Vishwanath Hesarur*
Department of Cardiology, Jawaharlal Nehru Medical College, KLES Dr Prabhakar ore Hospital and Medical Research Centre, KLE University, Belagavi, Karnataka, India
*Corresponding Author:
Vishwanath Hesarur
Assistant Professor
Department of Cardiology
Jawaharlal Nehru Medical College, KLES Dr Prabhakar Kore Hospital and Medical Research Centre
KLE University, Belagavi, Karnataka
India
Tel: 0831 247 0732
E-mail: drvishwanathhesarur@yahoo.com
Received date: October 25, 2017; Accepted date: November 23, 2017; Published date: November 30, 2017
Citation: Hesarur V (2017) Successful Percutaneous Intervention for Chronic Total Occlusion of Left Subclavian Artery. Interv Cardiol J. Vol.3 No.3:70
Keywords
Subclavian steal syndrome; Percutaneous transluminal angioplasty; Subclavian artery stenosis; Intervention; Atherosclerotic disease
Introduction
Subclavian artery stenosis is most commonly caused by atherosclerotic disease. Stenosis typically occurs in the first part of the subclavian artery proximal to the origin of the vertebral artery extending from the ostium to the origin of the vertebral artery. The incidence of left subclavian artery stenosis is far higher than that of right subclavian artery stenosis.
Intervention is generally reserved for the management of symptomatic patients who present with upper limb ischemia, Vertebrobasilar symptoms and subclavian steal syndrome. Endovascular stenting is preferred over surgery because of high success rate, less invasive and minimal complications. Here we report a case of 56-year-old female patient presented with subclavian steal syndrome that we successfully treated with percutaneous transluminal angioplasty (PTA).
Case Report
A 56-year-old female patient with history of hypertension and diabetes presented with dizziness, vertigo and left arm claudication with use of her left upper extremity since last six months.
Physical examination
Inability to measure BP on left arm with absent left radial pulse and right upper limb BP was 160/80 mmHg. There were no signs of ischemia in left upper extremity.
Investigations
Electrocardiogram showed sinus rhythm with no ST-T changes, transthoracic echocardiography revealed good biventricular function with type 1 diastolic dysfunction. Coronary angiography showed mild single vessel disease. Aortic arch angiography and selective left subclavian angiography revealed total occlusion of left ostio-proximal subclavian artery (Figure 1).
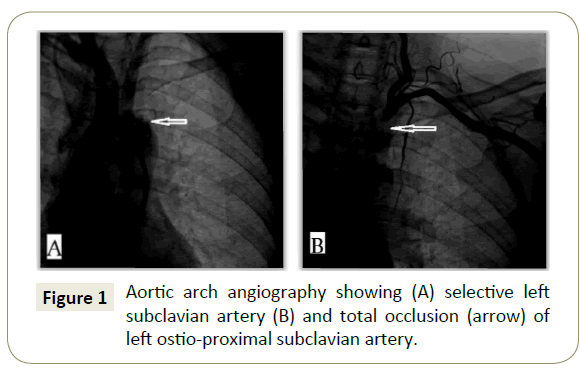
Figure 1: Aortic arch angiography showing (A) selective left subclavian artery (B) and total occlusion (arrow) of left ostio-proximal subclavian artery.
Procedure
The procedure was performed under local anaesthesia. The right femoral artery and left brachial artery were accessed percutaneously with 8F and 6F introducer sheaths, respectively. A preprocedural loading dose of Aspirin 325 mg and 600 mg of clopidogrel was given. Intravenous heparin 100 IU/kg and antibiotic were given.
Ostia of left subclavian artery was engaged by using JR 7F guiding catheter. Check angio showed total occlusion. A 6F shuttle sheath was used to cannulate the vessel and placed distal to the occlusion. The lesion was crossed retrogradely using 0.014 × 190 cm cross-it 200 and placed in proximal descending aorta (Figure 2A). Lesion was predilated using 3.5 × 15 mm balloon at 8 atm pressure (Figure 2B). Check angiogram through JR guiding catheter established good antegrade flow with no dissection (Figure 2C). Using another 0.014 × 180 cm BMW wire crossed the lesion antegradely and the cross-it 200 wire removed (Figure 2D). An 8 × 32 mm INVATEC scuba stent was deployed across ostioproximal subclavian artery (Figure 2E) with a good angiographic result (Figure 2F).
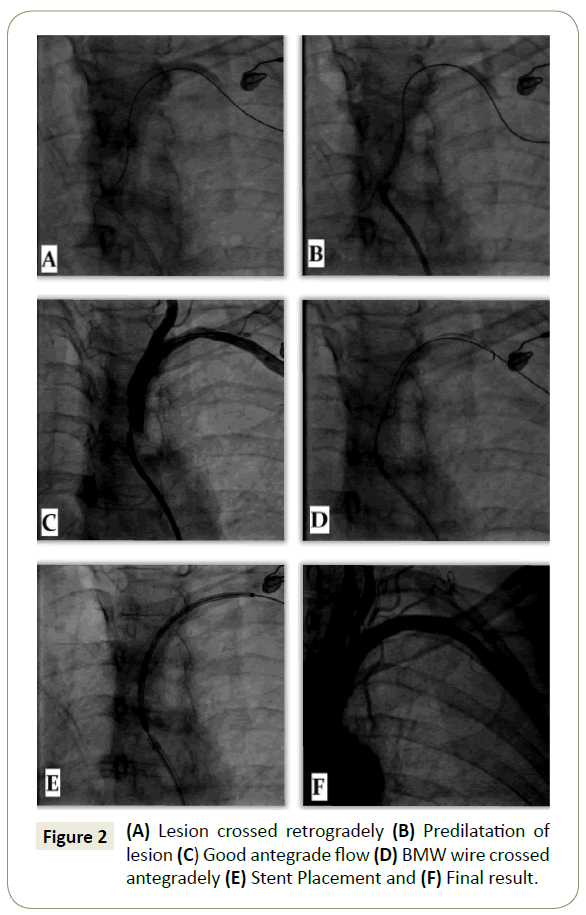
Figure 2: (A) Lesion crossed retrogradely (B) Predilatation of lesion (C) Good antegrade flow (D) BMW wire crossed antegradely (E) Stent Placement and (F) Final result.
Post procedure course was uneventful. The patient was discharged after three days with Aspirin 150 mg OD, Clopidogrel 75 mg BD and Rosuvastatin 20 mg OD.
Follow-up
Patient was followed up at 1, 3, 6 months and one year. Patient reported marked improvement of symptoms. At each visit, patient was monitored with Duplex ultrasound of left subclavian artery, measurement of BP and examination of pulse.
Discussion
Atherosclerosis is the most common cause of subclavian stenosis and, thus, steal syndromes, irrespective of the clinical manifestation [1-3]. However, other causes include large artery vasculitis, thoracic outlet syndrome, and stenosis after surgical repair of coarctation of aorta or tetralogy of Fallot.
The presence of subclavian stenosis is associated with increased total mortality (hazard ratio, 1.40) and cardiovascular disease mortality (hazard ratio, 1.57) [2] and with an increased risk of cerebrovascular ischemic events related to progressive carotid stenosis and compromised collateral pathways. Thus, subclavian artery stenosis is a cardiovascular risk marker and requires aggressive secondary prevention.
Even asymptomatic subclavian artery stenosis is associated with increased risk of morbidity and mortality related to underlying atherosclerotic disease burden in other vascular beds [2-4].
Symptomatic patients with proximal subclavian artery occlusive disease can be successfully treated either surgically or percutaneously [5,6–12].
First case report of subclavian angioplasty was done by Bachman and Kim in 1980 [13]. After this report, percutaneous intervention of subclavian disease has grown persistently, becoming the mainstay of therapy. Balloon angioplasty and stenting can be performed when stenting is unlikely to compromise the vertebral circulation. Technical success of the percutaneous approach can be achieved in >90%, with 5-year patency rates of 85% [12]. Complications during subclavian artery intervention are stroke (< 1%), dissection, access site complications (0% to 5%) like hematoma formation, thrombosis and pseudoaneurysm formation.
The major long-term risk of subclavian artery intervention is restenosis. Stenting appears to have significantly reduced the rate of restenosis, from 15% to 20% with angioplasty to 0% to 10%. The treatment for restenosis will depend on its etiology. Failure to cover the ostium or inadequate stent expansion may be treated with repeat angioplasty and, sometimes, re-stenting. Alternatively, surgical revascularization using an extra thoracic approach (carotid–subclavian, axillo-axillary) is a reasonable option in a symptomatic patient who is an operative candidate.
Conclusion
PTA is an effective and safe with high success rate, less invasive and minimal complications when compared to surgery for the treatment of symptomatic subclavian artery stenosis. However, regular clinical and duplex ultrasound assessment of subclavian artery is necessary after angioplasty for monitoring restenosis.
Conflict of Interest
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
Informed Consent
Written informed consent was obtained from patient for publication of this case report and accompanying images.
References
- Ochoa VM, Yeghiazarians Y (2011) Subclavian artery stenosis: A review for the vascular medicine practitioner. Vasc Med 16: 29-34.
- Aboyans V, Kamineni A, Allison MA, McDermott MM, Crouse JR, et al. (2010) The epidemiology of subclavian stenosis and its association with markers of subclinical atherosclerosis: The Multi- Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 211: 266-270.
- Labropoulos N, Nandivada P, Bekelis K (2010) Prevalence and impact of the subclavian steal syndrome. Ann Surg 252: 166-170.
- Clark CE, Taylor RS, Shore AC, Ukoumunne OC, Campbell JL (2012) Association of a difference in systolic blood pressure between arms with vascular disease and mortality: A systematic review and meta-analysis. Lancet 379: 905-914.
- Rogers JH, Calhoun RF (2007) Diagnosis and management of subclavian artery stenosis prior to coronary artery bypass grafting in the current era. J Card Surg 22: 20-25.
- Babic S, Sagic D, Radak D, Antonic Z, Otasevic P, et al. (2012) Initial and long-term results of endovascular therapy for chronic total occlusion of the subclavian artery. Cardiovasc Intervent Radiol 35: 255-262.
- Burihan E, Soma F, Iared W (2011) Angioplasty versus stenting for subclavian artery stenosis. The Cochrane database of systematic reviews. CD008461.
- De Vries JP, Jager LC, Van den Berg JC, Overtoom TT, Ackerstaff RG, et al. (2005) Durability of percutaneous transluminal angioplasty for obstructive lesions of proximal subclavian artery: Long-term results. J Vasc Surg 41:19-23.
- Filippo F, Francesco M, Francesco R, Corrado A, Chiara M, et al. (2006) Percutaneous angioplasty and stenting of left subclavian artery lesions for the treatment of patients with concomitant vertebral and coronary subclavian steal syndrome. Cardiovasc Intervent Radiol 29: 348-353.
- Salam TA, Lumsden AB, Smith RB (1994) Subclavian artery revascularization: A decade of experience with extrathoracic bypass procedures. J Surg Res 56: 387-392.
- Song L, Zhang J, Li J, Gu Y, Yu H, et al. (2012) Endovascular stenting vs. extrathoracic surgical bypass for symptomatic subclavian steal syndrome. J Endovasc Ther 19: 44–51.
- Wang KQ, Wang ZG, Yang BZ, Yuan C, Zhang WD, et al. (2010) Long-term results of endovascular therapy for proximal subclavian arterial obstructive lesions. Chin Med J (Engl) 123: 45-50.
- Bachman DM, Kim RM (1980) Transluminal dilatation for subclavian steal syndrome. AJR Am J Roentgenol 135: 995-996.

