagnostic consideration of a pancreatic solitary fibrous tumor based on imaging is an endocrine neoplasm. Endocrine neoplasms are easily microscopically distinguished from solitary fibrous tumor as they are composed of nests to trabeculae of round cells with granular eosinophilic cytoplasm, have “salt and pepper” chromatin and are positive for synaptophysin and chromogranin. The histologic differential diagnosis of pancreatic solitary fibrous tumor includes other spindle cell neoplasms, as many can have sclerosis and hyalinization. Within the pancreas, leiomyosarcoma is the most frequent spindle cell neoplasm and must be differentiated from solitary fibrous tumor as the prognosis is dramatically worse [2]. Leiomyosarcoma is characterized by a fascicular growth pattern with nuclear atypia and mitotic activity, unlike solitary fibrous tumor [2]. Positivity for desmin and smooth muscle actin separate leiomyosarcoma, as well as leiomyoma, from solitary fibrous tumor [2]. Gastrointestinal stromal tumor is a spindle cell lesion which immunohistochemically overlaps with solitary fibrous tumor. Both tumors are positive for vimentin and CD34, but gastrointestinal stromal tumor is positive for CD117 whereas solitary fibrous tumor is negative [2, 7]. Immunohistochemistry was performed in all five cases and confirmed the diagnosis of solitary fibrous tumor [2, 3, 4, 5].
In conclusion, we have reported the fifth case of pancreatic solitary fibrous tumor. This lesion is difficult to radiologically distinguish from other pancreatic neoplasms by crosssectional imaging. In our case, fine needle aspiration proved helpful to determine the benign mesenchymal nature of the tumor and was concordant with the pathologic findings at surgery. Histologic examination and immunohistochemistry were necessary to make the diagnosis of solitary fibrous tumor. While some malignant histologic features have been described in the literature, further reports and longer follow-up are needed to truly know the prognosis of this rare entity. Furthermore, the expanded use of endoscopic ultrasound with fine needle aspiration cytology may possibly spare patients the morbidity of pancreatic biopsy or resection.
Acknowledgements
We thank Daniel C Garcia and Nikolay D Dimov for translating journal articles.
Conflict of interest
The authors have no potential conflicts of interest
References
- Sung SH, Chang JW, Kim J, Lee KS, Han J, Park SI. Solitary fibrous tumors of the pleura: surgical outcome and clinical course. Ann ThoracSurg 2005; 9:303-7. [PMID 15620963]
- Lüttges J, Mentzel T, Hübner G, Klöppel G. Solitary fibrous tumour of the pancreas: a new member of the small group of mesenchymal pancreatic tumours. Virchows Arch 1999; 435:37-42. [PMID 10431844]
- Chatti K, Nouira K, Ben Reguigua M, Bedioui H, Oueslati S, Laabidi B, et al. Solitary fibrous tumor of the pancreas. A case report. GastroenterolClinBiol 2006; 30:317-9. [PMID 16565671]
- Gardini A, Dubini A, Saragoni L, Padovani F, Garcea D. Benign solitary fibrous tumor of the pancreas: a rare location of extra-pleural fibrous tumor. Single case report and review of the literature. Pathologica 2007; 1:15-8. [PMID 17566307]
- Miyamoto H, Molena DA, Schoeniger LO, HaodongXu. Solitary fibrous tumor of the pancreas: a case report. Int J SurgPathol 2007; 3:311-4. [PMID 17652547]
- Sheth S, Fishman EK. Imaging of uncommon tumors of the pancreas. RadiolClin North Am 2002; 6:1273-87. [PMID 12479711] 7. Pauser U, Kosmahl M, Sipos B, Klöppel G. Mesenchymal tumors of the pancreas. Surprising, but not uncommon. Pathologe 2005; 1:52-8. [PMID 15592845]
- Pauser U, Kosmahl M, Sipos B, Klöppel G.
Mesenchymal tumors of the pancreas. Surprising, but
not uncommon. Pathologe 2005; 1:52-8. [PMID
15592845]


