Lauren Dawes, Animesh Singla*, Steve Chryssidis and Marc Agzarian
Royal Prince Alfred Hospital, Sydney, NSW, Australia
Corresponding Author:
Animesh Singla
Royal Prince Alfred Hospital
Sydney, NSW, Australia
Tel: 0432582925
E-mail: animesh.singla@gmail.com
Received date: July 14, 2017; Accepted date: August 09, 2017; Published date: August 16, 2017
Citation: Dawes L, Singla A, Chryssidis S, Agzarian M (2017) Surpassing Expectations - A Novel Use of Flow Diverting Stent-in- Stent Technique for the Management of a Carotid-Venous Fistula. J Imaging Interv Radiol . Vol. 1 No. 1:1
Keywords
Interventional neurology; Flow-diverting stents; Intracranial aneurysm
Introduction
Flow diverting stents are a new class of neuro-interventional devices for the management of intracranial aneurysms not amenable to conventional techniques [1]. Complications include thromboembolism, intracranial haemorrhage, vessel injury and delayed rupture [2]. Carotid-venous and Carotico-cavernous fistulae (CCF) may result when the aneurysm involves the intracavernous portion of the internal carotid artery (ICA), with rupture resulting in direct communication with the cavernous sinus. Development of such fistulae after flow-diverting stents has only sparsely been reported. This article is the first case report of a carotid-venous fistula in the acute period following treatment with the Surpass flow diverting stent (Stryker, Neurovascular, Fremont, California, USA). It reports a novel ‘stent-in-stent’ technique using a second flow diverting stent to reduce flow through fistula with clinical symptom resolution.
Case Presentation
A 50 year old otherwise healthy male presented with a four month history of severe headaches associated with nausea and progressive visual disturbance. He also reported a chronic history of erectile dysfunction and profound lethargy. Laboratory results were significant for panhypopituitarism.
Investigations
Magnetic Resonance Imaging (MRI) revealed a right internal carotid aneurysm (41 × 34 × 37 mm) with superior elevation and compression of the optic chiasm (Figure 1). Subsequent Computed Tomography Angiography (CTA) delineated a giant fusiform right cavernous internal carotid artery aneurysm (39 × 33 × 37 mm) with mass effect and secondary adjacent bony remodeling (Figure 2). Cerebral angiography demonstrated associated turbulent flow and layering of contrast (Figures 3 and 4).
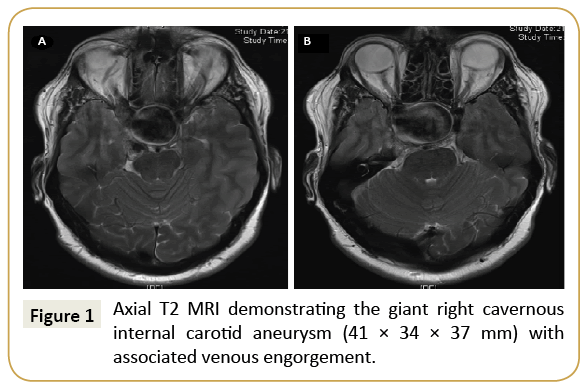
Figure 1: Axial T2 MRI demonstrating the giant right cavernous internal carotid aneurysm (41 × 34 × 37 mm) with associated venous engorgement.
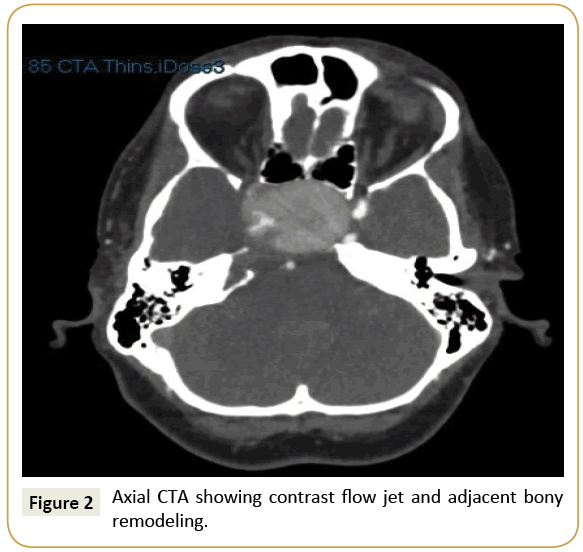
Figure 2: Axial CTA showing contrast flow jet and adjacent bony remodeling.
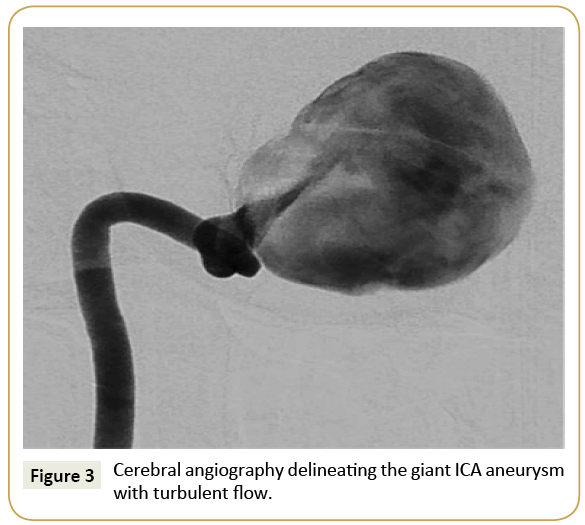
Figure 3: Cerebral angiography delineating the giant ICA aneurysm with turbulent flow.
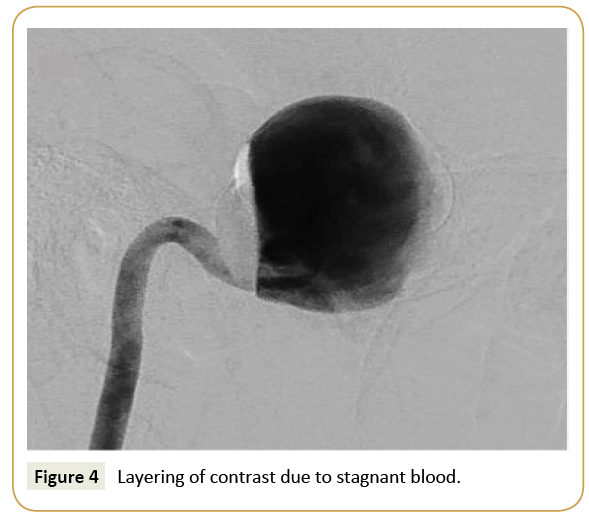
Figure 4: Layering of contrast due to stagnant blood.
Treatment
He underwent endovascular treatment with the use of a flowdiverting stent. He was premedicated with aspirin and clopidogrel. Through the right femoral artery, a Navien 058 access catheter and an XT-27 Micro-catheter were used to successfully access the outflow vessel, deploying a 4 × 40 mm Surpass flow-diverting stent across the aneurysm (Figure 5). The inferior, petrous portion required post dilatation with a 4 × 15 mm balloon with significant improvement in status.
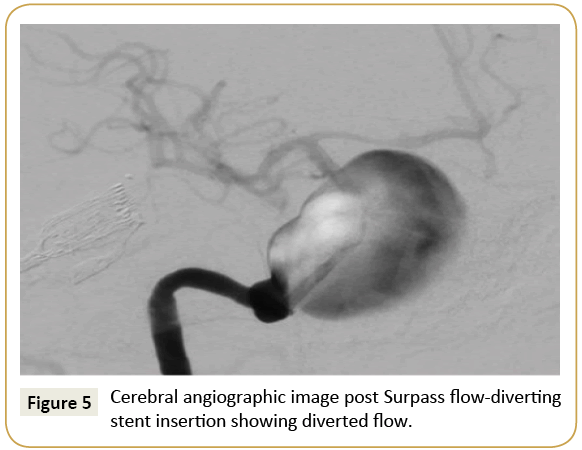
Figure 5: Cerebral angiographic image post Surpass flow-diverting stent insertion showing diverted flow.
Three days post-procedure he developed a cavernous sinus syndrome. Repeat CTA delineated de novo venous pathways through the petrous temporal bone and occipital diploe caused by the aneurysm, with subsequent cavernous sinus region remodeling. Hence it reflected the development of a carotid-venous fistula rather than a conventional carotid cavernous fistula (CCF).
The decision was made for initial conservative treatment to facilitate positive remodeling with stent endothelialisation and aneurysm thrombosis. One month post-procedure, due to ongoing symptoms, trans- venous embolization was attempted. The right common femoral vein was used to access the right internal jugular vein at the level of the skull base. This attempt was aborted due to difficulty negotiating the fistulated venous plexus.
Despite progressive aneurysm thrombosis and reduction in flow through the fistula, the patient continued to experience disabling pulsatile tinnitus. After multidisciplinary discussion, and given the previously attempted embolization a decision was made to attempt arterial correction of the carotid-venous fistula. The right common femoral artery was accessed and a Navien 035 was used to traverse the existing stent. A Surpass Streamline 3 × 25 mm flowdiverting stent was placed across the fistulating zone of the initial stent (Figure 6). An 8Fr Neuron Max sheath was positioned at the right ICA, and a Navien 035 was used to traverse the existing stent.
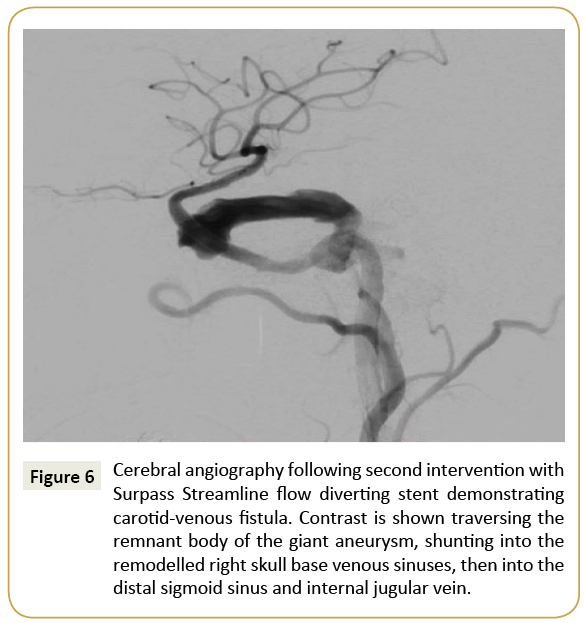
Figure 6: Cerebral angiography following second intervention with Surpass Streamline flow diverting stent demonstrating carotid-venous fistula. Contrast is shown traversing the remnant body of the giant aneurysm, shunting into the remodelled right skull base venous sinuses, then into the distal sigmoid sinus and internal jugular vein.
Outcome and Follow-Up
Post-procedure there was complete resolution of his pulsatile tinnitus and a gradual resolution of his right cavernous sinus syndrome over the ensuing three months. He continued dual antiplatelet therapy for twelve months, and at 18 months, repeat imaging (Figures 7 and 8) showed collapse of the aneurysm with scant residual flow. The patient remains neurologically intact and it is anticipated that ongoing remodeling will result in complete resolution.
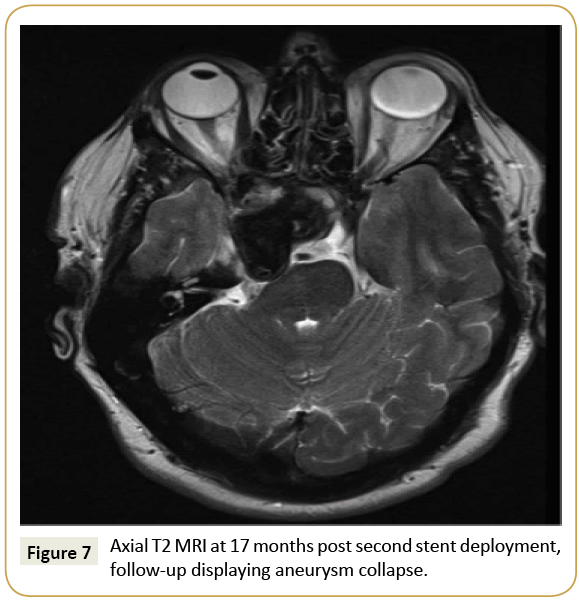
Figure 7: Axial T2 MRI at 17 months post second stent deployment, follow-up displaying aneurysm collapse.
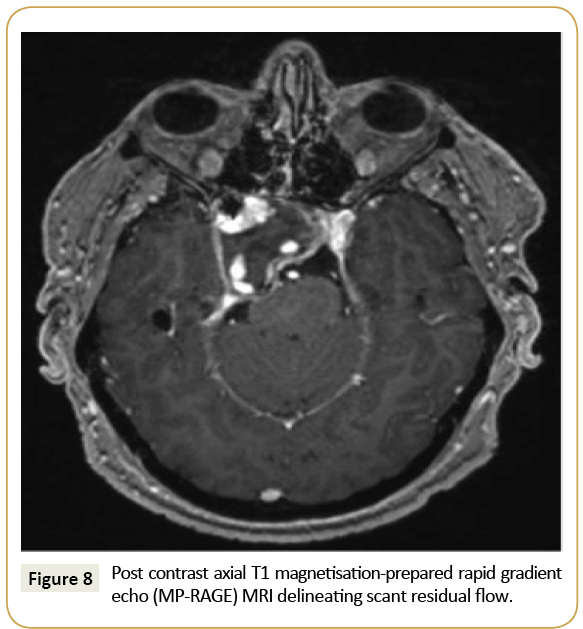
Figure 8: Post contrast axial T1 magnetisation-prepared rapid gradient echo (MP-RAGE) MRI delineating scant residual flow.
Discussion
The Surpass Streamline is a cobalt-chromium, low porosity, selfexpanding flow-diverting stent undergoing clinical evaluation for use in treatment of intra-cranial aneurysms [3]. Caroticocavernous fistulae (CCF) and carotid-venous fistulae are rare complications of flow diverting stents, with few documented cases. Presentation ranges from 3 to 110 days post intervention [4- 10]. Two underlying mechanisms leading to negative remodeling have been proposed. Progressive aneurysmal thrombosis can cause intramural inflammation and an inflammatory state with chemical degradation and aneurysm wall degeneration [9].
Secondly flow diverting stents have been shown to alter aneurysm wall haemodynamics, animal and in vitro studies suggesting they can lead to increased stress to areas of the aneurysm not previously under strain [8]. The diversion of blood flow to a distal parent artery with higher resistance and changes in cerebral autoregulation are also thought to play a role [9].
The goal of endovascular treatment of Carotid-venous and carotico-cavernous fistulae is to maintain ICA patency whilst occluding the pathological communication. Options include trans-arterial obliteration through embolization, transvenous coiling of the cavernous sinus or parent artery ligation [5,11]. The use of flow diverting stents to manage these has only recently been reported. Six cases in the literature exist [4-9]. Majority report the use of trans-arterial flow diversion concurrently with transvenous embolization. Nadarajah et al. [10] described posttraumatic right CCF treated successfully with telescoping four Pipeline embolization devices (PED; Covidien, Mansfield, MA, USA). Amuluru et al. [4] described a similar technique to manage post-flow diverting stent CCF.
This is the first case that uses the Surpass and Surpass Streamline flow-diverting stents for treatment of a carotid-venous fistula. The aim was to increase metallic coverage and minimise porosity in a segment of aneurysm with fistulous communication. The Surpass stent has a metallic coverage of approximately 30%; by placing overlapping stents it created a strong scaffold which would then endothelialise, maximising the chance of successful fistula closure [2]. The main drawback to this technique, similar to other flow diverting stents, is the need for dual antiplatelet therapy due to risk of in-stent thrombosis. This needs to be balanced against risk of further haemorrhage in context of a carotid-venous fistula.
References
The goal of endovascular treatment is to maintain ICA patency whilst occluding the pathological communication. A stent-in-stent technique utilizing Surpass and Surpass Streamline flow-diverting stents are a viable treatment option in certain cases. Further clinical evaluation is required in these novel endovascular devices.
Conflict of Interest
I, Animesh Singla, the corresponding author, on behalf of all other authors do not report any conflict of interest.
Patient consent was obtained prior to preparation of this manuscript and for dissemination of all imaging.
References
- Alderazi Y, Shastri D, Kass-Hout T, Prestigiacomo C, Gandhi C (2014) Flow diverters for intracranial aneurysms. Stroke Res Treat 2014: 1-12.
- Tan L, Sandler V, Todorova-Koteva K, Levine L, Lopes D, et al. (2014) Recovery of pituitary function following treatment of an unruptured giant cavernous carotid aneurysm using surpass flow-diverting stents. BMJ Case Rep 33.
- Colby G, Lin L, Caplan J, Jiang B, Michniewicz B, et al. (2016) Flow diversion of large internal carotid artery aneurysms with the surpass device: impressions and technical nuance from the initial North American experience. J Neurointerventional Surg 8: 279-286.
- Amuluru K, Al-Mufti F, Gandhi C, Prestigiacomo C, Singh I (2016) Direct carotid-cavernous fistula: A complication of and treatment with, flow diversion. Interv Neuroradiol 22: 569-576.
- Lin L, Colby G, Jiang B, Pero G, Boccardi E, et al. (2014) Transvenous approach for the treatment of direct carotid cavernous fistula following Pipeline embolization of cavernous carotid aneurysm: A report of two cases and review of the literature. Case Rep 2014: 35.
- Park S, Albuquerque F, Nanaszko M, Sanborn M, Moon K, et al. (2015) Critical assessment of complications associated with use of the pipeline embolization device. J Neurointerventional Surg 7: 652-659.
- Becske T, Kallmes D, Saatci I, McDougal C, Szikora I, et al. (2013) Pipeline for uncoilable or failed aneurysms: Results from a multicenter clinical trial. Radiology 267: 858-868.
- Kulczar Z, Houdart E, Bonafe A, Parker G, Millar J, et al. (2010) Intra-aneurysmal thrombosis as a possible cause of delayed aneurysm rupture after flow-diversion treatment. Am J Neuroradiol.
- Mustafa W, Kadziolka K, Anxionnat R, Peirot L (2010) Direct carotid-cavernous fistula following intracavernous carotid aneurysm treatment with a flow-diverter stent. A case report. Interv Neuroradiol J Peritherapeutic Neuroradiol Surg Proced Relat Neurosci 16: 447-450.
- Nadarajah M, Power M, Barry B, Wenderoth J (2012) Treatment of a traumatic carotid-cavernous fistula by the sole use of a flow diverting stent. J Neurointerv Surg 4: e1.
- Cebral J, Mut F, Raschi M, Scrivano E, Ceratto, et al. (2010) Aneurysm rupture following treatment with flow-diverting stents: computational hemodynamics analysis of treatment. Am J Neuroradiol 32: 27-33.
