Keywords
Lymph Nodes; Neoplasm Staging; Pancreatic Neoplasms; Surgery; Survival
Note Some references [19, 20, 22, 23, 25, 26, 27, 35, 36, 37, 39, 44, 48, 54, 55, 58, 59, 61, 63, 65, 68, 72, 73, 87, 88, 94, 96, 99, 104, 110, 111, 117, 119, 122, 125, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 141, 143, 144, 145, 147, 148, 150, 151, 152] are not discussed fully in the text because the data presented in the studies were not of a format which would allow any further analysis, other than the calculation of postoperative mortality, overall long-term survival and median survival. These references (plus the majority of the other references in the review) were used to generate the median post-operative survival, mortality rate and 1-, 2-, 3-, and 5-year survival rates, reported at the beginning to the results section under the heading literature search.
INTRODUCTION
Patients with resectable pancreatic cancer comprise a small subgroup of the overall population with the disease from around 15 to 20% [1]. The long term survival of patients is appalling, with nearly all patients dying from their disease within 7 years of surgery [2, 3, 4]. In the light of such bleak statistics, data regarding what factors may influence outcome, following attempted curative resection is essential in order to optimise the treatment options for patients.
METHODS
This review analysed all English-language publications using PubMed and Web of Science databases for studies detailing outcomes following resection for pancreatic ductal adenocarcinoma, from 1980 to the present day. The data examined from papers were post-operative mortality rates, median survival, yearly survival rates and other factors which may have influenced long-term survival; such as patient demographics, operative details and tumour characteristics (such as tumour size, lymph node metastases and tumour differentiation). When feasible, data derived from survival curves was included in the analysis. All the information examined related to pancreatic ductal adenocarcinoma only. Manuscripts which did not offer a differential breakdown between ductal adenocarcinomas and other cancers, such as periampullary tumours, distal cholangiocarcinoma and pancreatic endocrine tumours, were excluded from the review. Studies which described only outcomes following major vessel resection and reconstruction in addition to pancreatic resections were also excluded.
STATISTICS
Statistical analysis was undertaken using the Student’s t-test, Mann-Whitney and ANOVA with GraphPad Prism version 3.00 for Windows (GraphPad Software, San Diego, CA, USA). Where appropriate, a metaanalysis of data was undertaken using a random effects model with Comprehensive Meta-Analysis software (Biostat, Englewood, NJ, USA). Two-tailed P values than 0.05 were considered significant.
RESULTS
Literature Search
A total of 154 studies detailing outcomes following resection for 25,930 patients were included in the study. Due to variations in reporting and the number of studies published, a greater number of more recent studies were applicable for this study when compared to earlier publications. Per decade there were 74 studies from 2000 to the present day [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78], 52 studies from 1990 to 1999 [2, 3, 4, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127], 25 studies from 1980 to 1989 [128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152] and only 3 studies dating from before 1980 [153, 154, 155]. The median post-operative survival was 15.8 months with an operative mortality rate of 4.1%. The median one-year, two-year, threeyear and five-year survival rates across all studies (from all decades) were 63.3%, 36.0%, 22.5% and 12.0%, respectively.
Evolution of Surgical Pratice and Sub- Specialisation
Postoperative Mortality and Survival across the Decades
There has been a marked reduction in the post-operative mortality rate following pancreatic resection across the four decades examined by this review from being as high as 25% before 1980 to 2.9% from 2000 onwards (Figure 1) (P<0.001). This finding is reflected in single-institution reports examining post-operative mortality and the year of resection. Crucitti et al. observed a reduction in morbidity and mortality from 55.6% and 16.7% respectively to 20% and 6.7% across the time periods of 1981 to 1987 and 1993 to 1995 [85]. Yuen et al. found that their post-operative mortality fell from 10.7% from 1995 to 1997 to 2.3 from 1997 to 2000 [45].
Figure 1. Post-operative mortality rate and median
survival following resection for pancreatic ductal
adenocarcinoma across four decades (P<0.001 for
mortality decrease).
Winter et al. [17] reported remarkably similar mortality rates in their series of 1,423 pancreatic resections, to those observed by us across all studies, 30% from the 1970s, 5% from the 1980s, 2% and 0% from the 1990s and 2000s respectively, although this data incorporates non-ductal adenocarcinoma resections. The decreased morality seen following resection is most likely to be a corollary of increasing specialisation, centralisation of “Hepatobiliary” and “Pancreatic” services to dedicated units and improved pre-operative and post-operative care.
In spite of this marked improvement in postoperative mortality, median survival following resection appears unchanged (Figure 1). However, cumulative 1-, 2-, 3- and 5-year survival across these time points show an increase in the number of 5-year survivors from 1990 onwards, when compared to pre- 1990 reported survival rates. The percentage of 5-year survivors reported from studies from after 1990 being significantly greater than those from before this time interval (P<0.001). Single-centre reports examining survival across decades, such as Yeo et al. [109], have reported an improved median survival (17.5 months versus 7.5 months, respectively ) and improved 1- and 3-year survival rates (64% and 36% versus 32% and 14%) from resections undertaken in 1990s compared with those from the 1970s. Other studies have found improved five year survival (11% versus no survivors) from resections undertaken in 1990s compared to those from the 1970s [56].
Impact of Centralisation of Services and High-Volume HPB Units
Seventeen papers examining the impact of centralisation and high-volume units on pancreatic cancer resection results were identified from 1997 to 2006. Interpretation of the results across these studies requires some caution since some studies have analysed their results based on the volume of patients referred or treated by each centre, with delineation being made between high-volume and low-volume centres. Other reports have merely classified centres as “teaching” or “non-teaching” hospitals or “university” hospitals.
The majority of these papers have individually found a lower post-operative mortality following resection in a high volume/teaching hospital when compared to low volume centres (median mortality across all studies 5.5% versus 11%, respectively). The data is summarised in Table 1 [16, 21, 38, 46, 47, 49, 57, 93, 113, 156, 157, 158, 159, 160, 161, 162, 163]. Since 1979 it has been proposed that surgical volume impacted on mortality [164] and that this inverse relationship between hospital volume and mortality is most marked for high-risk procedures such as pancreaticoduodenectomy [165]. These findings are consistent with this notion. A detailed systematic review of hospital volume and mortality for pancreatic resection undertaken by van Heek et al. found that mortality rates were as high as 16.5% in hospitals undertaking less than 5 pancreatic resections annually, compared to 3.5% in those doing 24 or more [166].
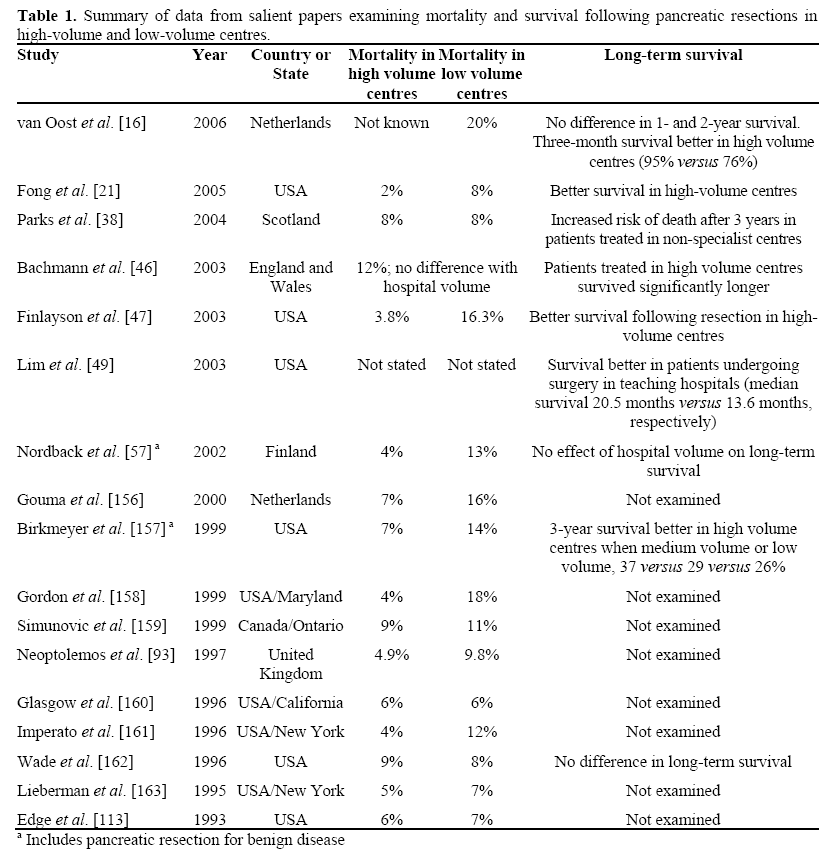
Although most of the earlier studies concentrated on variation in post-operative mortality and complications, more recent studies have examined the impact of highvolume centres on long-term survival following pancreatic resection. The data suggest that long-term survival is improved in hospitals with a higher volume (summarised in Table 1). In addition, treatment in specialist referral centres results in other benefits such as increased probability of resection, increased probability of pre-operative staging laparoscopy and increased probability of cytological confirmation of diagnosis [46].
Summary
In summary, there is clear evidence of improved post-operative mortality following pancreatic resection from 1970 to the present day. Whilst overall median survival has not changed, there is evidence of improved 5-year survival rates from 1990 onwards. Treatment in high volume specialist centres appears to result in a decrease in post-operative mortality and better long-term survival when compared to low-volume centres.
Gender, Age and Socioeconomic Status
There appears to have been little change in the demographics of patients undergoing resection of the pancreas for cancer over the years. The proportion of male gender patients and percentage of patients over 65 years of age, show no significant change over time [8, 13, 14, 30, 42, 43, 49, 50, 53, 66, 69, 70, 76, 80, 109, 114, 120, 124]. It is interesting to note that the proportion of elderly patients (i.e. aged over 65 years) does not appear to be increasing, in spite of significant improvements in the safety of pancreatic surgery over the same time period. There are reports of large series of pancreatic resections (n=287) of patients aged 80 or above years of age [167] which, in spite of slightly higher mortality rate than in younger patients (4.1% versus 1.7%), have shown that resections can be performed with a tolerable mortality in the very elderly. However, this approach does not appear to have been widely adopted.
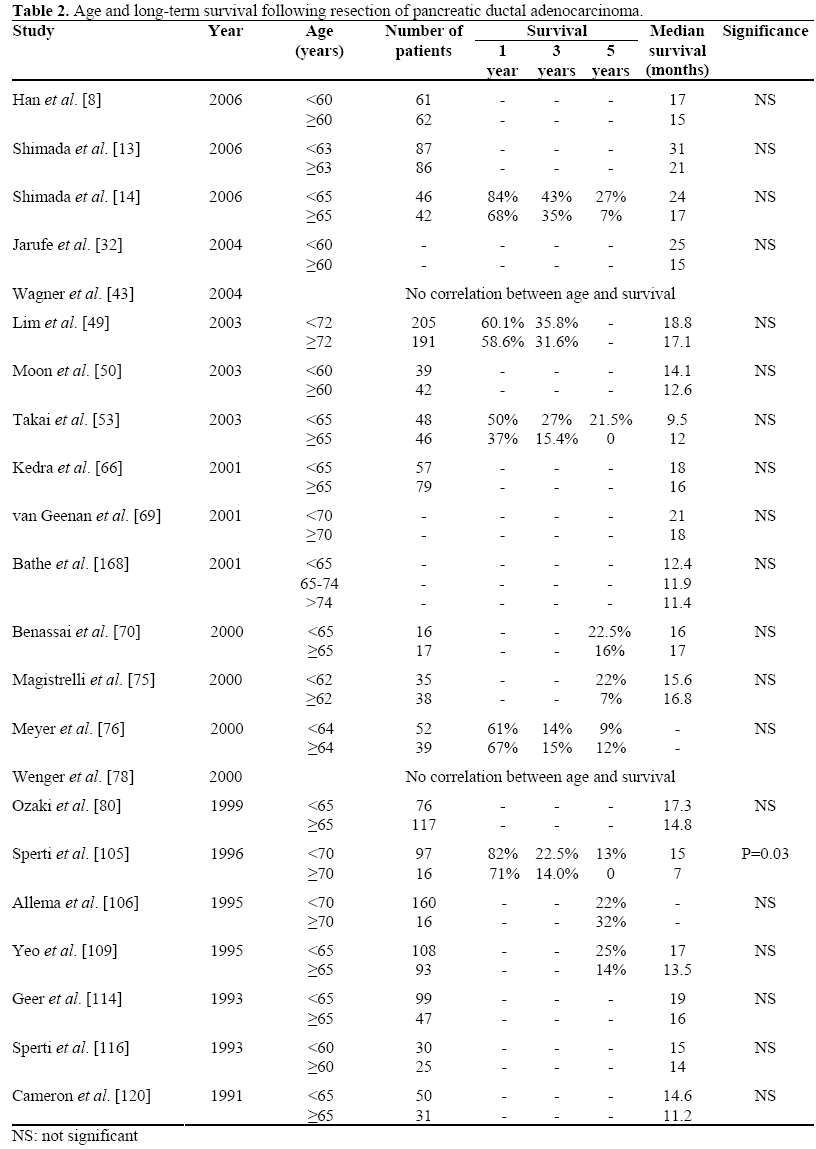
Age and Survival
Twenty-two studies reporting on age and survival following pancreatic cancer resection were identified. A summary of the pertinent findings is displayed in Table 2 [8, 13, 14, 32, 43, 49, 50, 53, 66, 69, 70, 75, 76, 78, 80, 105, 106, 109, 114, 116, 120, 168]. Only one study in the table found age to be a significant prognosticator for long-term survival [105], but the numbers in this study were relatively small. Another report examining resections from non-cystic epithelial pancreatic cancers (hence not included in the table) also concluded that patients aged over 74 years of age had a shorter median survival than those aged 65 to 74 years of age (11.4 months versus 25.1 months) [169].
Gender and Survival
Twenty studies reporting on gender and survival were identified [8, 10, 13, 14, 30, 42, 43, 49, 53, 66, 69, 70, 76, 80, 106, 109, 114, 116, 120, 124]. None of these studies reported that gender was associated with any variation in survival.
Socioeconomic Status, Ethnicity and Survival
The separation of socioeconomic status from ethnicity particularly in some countries, such as the US, can be fraught with difficulty; therefore the two are probably best discussed together. There is a relative paucity of data regarding the impact of these factors on survival from resected pancreatic malignancy. A total of four studies were identified which examined the effect of race and socioeconomic status. Cress et al. and Yeo et al. found no effect of race on outcome following resection [6, 109]. However, Lim et al. observed a significantly shorter median survival between African American and non- African American (10.3 months versus 18.3 months, respectively) [49]. In addition, they reported a strong trend towards better survival in patients with a higher-than-average income, which become significant on multivariate analysis.
Population-based studies have shown that African American patients had a higher risk of presenting with advanced-stage disease and unresectable tumours with a lower probability of receiving chemotherapy and/or surgery. The exact impact of cultural attitudes and of healthcare influencing these findings is difficult to elucidate. For example, Elubeidi et al. found a greater proportion of African Americans refused their respective therapies when compared to their white counterparts [169].
Bathe et al. reported a median survival of only 11.4 months in Hispanics undergoing resection compared to 21.7 months in non- Hispanics (P=0.009) [64, 168]. The causes of this are not immediately clear, since Hispanic patients had the same rates of resection as non-Hispanics and presented with similarstage disease. These are interesting findings which would require robust investigation to determine if there is an independent relationship between outcome following resection and ethnicity, or whether the results observed are a complex interplay of racedependent expectations, financial status and provision of healthcare.
Summary
It appears unlikely that age or gender have any impact on survival following pancreatic resection, since the overwhelming majority of papers reviewed show no evidence of any prognostic value. Factors leading to ethnic or class disparity and survival following resection for pancreatic cancer warrant further work, but no firm conclusions can be made at this time.
Pre-Operative Haematology and Biochemistry
Tumour Markers
Ten studies examining various tumour markers and survival following resection for pancreatic adenocarcinoma were found, principally CA 19-9. Three studies relied on the post-operative progression of the tumour marker and outcome, and hence were not applicable for this review. The results of those excluded studies found that normalisation of the levels of CA 19-9 were associated with improved disease-free survival and better overall survival [170, 171, 172].
Of the remaining studies, huge variations exist between the cut-off points used for analysis from above or below 1,000 or 100. Combined with variations in data presentation and reporting, this precludes detailed analysis of the results. Table 3 provides a suitable overview [7, 8, 14, 40, 53, 173, 174]. Overall, the results are inconclusive with studies equally split between those finding tumour markers such as CA 19-9 able to predict outcome and those reporting no statistically significant association. It is probable that the trend in tumour marker value post-operatively is of greater value in predicting outcome rather than a single reading at the time of surgery. In addition, tumour markers are an index of tumour burden, hence many patients eligible for resection surgery have low tumour burdens and thus more sensitive indices of tumour volume are needed. Yamaguchi et al., for example, reported no significant difference in CA 19-9 or CEA values between patients with large or small tumours undergoing resection surgery [82] (this study did not present tumour marker data in the context of survival following resection and so was not included in Table 3).
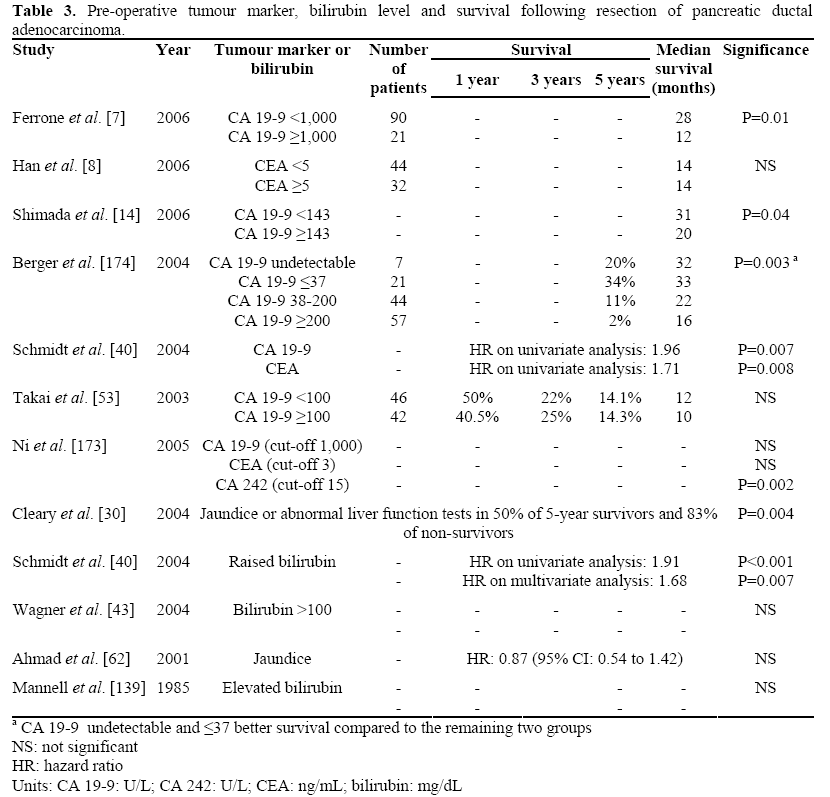
Bilirubin Level
With regards to long-term survival only two of the five studies reviewed reported a deleterious effect on survival in patients with a raised bilirubin (Table 3) [30, 40, 43, 62, 139]. Intuitively it is difficult to postulate how a raised bilirubin pre-operatively could impact on long-term survival following pancreaticoduodenectomy, except as an obtuse indicator of tumour size. Alternatively, peri-operative stenting may contribute to immediate postoperative mortality secondary to sepsis or impede oncological resection by obscuring tissue planes with oedema and inflammatory changes. There are few data to suggest that stenting per se increases risk following pancreaticoduodenectomy [175], particularly in the absence of positive bile cultures [176]. Although, data from small series do suggest that a raised bilirubin increases morbidity and mortality following surgery [146, 149].
C-Reactive Protein and Platelet Count
Other serum parameters examined in the context of long-term outcome following pancreaticoduodenectomy include C-reactive protein (CRP), glucose levels [40] and platelet count. There are too few studies to make a reasoned conclusion as to the validity of these findings, but the results are of interest and are discussed below. Jamieson et al. reported a median survival of 21.5 months in patients with a CRP of less than 10 versus a median survival 8.5 months in those patients with a CRP greater than this [24]. It is likely that CRP is a measure of tumour burden and indeed levels are significantly higher with increased tumour size and the degree of dedifferentiation [24].
Platelets are thought to interact with tumour cells and endothelial cells and to participate in both angiogenesis and haematological metastases. Platelets are also raised in inflammatory processes, such as those found with carcinogenesis. Hence, increased platelets could correlate with survival as a function of tumour burden and metastatic potential. Two English-language papers have reported significantly lower survival in patients with a thrombocytosis. Brown et al. reported a median survival of 18.6 months in patients with platelets below 300 x109/L and 11.2 months with platelets above 300 x109/L (P=0.034 on univariate analysis and P=0.007 on multivariate analysis) [18]. Suzuki et al. found that a thrombocytosis with platelets of over 400 x109/L was associated with diseasefree survival of 4.9 months versus 46.5 months in those with a normalised platelet count [41]. These findings merit further investigation and validation.
Summary
It is likely that serum tumour markers are not sufficiently sensitive to accurately predict prognosis at the time of resection, although serial post-operative markers may be more exact. There is evidence that pre-operative bilirubin levels, CRP and platelet counts may predict prognosis in a similar way to tumour markers, by serving as index of tumour burden and/or aggressiveness. There is emerging evidence that raised platelet counts and CRP could be strongly linked to adverse outcome, but more data is required.
Intraoperative Factors
Operation Duration
Five studies were found examining duration of operation with survival following pancreaticoduodenectomy [43, 53, 75, 109, 114]. No definite conclusions can be drawn from the data. It seems likely that duration of operation would be related, in some part, to tumour size and this could explain the observations from some studies that the period of surgery was associated with poorer survival. However, it is difficult to see how this data, if borne out by other studies, could be applied in a clinical setting in predicting or improving survival.
Blood Loss
Thirteen papers reported on intraoperative blood loss and transfusion requirements in pancreatic cancer resection (Table 4) [8, 40, 43, 49, 50, 53, 66, 75, 77, 105, 106, 114, 120]. The data presented varies from units transfused to actual blood loss intraoperatively, hence severely limiting the number of studies included in the metaanalysis. Studies included in the metaanalysis were those reporting median survival and yearly survival for the cut-off points of less than 2 units or more than 2 units of blood transfused. Meta-analysis of 1-, 3- and 5-year survival data did not reveal a significant trend towards transfusion affecting survival (OR=0.84, 95% CI: 0.52-1.37; P=0.484) (Figure 2). However, on analysis of the median survival data, transfusion of less than 2 units was found to favour prolonged survival (OR=1.83, 95% CI: 1.04-3.24; P=0.037).
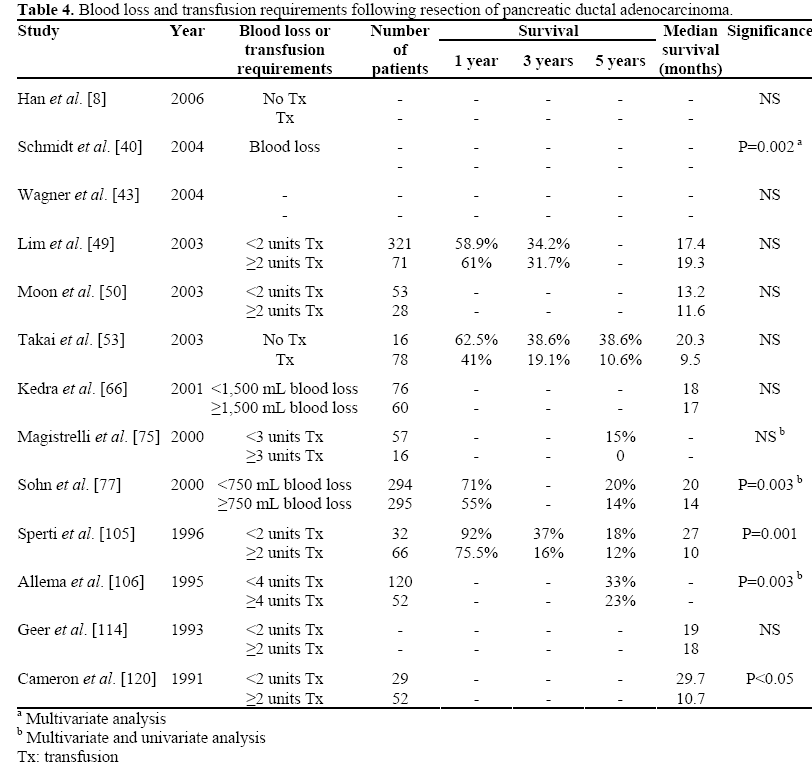
Figure 2. Forrest plot of median survival data and 1-,
3-, 5-year survival following blood transfusion in
pancreatic cancer resections.
There are several possibilities on how intraoperative blood loss and blood transfusion may impact on long-term survival.
It is conceivable that technically difficult operations, due to large tumours or adherent tumours, will be accompanied by greater blood loss and hence post-operative transfusion requirements. However, three of the examined studies found that blood loss/transfusion requirements were independently prognostic [40, 105, 106]. Allogenic blood transfusions have been postulated to induce host immunosuppression, as evidenced by increased renal graft survival following transfusions [177, 178, 179]. This immunosuppression following cancer resections could result in increased probability of recurrence. A number of papers examining survival and blood transfusion for a wide range of oncological surgery have reported on this, although as yet it has not been definitively proved by a randomized controlled trial or meta analyses [180].
The nature of pancreatic surgery precludes the complete elimination of blood transfusion, although it would be prudent to minimise transfusion requirements, particularly in light of the data supporting the possibility of a deleterious impact on survival. There are various means by which this could be achieved, including a much higher threshold for transfusion, the use of white cell filters when transfusing, although this is a costly process without proven success [180], or the use of autologous blood transfusion. It must be stressed that a recent study of autologous versus allogenic blood transfusion, during colorectal cancer surgery, found no improvement in recurrence rates or survival [181].
Location of Tumour
There was wide variation in the homogeneity of data examining tumour location and survival, with some studies reporting on the type of resection i.e. distal pancreatectomy or pancreaticoduodenectomy (Table 5) [10, 14, 30, 43, 49, 66, 75, 77, 80, 97, 105, 107, 109, 116, 120, 124]. Furthermore, not all authors distinguished between distal pancreatectomies or pancreaticoduodenectomies, reporting between partial or total resections instead. In spite of this spectrum of data reporting, only one study found tumour location to be of significance in prognosis. It is of note that the same authors in a follow-up study several years later in a larger cohort of patients, no longer found that tumour location factored in survival following resection [105, 116].
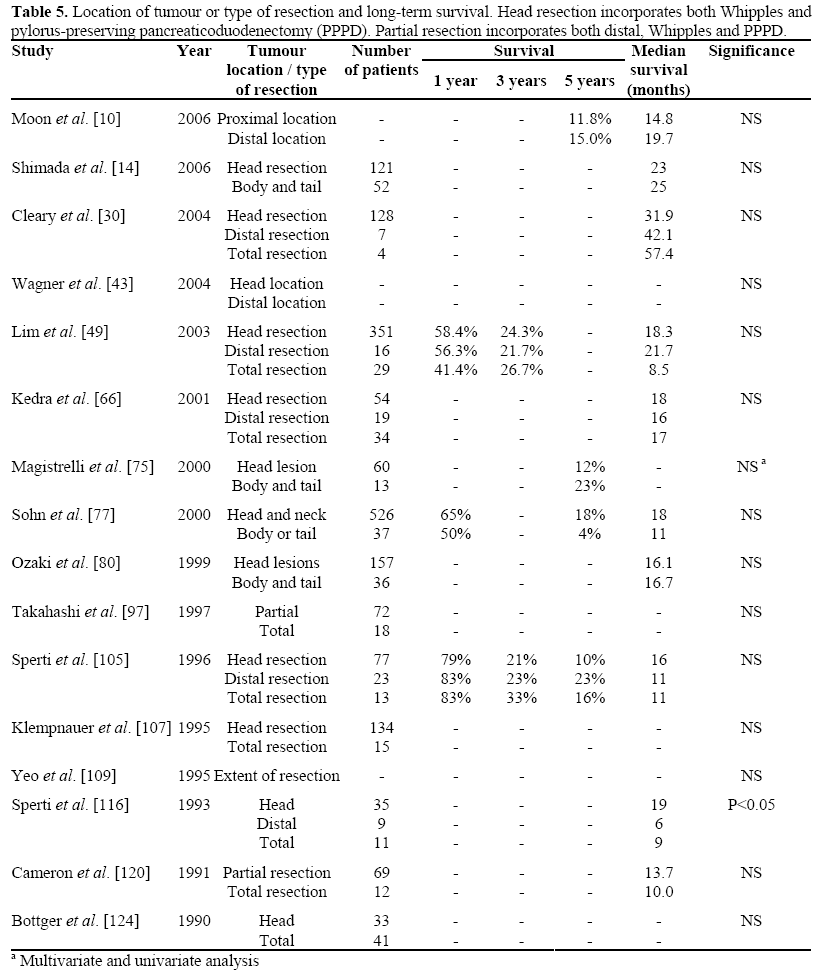
There are obvious risks to inferring where tumours are located according to the type of resection undertaken. However, it would be reasonable to assume that most recorded distal pancreatectomies would be undertaken for tumours located in the pancreatic tail, and most proximal pancreatectomies for those in the head. There is one further caveat to add to the assumption that location plays no part in outcome. Sohn et al. report significantly larger diameter in distally positioned tumours when compared to pancreatic head lesions (3.9 cm versus 3.0 cm, respectively [77]). A differential breakdown in tumours sizes was not available in the other papers reviewed. However, such a finding does raise the possibility that distal cancers have an equal survival to proximally placed cancers in spite of being larger at the time of resection. Despite these reservations, currently the evidence presented strongly suggests that tumour location is not a factor in long-term survival following ductal adenocarcinoma resection.
Summary
Duration of operation has been reported by some studies to relate to long-term survival following curative resection for pancreatic ductal adenocarcinoma, although no study has found this to be a significant prognosticator on multivariate analysis. Both intraoperative blood loss and units transfused have been found to predict long-term survival on univariate, multivariate analyses and metaanalysis. This finding could be multifactorial in nature, partly attributable to higher bloodloss operations being associated with bigger and larger cancers, and secondary to a transfusion mediated immune-suppression. Finally, the current evidence does not suggest that tumour location affects survival.
Tumour Characteristics
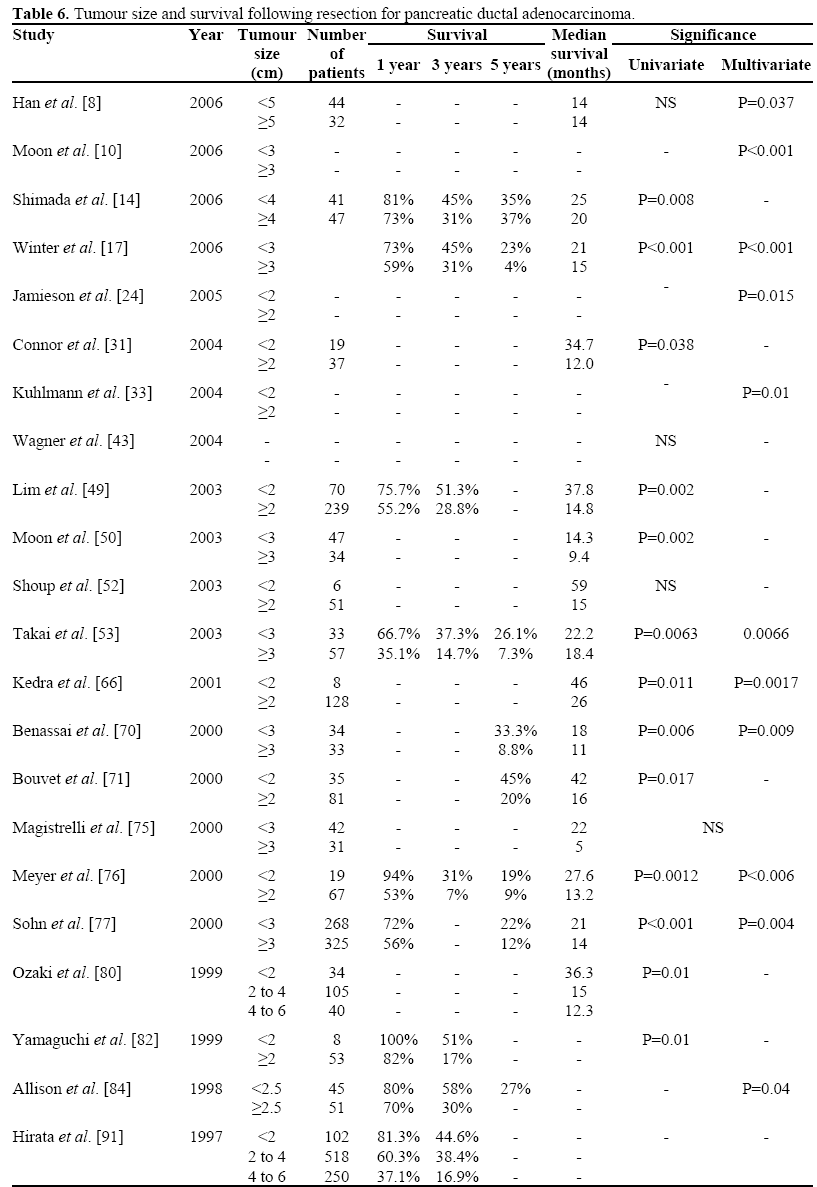
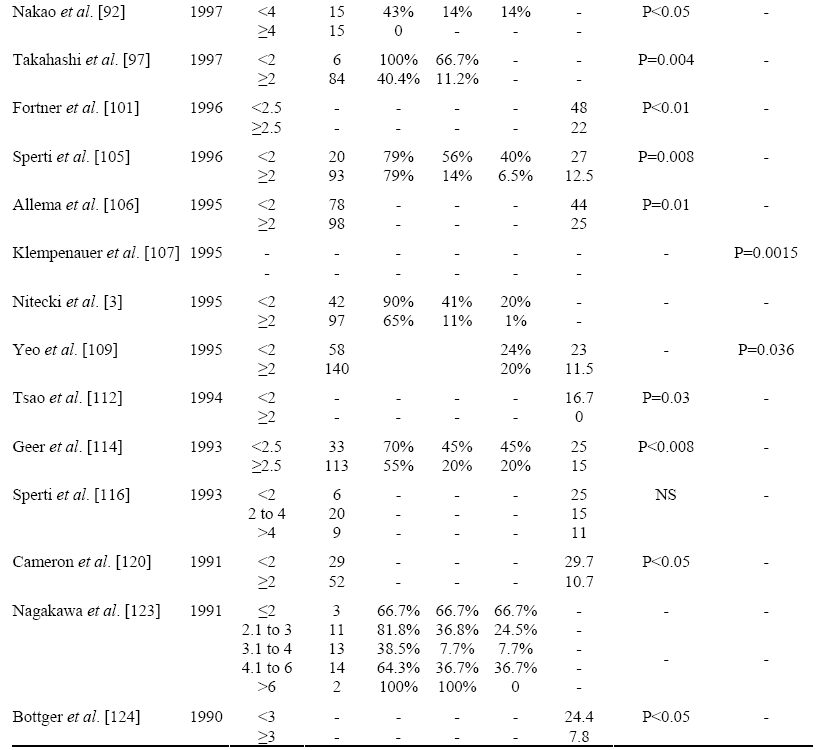
Tumour Size
Many studies reviewed did not report median tumour size for their series, instead reporting tumour sizes as greater or less than a fixed diameter. Figure 3 displays the proportions of tumour size resected from these studies. Those studies that report a median tumour diameter normally quote it as between 3.0 to 3.5 cm [15, 95].
Figure 3. Median proportion (expressed as percentage)
of resected tumour sizes. N value refers to the number
of studies from which data was derived. For tumours
greater than 5 and 6 cm, the number of studies found
reporting this data was only one each, therefore bars
are shown cross-hatched.
Table 6 [3, 8, 10, 14, 17, 24, 31, 33, 43, 49, 50, 52, 53, 66, 70, 71, 75, 76, 77, 80, 82, 84, 91, 92, 97, 101, 105, 106, 107, 109, 112, 114, 116, 120, 123, 124] summarises data from all studies comparing tumour size with outcome following resection. It can be clearly seen that most studies report a significant association with tumour size and prognosis, on either multivariate or univariate analysis. Figure 4 summarises the median of the median survivals reported by the studies in Table 6 for varying cut-off points of tumour size. The data represented in this format strongly suggests that tumour size affects survival, with the greatest impact seen in resected tumours below 2 cm in size (35.5 months versus 14 months). Although it has to be noted that for larger tumour sizes the number of studies found were fewer, falling to just one study reporting median survival for tumours above or below 5 cm. Meta-analysis of yearly survival rates and median survival for tumours less than 2 cm or greater than 2 cm in size revealed that tumours less than 2 cm are associated with a better survival (OR=0.32, 95% CI: 0.18-0.56; P<0.001, and OR=2.52, 95% CI: 1.95-3.29; P<0.001, respectively) (Figure 5).
Figure 4. Cross-study median value for survival from
studies reporting median survival and tumour size. N
value refers to the number of studies from which data
was obtained.
Figure 5. Forrest plot of median survival data and 1-,
3-, and 5-year survival and tumour size in pancreatic
cancer resections.
There are several possible ways by which larger tumours negatively impact on survival. The effect could be temporal in that larger tumours have an increased probability of micro-metastases and lymphatic spread at the time of surgery, due to their long-term presence. It may be that larger cancers reflect a more aggressive phenotype in fastergrowing de-differentiated tumours. Obtaining suitable oncological clearance with larger tumours could also contribute to decreased survival. However, the recent ESPAC data found that microscopic tumour involvement of the resection margin was not associated with tumour diameter [67]. There is evidence that tumours less than 2 cm in diameter have a greater probability of being clear of lymph node involvement, are better differentiated and have less perineural involvement than larger tumours [82]. Patterns of recurrence following pancreatic cancer resection also suggest that local recurrence is not the most common cause of death and that most deaths are secondary to systemic dissemination of disease, in the form of hepatic and lymphatic metastases [182]. This would suggest that tumour diameter determines survival by reflecting an aggressive tumour phenotype which is more likely to metastasise early, rather than comprising the resection margin at the time of surgery.
Since tumour size can often be reliably assessed on cross-sectional imaging, these findings are significant in radiologically predicting which patients should proceed with resection surgery. A tumour size of greater than 3 cm on pre-operative imaging demonstrated poorer survival after resection with a relative hazard of 3.8 [183]. For patients who represent poor candidates for resection surgery, due to low functional capacity or anaesthetic risk, tumour size on pre-operative staging could be an important
Lymph Node Status
A total of 51 studies detailing outcome and lymph node status were found and the data presented in Table 7 [3, 5, 7, 8, 13, 14, 15, 17, 18, 29, 30, 32, 33, 40, 42, 43, 49, 50, 52, 53, 60, 62, 66, 70, 71, 74, 75, 76, 77, 78, 80, 84, 91, 92, 95, 97, 100, 105, 106, 108, 109, 114, 115, 116, 118, 120, 123, 124, 140, 142, 168]. The median percentage of lymph node negative tumours was 42.4%, range from 11.4% to 72.0%. The majority of the studies reviewed concluded that lymph node status was a predictor of survival on either univariate or multivariate analysis. The median cross-study survival for lymph node negative patients (N0) was 25 months and 13.6 months for lymph node positive patients (N1). This difference was found to be highly significant on both parametric and nonparametric statistical analysis (P<0.001). A positive association of negative lymph node status on survival was further confirmed by meta-analysis of the median survival data (OR=2.09, 95% CI: 1.69-2.60; P<0.001) and yearly survival data (OR=0.32, 95% CI: 0.24- 0.42; P<0.001) displayed in Figure 6.
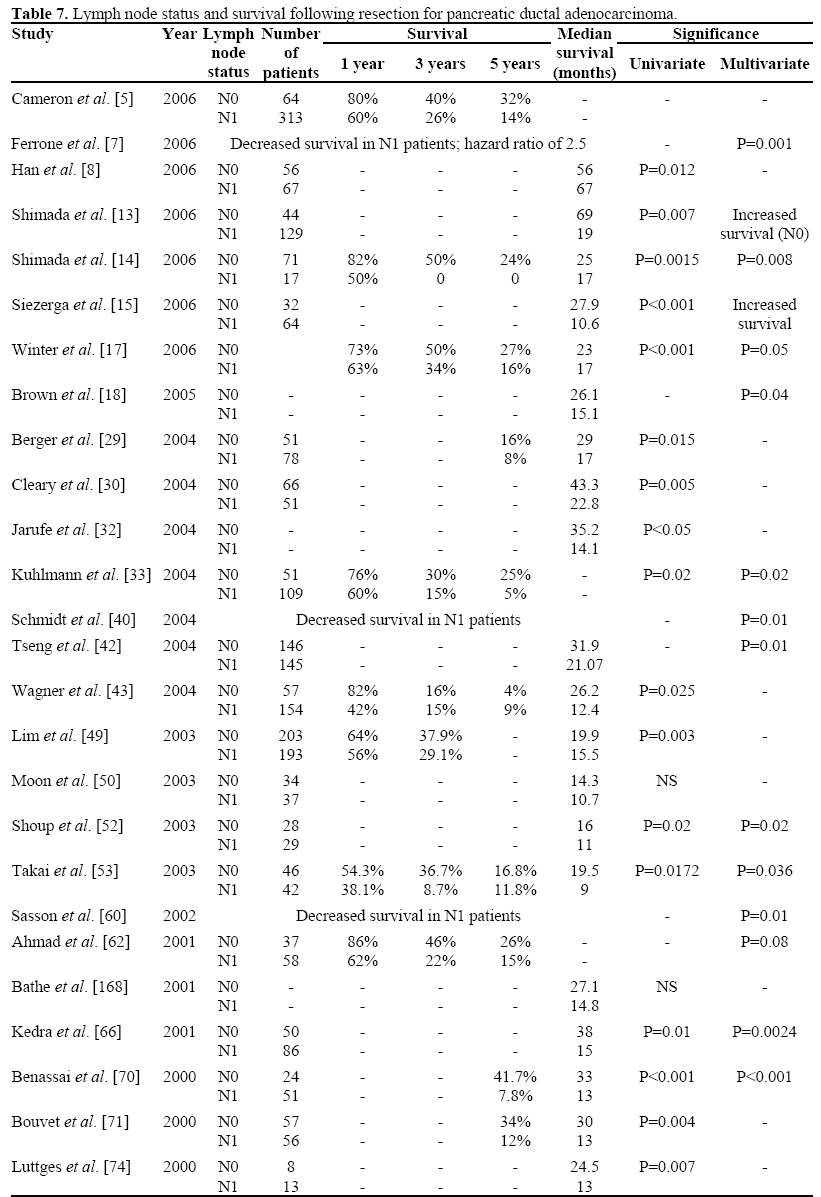
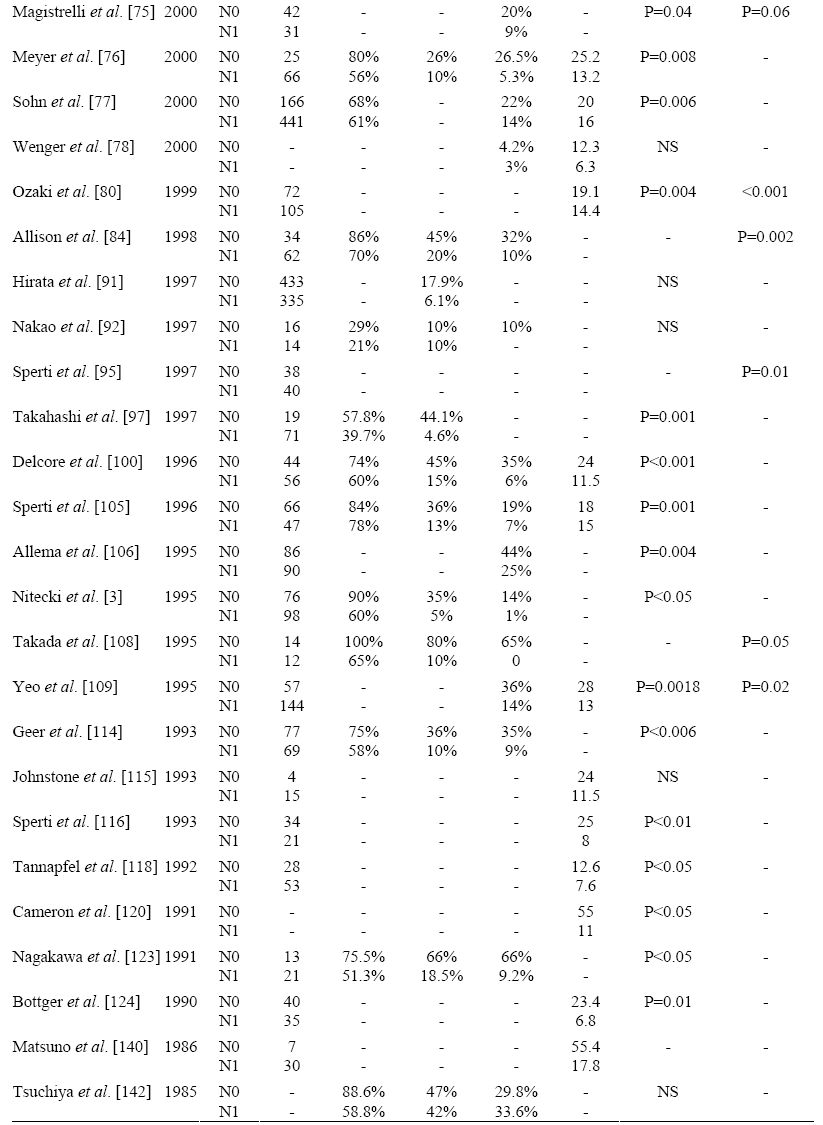
Figure 6. Forrest plot of median survival data and 1-,
3-, and 5-year survival and lymph node status in
pancreatic cancer resections.
The data suggest that lymph node positivity is a major determinant of outcome following resection, a finding supported by the largest prospective series of prognostic factors (the ESPAC 1 trial) [67]. More recently, some studies have found that the ratio of involved lymph nodes to total lymph nodes harvested is a more accurate predictor of survival than lymph node status alone [15, 29]. These findings would suggest that outcome might be improved by removing more lymph nodes, by undertaking an extended lymphadenectomy.
Only two randomized controlled trials have examined the role of extended resections [83, 90]. Although, both studies demonstrated increased lymph node harvest in the extended resection arm (19.8 versus 13.3 and 28.5 versus 17), neither study found that this resulted in a survival advantage (median survival: 16.7 months versus 11.2 months and 20 months versus 21 months) for the respective studies. Pawlik et al. found that only 0.3% of patients would achieve a survival advantage following an extended lymphadenectomy [184]. The required sample size for a randomized trial suitably powered to detect such a difference would be too large to make it feasible. For such an aggressive cancer such as pancreatic ductal adenocarcinoma, a further consideration is that patients who have extensive lymph node involvement would have a high probability of concurrent hepatic micrometastases, thereby precluding them from benefiting from radical resections. At present, there is no evidence that extended lymphadenectomy has a role to play pancreatic cancer surgery.
Grade of Tumour
Thirty-six studies reporting on survival and tumour grade were reviewed and the results are summarised in Table 8 [8, 13, 14, 15, 17, 30, 31, 32, 33, 43, 49, 50, 52, 53, 66, 70, 71, 74, 75, 76, 77, 81, 89, 95, 97, 98, 105, 106, 107, 108, 114, 116, 118, 120, 124, 140]. In contrast to the data on lymph node status, there is not an overwhelming consensus confirming an adverse outcome with poorer tumour grade. However, the majority of papers reviewed reported a statistically significant association. Tumours which were well-differentiated at resection accounted for the smallest proportion of all cancers, with moderately-differentiated tumours responsible for the majority of all resected tumours. These ratios are to be interpreted with some caution, since there were far fewer papers displaying the number of moderately-differentiated tumours, with many papers choosing to group this category with either well-differentiated or poorly-differentiated tumours, presumably in an attempt to amplify any survival differences. Meta-analysis of median survival (OR=2.40, 95% CI: 1.69-3.41) and yearly survival (OR=0.26, 95% CI: 0.15-0.45) figures between well-differentiated and poorly differentiated tumours confirmed that well-differentiated tumours were associated with prolonged survival (P<0.001) (Figure 7). Tumour grade impacts on survival by serving as an index of the biological aggressiveness of the cancer. Data from ESPAC trial also confirms tumour grade and lymph node status being the only two independent prognosticators following pancreatic cancer resection. Unfortunately, apart from serving as an index of prognosis, tumour grade is unquantifiable pre-operatively and cannot be influenced by surgical technique or chemotherapy.
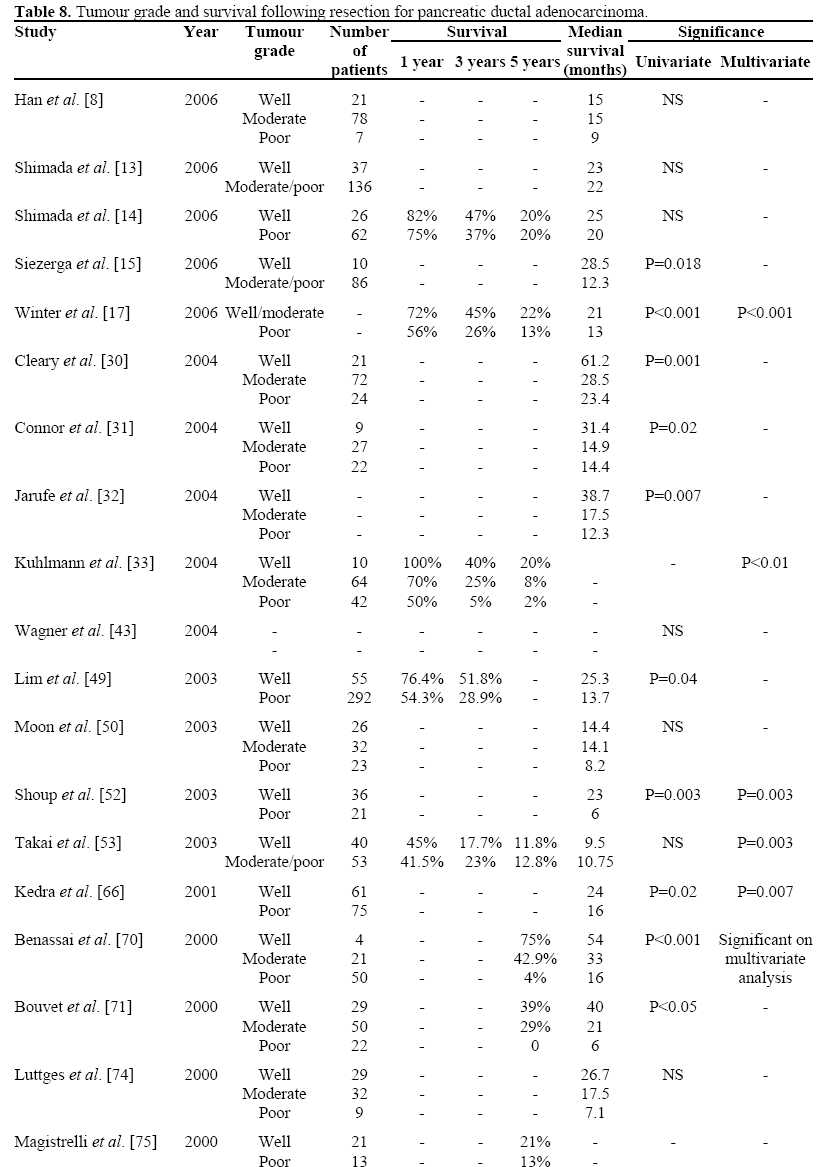

Figure 7. Forrest plot of median survival data and 1-,
3-, and 5-year survival and tumour grade in pancreatic
cancer resections.
Perineural and Blood Vessel Invasion
Thirteen studies detailing outcomes for pancreatic cancers with perineural invasion were found and eleven studies for pancreatic cancers and blood vessel invasion. The summarised data is presented in Table 9 [13, 14, 30, 43, 71, 76, 80, 97, 105, 114, 116, 120, 124] and Table 10 [13, 15, 30, 43, 66, 71, 74, 76, 80, 105, 120]. The majority of studies reviewed determined that blood vessel invasion was associated with poor outcome, predominantly on univariate analysis. Just over half of the studies examining perineural infiltration reported it as a significant prognostic variable for survival. The crossstudy median value for tumours without perineural invasion was 62.1% (12 studies) and tumours with no blood vessel invasion was 83.8% (9 studies). Cross-study median values for survival were 16 months versus 18.4 months for tumours with and without perineural infiltration, respectively, and 11.9 months versus 20.6 months for tumours with and without blood vessel invasion, respectively. Neither groups achieved statistical significance on simple parametric and non-parametric analysis. Meta-analysis of yearly survival data for perineural invasion did not achieve statistical significance (OR=0.53, 95% CI: 0.16-1.74, P=0.296), however the median survival data did (OR=2.37, 95% CI: 1.77-3.18, P<0.001). A similar finding was seen with blood vessel invasion with yearly survival data failing to show a significant survival advantage with no blood vessel invasion (OR=0.58, 95% CI: 0.26-1.31, P=0.191), which was found to be approaching significance following analysis of median survival data (OR=1.88, 95% CI: 0.89-3.49, P=0.097, respectively).
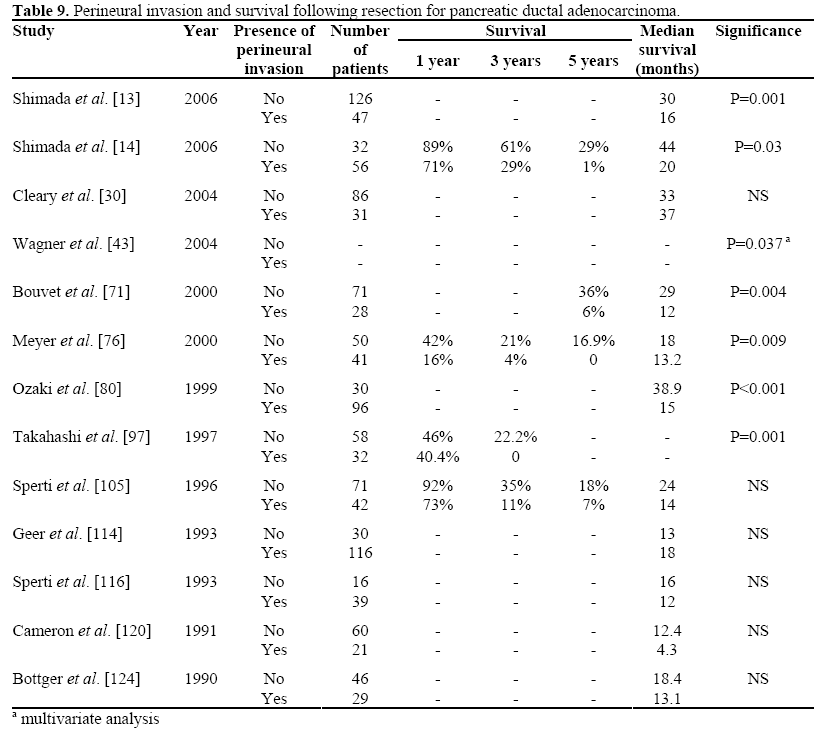
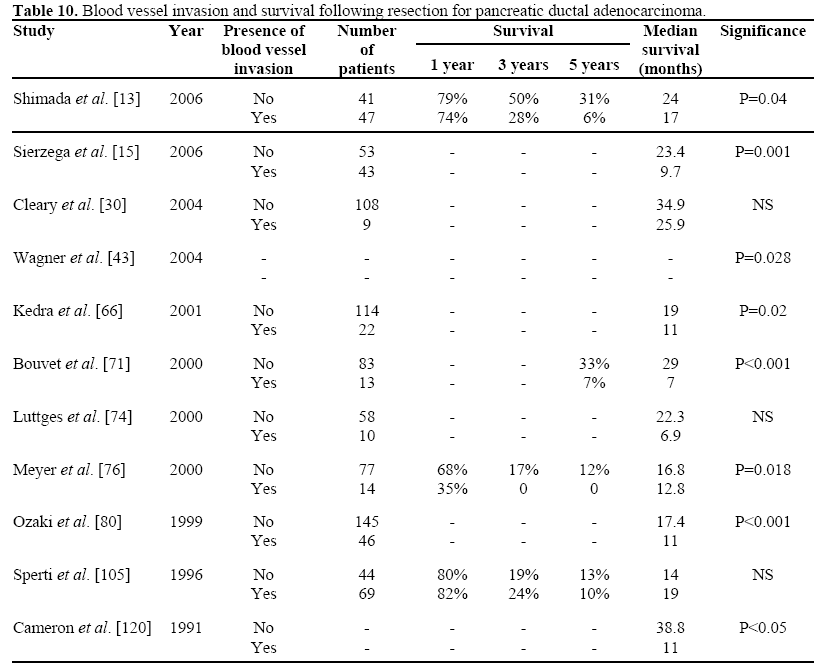
Micro-invasion of perineural and vascular tissue reflects an aggressive cancer phenotype. Perineural invasion, in particular, is regarded as a factor associated in local recurrence of pancreatic cancer and is associated with increasing de-differentiation of pancreatic tumours [185]. Pancreatic tissue hosts a large number of neural tissue and gangliae and is in close physical approximation to neural plexi in the retroperitoneum. It is, therefore, probable that perineural infiltration accounts for the main mechanism by which pancreatic cancers infiltrate the retroperitoneum. Data available only in abstract form by Pour et al. reported the presence of perineural infiltration in two tumours measuring only 2 and 4 mm in diameter [186], suggesting that perineural infiltration may be a very early event in pancreatic carcinogenesis. However, our finding that up to 63% of resected cancers were free of perineural infiltration would suggest otherwise. Despite microvessel invasion apparently being a less common finding (83% of resected cancers did not present with blood vessel invasion) the findings from Table 10 suggest that a greater proportion of the reviewed papers found it to impact deleteriously on survival when compared to perineural infiltration. This may be a consequence of the fact that although local recurrence is common following pancreatic cancer resection, it has been previously shown not to be a direct cause of death in contrast to lymphatic and hepatic metastatic disease [182]. So, whilst perineural invasion is more common and possibly an early event, microvessel invasion would lead to earlier haematogenous dissemination of disease and hence a have greater impact on survival.
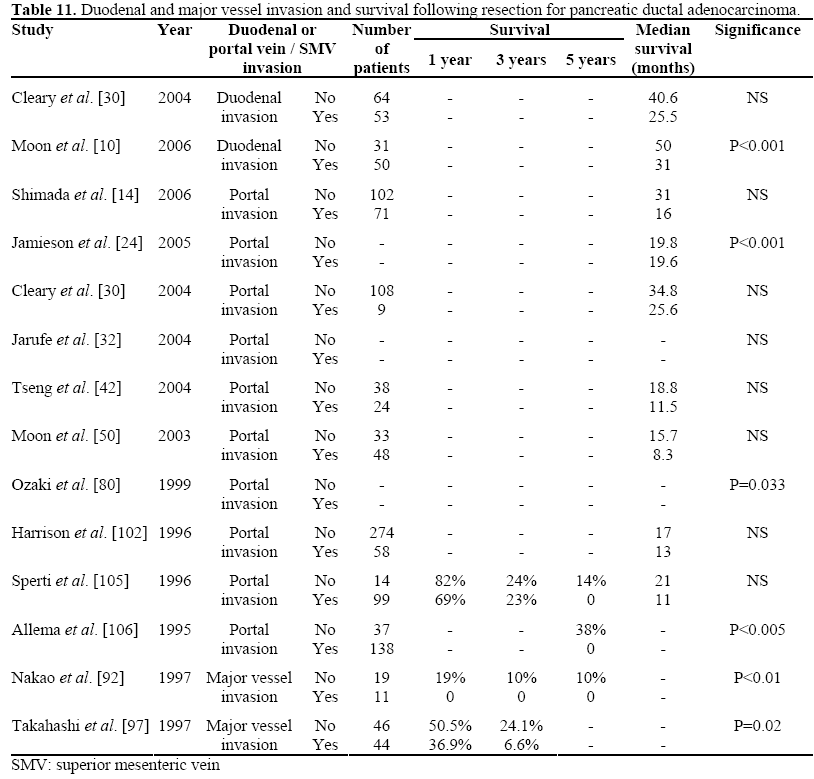
Duodenal and Major Vessel Invasion
Assessment of the clinical significance of major vessel invasion was problematic, since many studies detailing these results were papers reporting their series of venous resections. These papers were on the authors’ database since they also incorporated survival data for non-vascular pancreatic resections. Since, many centres would deem encasement of a major vessel a sign of inoperability, these data were not available from such papers, although many surgeons would be prepared to take a sleeve of portal vein to achieve a clear resection margin. These considerations may explain the skewed data presented in Table 11 [10, 14, 24, 30, 32, 42, 50, 80, 92, 97, 102, 105, 106], with many studies finding no significant impact on long-term survival. An adequate review of the risk-benefits of major venous resection and reconstruction in pancreatic cancer surgery is not the purpose of this paper. Only two papers were found detailing survival and duodenal invasion, whose findings are clearly at odds with each other, precluding any reasoned conclusion [10, 30].
Resection Margin
For most oncological resections histological involvement by tumour at the resection margin would be defined as non-curative operation, however, as the data in Table 12 [3, 5, 8, 10, 13, 14, 15, 17, 18, 28, 30, 31, 32, 33, 42, 43, 50, 51, 52, 53, 60, 70, 71, 74, 75, 77, 78, 79, 92, 97, 106, 108, 109, 114, 120, 126] shows some patients with R1 resections do survive to 5 years following their surgery. In addition, whilst survival following R1 resections is poor, it appears equivalent to survival associated with other deleterious factors. The median cross-study survival for R1 resections was 10.3 months (versus 20.3 months for R0 margins), as compared to 13.6 months for lymph node positive patients, 10.5 months for poorly differentiated tumours and 13 months for tumours greater than 3 cm in diameter. Clearly then, whilst positive resection margins would appear to impact negatively on survival, with the majority of the 35 reviewed studies confirming this on univariate or multivariate analysis, it is not necessarily equivalent to a palliative procedure. Six of the studies reviewed found that resection margins were not significantly associated with any decrease in survival [30, 31, 42, 52, 75, 114]. This observation is supported by the ESPAC data, which demonstrated resection margin to an independent risk factor for survival only in the absence of tumour grade or nodal status [67]. Indeed, our cross-study median survival of 10.3 months for R1 resections is very similar to the ESPAC’s group prospectively collected survival value of 10.9 months. Meta-analysis of median survival data (OR=3.00, 95% CI: 2.15-4.17, P<0.001)and yearly survival (OR=0.26, 95% CI: 0.16-0.42, P<0.001) both showed a strong survival advantage associated with a negative resection margin (Figure 8).
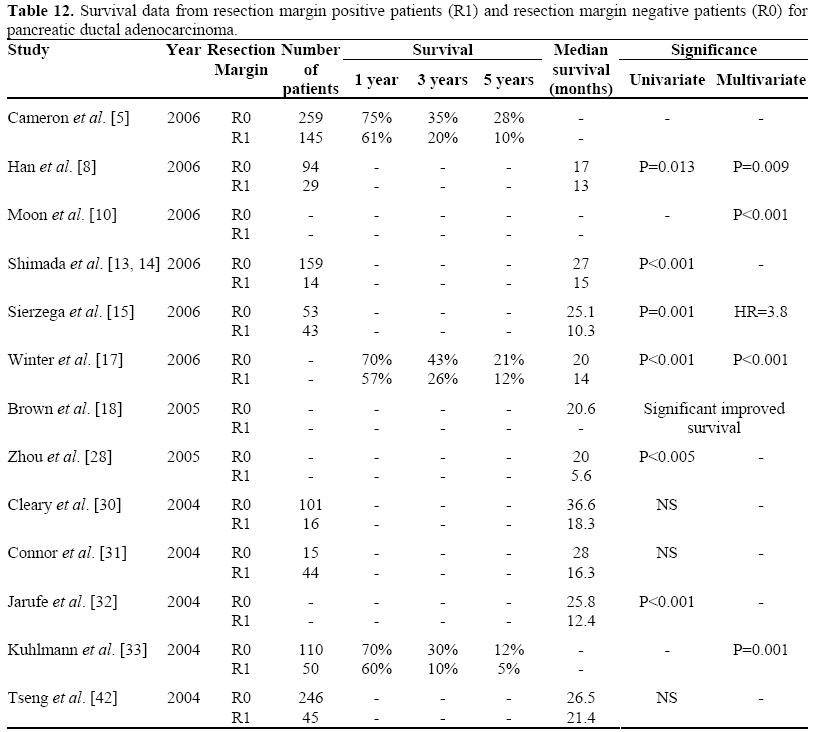
Figure 8. Forrest plot of median survival data and 1-,
3-, and 5-year survival and resection margin in
pancreatic cancer resections.
The reasons for this apparent disparity is that pathological handling and reporting of pancreatic specimens, at present, varies widely and guidelines issued by professional bodies lack detailed guidance regarding the assessment of resection margins [187]. These discrepancies in reporting obfuscate comparison of multinational studies. In addition, in many cases positive resection margins may not refer to tumour infiltration at the transection point across pancreatic tissue, bile duct or duodenum but rather to tumour infiltration up to the retroperitoneal tissues, i.e. dissection planes rather than transection margins. These considerations would suggest that resection margin may impact on survival by acting as an indicator of biological aggressiveness rather than being a technical factor which could be influenced by the operating surgeon [188].
Summary
A tumour diameter of less than 2 cm, negative lymph nodes, well-differentiated tumours and a negative resection margin would appear to be highly significant factors in determining prolonged survival following pancreatic cancer surgery. Individual studies also demonstrate that perineural and microvessel invasion are important prognostic factors, but this association is only weakly supported by meta-analysis of the current data. Resection margin and tumour diameter are probably indices of aggressive tumour phenotype rather than being directly causative for poor survival after surgery. Of these entire tumour characteristics reviewed, only tumour diameter can reliably be predicted preoperatively, the remainder being histopathological considerations following resection.
CONCLUSION
There have been considerable advances in the management of pancreatic cancer and centralisation of services has had a major impact on post-operative mortality and a modest increase in long-term survival. While the impact of chemotherapy and radiotherapy has not been assessed by this study, neoadjuvant therapy has also impacted significantly on the outcome following resection of pancreatic cancer. Until recently, no general consensus regarding the most appropriate regimen has been reached. This was predominantly due to a lack of adequately powered trials. A meta-analyses of five randomized controlled trials, from 1985 to 2004, investigating the roles of chemoradiation and chemotherapy revealed a 25% significant reduction in the risk of death following adjuvant treatment [189]. The most notable prospective study to date is the ESPAC-1 trial which has indicated a significant positive impact on long-term survival with chemotherapy with chemotherapy having a detrimental effect on survival [190]. Thus the current standard of care for pancreatic cancer is curative surgery followed by adjuvant systemic chemotherapy. Chemoradiation may yet have a role to play in patients with positive resection margins, but this remains to be determined [191].
However, it is a sobering thought that, excluding blood transfusion, tumour characteristics remain the only significant features influencing survival after pancreatic cancer surgery. Apart from tumour size, assessment of these criteria can only be made histopathologically and do not appear to be amenable to pre-operative or intraoperative manipulation. It remains to be seen whether new imaging modalities such as endoscopic ultrasound may allow better assessment of factors such as lymph node involvement. In light of these data, it could be reasoned that that tumour size, on cross-sectional imaging, might be employed as means of selecting the most appropriate candidates for surgery, in cases where the risks of resection are high.
Conflict of interest
The authors have no potential conflicts of interest
References
- Mancuso A, Calabrò F, Sternberg CN. Current therapies and advances in the treatment of pancreatic cancer. Crit Rev Oncol Hematol 2006; 58:231-41. [PMID 16725343]
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg 1999; 189:1-7. [PMID 10401733]
- Nitecki SS, Sarr MG, Colby TV, van Heerden JA. Long-term survival after resection for ductal adenocarcinoma of the pancreas. Is it really improving? Ann Surg 1995; 221:59-66. [PMID 7826162]
- Bramhall SR, Allum WH, Jones AG, Allwood A, Cummins C, Neoptolemos JP. Treatment and survival in 13,560 patients with pancreatic cancer, and incidence of the disease, in the West Midlands: an epidemiological study. Br J Surg 1995; 82:111-5. [PMID 7881926]
- Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006; 244:10-15. [PMID 16794383]
- Cress RD, Yin D, Clarke L, Bold R, Holly EA. Survival among patients with adenocarcinoma of the pancreas: a population-based study (United States). Cancer Causes Control 2006; 17:403-9. [PMID 16596292]
- Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, Fernandez-delCastillo C, Warshaw AL. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J Clin Oncol 2006; 24:2897-902. [PMID 16782929]
- Han SS, Jang JY, Kim SW, Kim WH, Lee KU, Park YH. Analysis of long-term survivors after surgical resection for pancreatic cancer. Pancreas 2006; 32:271- 5. [PMID 16628082]
- Kuhlmann K, de Castro S, van Heek T, Busch O, van Gulik T, Obertop H, Gouma D. Microscopically incomplete resection offers acceptable palliation in pancreatic cancer. Surgery 2006; 139:188-96. [PMID 16455327]
- Moon HJ, An JY, Heo JS, Choi SH, Joh JW, Kim YI. Predicting survival after surgical resection for pancreatic ductal adenocarcinoma. Pancreas 2006; 32:37-43. [PMID 16340742]
- Nakagohri T, Kinoshita T, Konishi M, Takahashi S, Gotohda N. Nodal involvement is strongest predictor of poor survival in patients with invasive adenocarcinoma of the head of the pancreas. Hepatogastroenterology 2006; 53:447-51. [PMID 16795990]
- Schwarz RE, Smith DD. Extent of lymph node retrieval and pancreatic cancer survival: information from a large US population database. Ann Surg Oncol 2006;13:1189-200. [PMID 16955385]
- Shimada K, Sakamoto Y, Sano T, Kosuge T, Hiraoka N. Reappraisal of the clinical significance of tumor size in patients with pancreatic ductal carcinoma. Pancreas 2006; 33:233-9. [PMID 17003643]
- Shimada K, Sakamoto Y, Sano T, Kosuge T. Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery 2006; 139:288-95. [PMID 16546491]
- Sierzega M, Popiela T, Kulig J, Nowak K. The ratio of metastatic/resected lymph nodes is an independent prognostic factor in patients with nodepositive pancreatic head cancer. Pancreas 2006; 33:240-5. [PMID 17003644]
- van Oost FJ, Luiten EJ, van de Poll-Franse LV, Coebergh JW, van den Eijnden-van Raaij AJ. Outcome of surgical treatment of pancreatic, peri-ampullary and ampullary cancer diagnosed in the south of The Netherlands: a cancer registry based study. Eur J Surg Oncol 2006; 32:548-52. [PMID 16569495]
- Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J Gastrointest Surg 2006; 10:1199-210. [PMID 17114007]
- Brown KM, Domin C, Aranha GV, Yong S, Shoup M. Increased preoperative platelet count is associated with decreased survival after resection for adenocarcinoma of the pancreas. Am J Surg 2005; 189:278-82. [PMID 15792750]
- Christein JD, Kendrick ML, Iqbal CW, Nagorney DM, Farnell MB. Distal pancreatectomy for resectable adenocarcinoma of the body and tail of the pancreas. J Gastrointest Surg 2005; 9:922-7. [PMID 16137585]
- Ferrone CR, Kattan MW, Tomlinson JS, Thayer SP, Brennan MF, Warshaw AL. Validation of a postresection pancreatic adenocarcinoma nomogram for disease-specific survival. J Clin Oncol 2005; 30:7529-35. [PMID 16234519]
- Fong Y, Gonen M, Rubin D, Radzyner M, Brennan MF. Long-term survival is superior after resection for cancer in high-volume centers. Ann Surg 2005; 242:540-4. [PMID 16192814]
- Hirota M, Shimada S, Yamamoto K, Tanaka E, Sugita H, Egami H, Ogawa M. Pancreatectomy using the no-touch isolation technique followed by extensive intraoperative peritoneal lavage to prevent cancer cell dissemination: a pilot study. JOP. J Pancreas (Online) 2005; 6:143-51. [PMID 15767730]
- Jain S, Sacchi M, Vrachnos P, Lygidakis NJ. Carcinoma of the pancreas with portal vein involvement--our experience with a modified technique of resection. Hepatogastroenterology 2005; 52:1596- 600. [PMID 16201124]
- Jamieson NB, Glen P, McMillan DC, McKay CJ, Foulis AK, Carter R, Imrie CW. Systemic inflammatory response predicts outcome in patients undergoing resection for ductal adenocarcinoma head of pancreas. Br J Cancer 2005; 92:21-3. [PMID 15597096]
- Krysa J, Miller M, Kukreja N, Steger A. Pancreatic cancer: is an aggressive approach justified? Ann R Coll Surg Engl 2005; 87:163-6. [PMID 15901374]
- Mu DQ, Peng SY, Wang GF. Extended radical operation of pancreatic head cancer: appraisal of its clinical significance. World J Gastroenterol 2005; 11:2467-71. [PMID 15832419]
- Ridwelski K, Meyer F, Schmidt U, Lippert H. Results of surgical treatment in ampullary and pancreatic carcinoma and its prognostic parameters after R0-resection. Zentrabl Chir 2005; 130:353-61. [PMID 16103961]
- Zhou GW, Wu WD, Xiao WD, Li HW, Peng CH. Pancreatectomy combined with superior mesentericportal vein resection: report of 32 cases. Hepatobiliary Pancreat Dis Int 2005; 4:130-4. [PMID 15730937]
- Berger AC, Watson JC, Ross EA, Hoffman JP. The metastatic/examined lymph node ratio is an important prognostic factor after pancreaticoduodenectomy for pancreatic adenocarcinoma. Am Surg 2004; 70:235-40. [PMID 15055847]
- Cleary SP, Gryfe R, Guindi M, Greig P, Smith L, Mackenzie R, et al. Prognostic factors in resected pancreatic adenocarcinoma: analysis of actual 5-year survivors. J Am Coll Surg 2004; 198:722-31. [PMID 15110805]
- Connor S, Bosonnet L, Ghaneh P, Alexakis N, Hartley M, Campbell F, et al. Survival of patients with periampullary carcinoma is predicted by lymph node 8a but not by lymph node 16b1 status. Br J Surg 2004; 91:1592-9. [PMID 15515111]
- Jarufe NP, Coldham C, Mayer AD, Mirza DF, Buckels JA, Bramhall SR. Favourable prognostic factors in a large UK experience of adenocarcinoma of the head of the pancreas and periampullary region. Dig Surg 2004; 21:202-9. [PMID 15218236]
- Kuhlmann KF, de Castro SM, Wesseling JG, ten Kate FJ, Offerhaus GJ, Busch OR, et al. Surgical treatment of pancreatic adenocarcinoma; actual survival and prognostic factors in 343 patients. Eur J Cancer 2004; 40:549-58. [PMID 14962722]
- Li B, Chen FZ, Ge XH, Cai MZ, Jiang JS, Li JP, Lu SH. Pancreatoduodenectomy with vascular reconstruction in treating carcinoma of the pancreatic head. Hepatobiliary Pancreat Dis Int 2004; 3:612-5. [PMID 15567757]
- Lygidakis NJ, Singh G, Bardaxoglou E, Dedemadi G, Sgourakis G, Nestoridis J, et al. Mono-bloc total spleno-pancreaticoduodenectomy for pancreatic head carcinoma with portal-mesenteric venous invasion. A prospective randomized study. Hepatogastroenterology 2004; 51:427-33. [PMID 15086174]
- Mu DQ, Peng SY, Wang GF. Risk factors influencing recurrence following resection of pancreatic head cancer. World J Gastroenterol 2004; 10:906-9. [PMID 15040043]
- Nagakawa T, Sanada H, Inagaki M, Sugama J, Ueno K, Konishi I, et al. Long-term survivors after resection of carcinoma of the head of the pancreas: significance of histologically curative resection. J Hepatobiliary Pancreat Surg 2004; 11:402-8. [PMID 15619016]
- Parks RW, Bettschart V, Frame S, Stockton DL, Brewster DH, Garden OJ. Benefits of specialisation in the management of pancreatic cancer: results of a Scottish population-based study. Br J Cancer 2004; 91:459-65. [PMID 15226766]
- Poon RT, Fan ST, Lo CM, Liu CL, Lam CM, Yuen WK, et al. Pancreaticoduodenectomy with en bloc portal vein resection for pancreatic carcinoma with suspected portal vein involvement. World J Surg 2004; 28:602-8. [PMID 15366753]
- Schmidt CM, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, et al. Pancreaticoduodenectomy: a 20-year experience in 516 patients. Arch Surg 2004; 139:718-27. [PMID 15249403]
- Suzuki K, Aiura K, Kitagou M, Hoshimoto S, Takahashi S, Ueda M, Kitajima M. Platelet counts closely correlate with the disease-free survival interval of pancreatic cancer patients. Hepatogastroenterology 2004; 51:847-53. [PMID 15143932]
- Tseng JF, Raut CP, Lee JE, Pisters PW, Vauthey JN, Abdalla EK, et al. Pancreaticoduodenectomy with vascular resection: margin status and survival duration. J Gastrointest Surg 2004; 8:935-50. [PMID 15585381]
- Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Büchler MW. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg 2004; 91:586- 94. [PMID 15122610]
- Wakeman CJ, Martin IG, Robertson RW, Dobbs BR, Frizelle FA. Pancreatic cancer: management and survival. ANZ J Surg 2004; 74:941-4. [PMID 15550079]
- Yuen JS, Ooi LL, Chow PK, Chung AY, Khin LW, Soo KC. Subspecialization and pancreaticoduodenectomy: learning experience from 71 consecutive cases. Asian J Surg 2004; 27:73-9. [PMID 15140656]
- Bachmann MO, Alderson D, Peters TJ, Bedford C, Edwards D, Wotton S, Harvey IM. Influence of specialization on the management and outcome of patients with pancreatic cancer. Br J Surg 2003; 90:171-7. [PMID 12555292]
- Finlayson EV, Birkmeyer JD. Effects of hospital volume on life expectancy after selected cancer operations in older adults: a decision analysis. J Am Coll Surg 2003; 196:410-7. [PMID 12648693]
- Howard TJ, Villanustre N, Moore SA, DeWitt J, LeBlanc J, Maglinte D, McHenry L. Efficacy of venous reconstruction in patients with adenocarcinoma of the pancreatic head. J Gastrointest Surg 2003; 7:1089-95. [PMID 14675720]
- Lim JE, Chien MW, Earle CC. Prognostic factors following curative resection for pancreatic adenocarcinoma: a population-based, linked database analysis of 396 patients. Ann Surg 2003; 237:74-85. [PMID 12496533]
- Moon HJ, Jang KT, Heo JS, Choi SH, Joh JW, Kim YI. A result of surgical treatment for ductal adenocarcinoma of the head of the pancreas. Korean J Gastroenterol 2003; 42:156-63. [PMID 14532721]
- Nakagohri T, Kinoshita T, Konishi M, Inoue K, Takahashi S. Survival benefits of portal vein resection for pancreatic cancer. Am J Surg 2003; 186:149-53. [PMID 12885608]
- Shoup M, Conlon KC, Klimstra D, Brennan MF. Is extended resection for adenocarcinoma of the body or tail of the pancreas justified. J Gastrointest Surg 2003; 7:946-52. [PMID 14675703]
- Takai S, Satoi S, Toyokawa H, Yanagimoto H, Sugimoto N, Tsuji K, et al. Clinicopathologic evaluation after resection for ductal adenocarcinoma of the pancreas: a retrospective, single-institution experience. Pancreas 2003; 26:243-9. [PMID 12657950]
- Talar-Wojnarowska R, Gasiorowska A, Strzelczyk J, Janiak A, Malecka-Panas E. Prognostic factors in the operative and palliative treatment of pancreatic cancer. Neoplasma 2003; 50:383-7. [PMID 14628094]
- Hartel M, Niedergethmann M, Farag-Soliman M, Sturm JW, Richter A, Trede M, Post S. Benefit of venous resection for ductal adenocarcinoma of the pancreatic head. Eur J Surg 2002; 168:707-12. [PMID 15362580]
- Ni QX, Zhang QH, Fu DL, Cao GH, Yao QY, Jin C, et al. Curative resection of pancreatic head carcinoma in recent 30 years: report of 377 cases. Hepatobiliary Pancreat Dis Int 2002; 1:126-8. [PMID 14607640]
- Nordback L, Parviainen M, Räty S, Kuivanen H, Sand J. Resection of the head of the pancreas in Finland: effects of hospital and surgeon on short-term and long-term results. Scand J Gastroenterol 2002; 37:1454-60. [PMID 12523597]
- Popiela T, Kedra B, Sierzega M. Does extended lymphadenectomy improve survival of pancreatic cancer patients? Acta Chir Belg 2002; 102:78-82. [PMID 12051095]
- Richter A, Niedergethmann M, Lorenz D, Sturm JW, Trede M, Post S. Resection for cancers of the pancreatic head in patients aged 70 years or over. Eur J Surg 2002; 168:339-44. [PMID 12428871]
- Sasson AR, Hoffman JP, Ross EA, Kagan SA, Pingpank JF, Eisenberg BL. En bloc resection for locally advanced cancer of the pancreas: is it worthwhile? J Gastrointest Surg 2002; 6:147-57. [PMID 11992799]
- Yeo CJ, Cameron JL, Lillemoe KD, Sohn TA, Campbell KA, Sauter PK, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg 2002; 236:355-66. [PMID 12192322]
- Ahmad NA, Lewis JD, Ginsberg GG, Haller DG, Morris JB, Williams NN, et al. Long term survival after pancreatic resection for pancreatic adenocarcinoma. Am J Gastroenterol 2001; 96:2609- 15. [PMID 11569683]
- Bachellier P, Nakano H, Oussoultzoglou PD, Weber JC, Boudjema K, Wolf PD, Jaeck D. Is pancreaticoduodenectomy with mesentericoportal venous resection safe and worthwhile? Am J Surg 2001; 182:120-9. [PMID 11574081]
- Bathe OF, Caldera H, Hamilton KL, Franceschi D, Sleeman D, Livingstone AS, Levi JU. Diminished benefit from resection of cancer of the head of the pancreas in patients of advanced age. J Surg Oncol 2001; 77:115-22. [PMID 11398165]
- Karpoff HM, Klimstra D, Brennan MF, Conlon KC. Results of total pancreatectomy for adenocarcinoma of the pancreas. Arch Surg 2001; 136:44-7. [PMID 11146775]
- Kedra B, Popiela T, Sierzega M, Precht A. Prognostic factors of long-term survival after resective procedures for pancreatic cancer. Hepatogastroenterology 2001; 48:1762-6. [PMID 11813619]
- Neoptolemos JP, Stocken DD, Dunn JA, Almond J, Beger HG, Pederzoli P, et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann Surg 2001; 234:758-68. [PMID 11729382]
- van Geenen RC, ten Kate FJ, de Wit LT, van Gulik TM, Obertop H, Gouma DJ. Segmental resection and wedge excision of the portal or superior mesenteric vein during pancreatoduodenectomy. Surgery 2001; 129:158-63. [PMID 11174708]
- van Geenen RC, van Gulik TM, Offerhaus GJ, de Wit LT, Busch OR, Obertop H, Gouma DJ. Survival after pancreaticoduodenectomy for periampullary adenocarcinoma: an update. Eur J Surg Oncol 2001; 27:549-57. [PMID 11520088]
- Benassai G, Mastrorilli M, Quarto G, Cappiello A, Giani U, Forestieri P, Mazzeo F. Factors influencing survival after resection for ductal adenocarcinoma of the head of the pancreas. J Surg Oncol 2000; 73:212-8. [PMID 10797334]
- Bouvet M, Gamagami RA, Gilpin EA, Romeo O, Sasson A, Easter DW, Moossa AR. Factors influencing survival after resection for periampullary neoplasms. Am J Surg 2000; 180:13-7. [PMID 11036132]
- Gebhardt C, Meyer W, Reichel M, Wünsch PH. Prognostic factors in the operative treatment of ductal pancreatic carcinoma. Langenbecks Arch Surg 2000; 385:14-20. [PMID 10664114]
- Henne-Bruns D, Vogel I, Lüttges J, Klöppel G, Kremer B. Surgery for ductal adenocarcinoma of the pancreatic head: staging, complications, and survival after regional versus extended lymphadenectomy. World J Surg 2000; 24:595-601. [PMID 10787083]
- Lüttges J, Schemm S, Vogel I, Hedderich J, Kremer B, Klöppel G. The grade of pancreatic ductal carcinoma is an independent prognostic factor and is superior to the immunohistochemical assessment of proliferation. J Pathol 2000; 191:154-61. [PMID 10861575]
- Magistrelli P, Antinori A, Crucitti A, La Greca A, Masetti R, Coppola R, et al. Prognostic factors after surgical resection for pancreatic carcinoma. J Surg Oncol 2000; 74:36-40. [PMID 10861607]
- Meyer W, Jurowich C, Reichel M, Steinhäuser B, Wünsch PH, Gebhardt C. Pathomorphological and histological prognostic factors in curatively resected ductal adenocarcinoma of the pancreas. Surg Today 2000; 30:582-7. [PMID 10930222]
- Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, et al. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg 2000; 4:567-79. [PMID 11307091]
- Wenger FA, Peter F, Zieren J, Steiert A, Jacobi CA, Müller JM. Prognosis factors in carcinoma of the head of the pancreas. Dig Surg 2000; 17:29-35. [PMID 10720829]
- Benassai G, Mastrorilli M, Mosella F, Mosella G. Significance of lymph node metastases in the surgical management of pancreatic head carcinoma. J Exp Clin Cancer Res 1999; 18:23-8. [PMID 10374672]
- Ozaki H, Hiraoka T, Mizumoto R, Matsuno S, Matsumoto Y, Nakayama T, et al. The prognostic significance of lymph node metastasis and intrapancreatic perineural invasion in pancreatic cancer after curative resection. Surg Today 1999; 29:16-22. [PMID 9934826]
- Sellner FJ, Riegler FM, Machacek E. Implications of histological grade of tumour for the prognosis of radically resected periampullary adenocarcinoma. Eur J Surg 1999; 165:865-70. [PMID 10533763]
- Yamaguchi K, Mizumoto K, Noshiro H, Sugitani A, Shimizu S, Chijiiwa K, Tanaka M. Pancreatic carcinoma: < or = 2 cm versus > 2 cm in size. Int Surg 1999; 84:213-9. [PMID 10533779]
- Yeo CJ, Cameron JL, Sohn TA, Coleman J, Sauter PK, Hruban RH, et al. Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: comparison of morbidity and mortality and short-term outcome. Ann Surg 1999; 229:613-22. [PMID 10235519]
- Allison DC, Piantadosi S, Hruban RH, Dooley WC, Fishman EK, Yeo CJ, et al. DNA content and other factors associated with ten-year survival after resection of pancreatic carcinoma. J Surg Oncol 1998; 67:151-9. [PMID 9530884]
- Crucitti F, Doglietto GB, Viola G, Frontera D, De Cosmo G, Sgadari A, et al. Assessment of risk factors for pancreatic resection for cancer. World J Surg 1998; 22:241-7. [PMID 9494415]
- Harrison LE, Brennan MF. Portal vein involvement in pancreatic cancer: a sign of unresectability? Adv Surg 1998; 31:375-94. [PMID 9408502]
- Imaizumi T, Hanyu F, Harada N, Hatori T, Fukuda A. Extended radical Whipple resection for cancer of the pancreatic head: operative procedure and results. Dig Surg 1998; 15:299-307. [PMID 9845603]
- Leach SD, Lee JE, Charnsangavej C, Cleary KR, Lowy AM, Fenoglio CJ, et al. Survival following pancreaticoduodenectomy with resection of the superior mesenteric-portal vein confluence for adenocarcinoma of the pancreatic head. Br J Surg 1998; 85:611-7. [PMID 9635805]
- Mukaiya M, Hirata K, Satoh T, Kimura M, Yamashiro K, Ura H, et al. Lack of survival benefit of extended lymph node dissection for ductal adenocarcinoma of the head of the pancreas: retrospective multi-institutional analysis in Japan. World J Surg 1998; 22:248-52. [PMID 9494416]
- Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali C, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg 1998; 228:508-17. [PMID 9790340]
- Hirata K, Sato T, Mukaiya M, Yamashiro K, Kimura M, Sasaki K, Denno R. Results of 1001 pancreatic resections for invasive ductal adenocarcinoma of the pancreas. Arch Surg 1997; 132:771-6. [PMID 9230864]
- Nakao A, Harada A, Nonami T, Kaneko T, Nomoto S, Koyama H, et al. Lymph node metastasis in carcinoma of the body and tail of the pancreas. Br J Surg 1997; 84:1090-2. [PMID 9278647]
- Neoptolemos JP, Russell RC, Bramhall S, Theis B. Low mortality following resection for pancreatic and periampullary tumours in 1026 patients: UK survey of specialist pancreatic units. UK Pancreatic Cancer Group. Br J Surg 1997; 84:1370-6. [PMID 9361591]
- Shahrudin MD. Carcinoma of the pancreas: resection outcome at the University Hospital Kuala Lumpur. Int Surg 1997; 82:269-74. [PMID 9372373]
- Sperti C, Pasquali C, Piccoli A, Pedrazzoli S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg 1997; 21:195-200. [PMID 8995078]
- Sung JP, Stewart RD, O'Hara VS, Westhpal KF, Wilkinson JE, Hill J. A study of forty-nine consecutive Whipple resections for periampullary adenocarcinoma. Am J Surg 1997; 174:6-10. [PMID 9240943]
- Takahashi T, Niino N, Ishikura H, Okushiba S, Dohke M, Katoh H. Predictive factors for long-term survival in patients with pancreatic carcinoma. Hepatogastroenterology 1997; 44:1463-8. [PMID 9356873]
- Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg 1997; 226:248-60. [PMID 9339931]
- Conlon KC, Klimstra DS, Brennan MF. Long-term survival after curative resection for pancreatic ductal adenocarcinoma. Clinicopathologic analysis of 5-year survivors. Ann Surg 1996; 223:273-9. [PMID 8604907]
- Delcore R, Rodriguez FJ, Forster J, Hermreck AS, Thomas JH. Significance of lymph node metastases in patients with pancreatic cancer undergoing curative resection. Am J Surg 1996; 172:463-8. [PMID 8942545]
- Fortner JG, Klimstra DS, Senie RT, Maclean BJ. Tumor size is the primary prognosticator for pancreatic cancer after regional pancreatectomy. Ann Surg 1996; 223:147-53. [PMID 8597508]
- Harrison LE, Klimstra DS, Brennan MF. Isolated portal vein involvement in pancreatic adenocarcinoma. A contraindication for resection? Ann Surg 1996; 224:342-7. [PMID 8813262]
- Nagakawa T, Nagamori M, Futakami F, Tsukioka Y, Kayahara M, Ohta T, et al. Results of extensive surgery for pancreatic carcinoma. Cancer 1996; 77:640-5. [PMID 8616755]
- Roder JD, Stein HJ, Siewert JR. Carcinoma of the periampullary region: who benefits from portal vein resection? Am J Surg 1996; 171:170-4. [PMID 8554135]
- Sperti C, Pasquali C, Piccoli A, Pedrazzoli S. Survival after resection for ductal adenocarcinoma of the pancreas. Br J Surg 1996; 83:625-31. [PMID 8689203]
- Allema JH, Reinders ME, van Gulik TM, Koelemay MJ, Van Leeuwen DJ, de Wit LT, et al. Prognostic factors for survival after pancreaticoduodenectomy for patients with carcinoma of the pancreatic head region. Cancer 1995; 75:2069- 76. [PMID 7697596]
- Klempnauer J, Ridder GJ, Pichlmayr R. Prognostic factors after resection of ampullary carcinoma: multivariate survival analysis in comparison with ductal cancer of the pancreatic head. Br J Surg 1995; 82:1686-91. [PMID 8548242]
- Takada T, Yasuda H. A search for prognostic factors in cancer of the pancreatic head: the significance of the DNA ploidy pattern. Surg Oncol 1995; 4:237-43. [PMID 8850025]
- Yeo CJ, Cameron JL, Lillemoe KD, Sitzmann JV, Hruban RH, Goodman SN, et al. Pancreaticoduodenectomy for cancer of the head of the pancreas. 201 patients. Ann Surg 1995; 221:721-31. [PMID 7794076]
- Allema JH, Reinders ME, van Gulik TM, van Leeuwen DJ, de Wit LT, Verbeek PC, Gouma DJ. Portal vein resection in patients undergoing pancreatoduodenectomy for carcinoma of the pancreatic head. Br J Surg 1994; 81:1642-6. [PMID 7827892]
- Mohiuddin M, Rosato F, Schuricht A, Barbot D, Biermann W, Cantor R. Carcinoma of the pancreas- the Jefferson experience 1975-1988. Eur J Surg Oncol 1994; 20:13-20. [PMID 8131862]
- Tsao JI, Rossi RL, Lowell JA. Pylorus-preserving pancreatoduodenectomy. Is it an adequate cancer operation. Arch Surg 1994; 129:405-12. [PMID 7908796]
- Edge SB, Schmieg RE Jr, Rosenlof LK, Wilhelm MC. Pancreas cancer resection outcome in American University centers in 1989-1990. Cancer 1993; 71:3502-8. [PMID 8098265]
- Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg 1993; 165:68-72. [PMID 8380315]
- Johnstone PA, Sindelar WF. Lymph node involvement and pancreatic resection: correlation with prognosis and local disease control in a clinical trial. Pancreas 1993; 8:535-9. [PMID 8302788]
- Sperti C, Bonadimani B, Pasquali C, Piccoli A, Cappellazzo F, Rugge M, Pedrazzoli S. Ductal adenocarcinoma of the pancreas: clinicopathologic features and survival. Tumori 1993; 79:325-30. [PMID 8116075]
- Satake K, Nishiwaki H, Yokomatsu H, Kawazoe Y, Kim K, Haku A, et al. Surgical curability and prognosis for standard versus extended resection for T1 carcinoma of the pancreas. Surg Gynecol Obstet 1992; 175:259-65. [PMID 1514162]
- Tannapfel A, Wittekind C, Hünefeld G. Ductal adenocarcinoma of the pancreas. Int J Pancreatol 1992; 12:145-52. [PMID 1460329]
- Andren-Sandberg A, Ahrén B, Tranberg KG, Bengmark S. Surgical treatment of pancreatic cancer. The Swedish experience. Int J Pancreatol 1991; 9:145- 51. [PMID 1744440]
- Cameron JL, Crist DW, Sitzmann JV, Hruban RH, Boitnott JK, Seidler AJ, Coleman J. Factors influencing survival after pancreaticoduodenectomy for pancreatic cancer. Am J Surg 1991; 161:120-4. [PMID 1987845]
- Delcore R, Thomas JH, Hermreck AS. Pancreaticoduodenectomy for malignant pancreatic and periampullary neoplasms in elderly patients. Am J Surg 1991; 162:532-5. [PMID 1670220]
- Livingston EH, Welton ML, Reber HA. Surgical treatment of pancreatic cancer. The United States Experience. Int J Pancreatol 1991; 9:153-7. [PMID 1720800]
- Nagakawa T, Konishi I, Ueno K, Ohta T, Akiyama T, Kayahara M, Miyazaki I. Surgical treatment of pancreatic cancer. The Japanese experience. Int J Pancreatol 1991; 9:135-45. [PMID 1744439]
- Böttger T, Zech J, Weber W, Sorger K, Junginger T. Relevant factors in the prognosis of ductal pancreatic carcinoma. Acta Chir Scand 1990; 156:781- 8. [PMID 1706125]
- Doerr RJ, Yildiz I, Flint LM. Pancreaticoduodenectomy. University experience and resident education. Arch Surg 1990; 125:463-5. [PMID 2322112]
- Trede M, Schwall G, Saeger HD. Survival after pancreatoduodenectomy. 118 consecutive resections without an operative mortality. Ann Surg 1990; 211:447-8. [PMID 2322039]
- Winek T, Hamre D, Mozell E, Vetto RM. Prognostic factors for survival after pancreaticoduodenectomy for malignant disease. Am J Surg 1990; 159:454-6. [PMID 2334005]
- Kairaluoma MI, Ståhlberg M, Kiviniemi H, Haukipuro K. Results of pancreatoduodenectomy for carcinoma of the head of the pancreas. Hepatogastroenterology 1989; 36:412-8. [PMID 2613164]
- Lygidakis NJ, van der Hyde MN, Houthoff HJ, Schipper ME, Huibregtse K, Tytgat GN, et al. Resectional surgical procedures for carcinoma of the head of the pancreas. Surg Gynecol Obstet 1989; 168:157-65. [PMID 2911793]
- Manabe T, Ohshio G, Baba N, Miyashita T, Asano N, Tamura K, et al. Radical pancreatectomy for ductal cell carcinoma of the head of the pancreas. Cancer 1989; 64:1132-7. [PMID 2547508]
- Michelassi F, Erroi F, Dawson PJ, Pietrabissa A, Noda S, Handcock M, Block GE. Experience with 647 consecutive tumors of the duodenum, ampulla, head of the pancreas, and distal common bile duct. Ann Surg 1989; 210:544-54. [PMID 2679459]
- Pellegrini CA, Heck CF, Raper S, Way LW. An analysis of the reduced morbidity and mortality rates after pancreaticoduodenectomy. Arch Surg 1989; 124:778-81. [PMID 2742478]
- Sindelar WF. Clinical experience with regional pancreatectomy for adenocarcinoma of the pancreas. Arch Surg 1989; 124:127-32. [PMID 2910241]
- Ishikawa O, Ohhigashi H, Sasaki Y, Kabuto T, Fukuda I, Furukawa H, et al. Practical usefulness of lymphatic and connective tissue clearance for the carcinoma of the pancreas head. Ann Surg 1988; 208:215-20. [PMID 2840866]
- Connolly MM, Dawson PJ, Michelassi F, Moossa AR, Lowenstein F. Survival in 1001 patients with carcinoma of the pancreas. Ann Surg 1987; 206:366- 73. [PMID 2820322]
- Crist DW, Sitzmann JV, Cameron JL. Improved hospital morbidity, mortality, and survival after the Whipple procedure. Ann Surg 1987; 206:358-65. [PMID 3632096]
- Braasch JW, Deziel DJ, Rossi RL, Watkins E Jr, Winter PF. Pyloric and gastric preserving pancreatic resection. Experience with 87 patients. Ann Surg 1986; 204:411-8. [PMID 3767476]
- Grace PA, Pitt HA, Tompkins RK, DenBesten L, Longmire WP Jr. Decreased morbidity and mortality after pancreatoduodenectomy. Am J Surg 1986; 151:141-9. [PMID 3946745]
- Mannell A, van Heerden JA, Weiland LH, Ilstrup DM. Factors influencing survival after resection for ductal adenocarcinoma of the pancreas. Ann Surg 1986; 203:403-7. [PMID 3008674]
- Matsuno S, Sato T. Surgical treatment of carcinoma of the pancreas. Experience in 272 patients. Am J Surg 1986; 152:499-504. [PMID 2430481]
- Tarazi RY, Hermann RE, Vogt DP, Hoerr SO, Esselstyn CB Jr, Cooperman AM, et al. Results of surgical treatment of periampullary tumors: a thirtyfive- year experience. Surgery 1986; 100:716-23. [PMID 3764694]
- Tsuchiya R, Noda T, Harada N, Miyamoto T, Tomioka T, Yamamoto K, et al. Collective review of small carcinomas of the pancreas. Ann Surg 1986; 203:77-81. [PMID 3942423]
- Jones BA, Langer B, Taylor BR, Girotti M. Periampullary tumours, which ones should be resected? Am J Surg 1985; 149:46-52. [PMID 3966641]
- Siedek M, Birtel F, Mitrenga I. Pankreasgagganastome und Pankreatojejunopicatio nach recctstresektion. Langenbecks Arch Surg 1985; 366:610.
- Trede M. The surgical treatment of pancreatic carcinoma. Surgery 1985; 97:28-35. [PMID 2578229]
- Lerut JP, Gianello PR, Otte JB, Kestens PJ. Pancreaticoduodenal resection. Surgical experience and evaluation of risk factors in 103 patients. Ann Surg 1984; 199:432-7. [PMID 6712319]
- Morrow M, Hilaris B, Brennan MF. Comparison of conventional surgical resection, radioactive implantation, and bypass procedures for exocrine carcinoma of the pancreas 1975-1980. Ann Surg 1984; 199:1-5. [PMID 6419687]
- van Heerden JA. Pancreatic resection for carcinoma of the pancreas: Whipple versus total pancreatectomy--an institutional perspective. World J Surg 1984; 8:880-8. [PMID 6516431]
- Andrén-Sandberg A, Ihse I. Factors influencing survival after total pancreatectomy in patients with pancreatic cancer. Ann Surg 1983; 198:605-10. [PMID 6639161]
- Appelqvist P, Virén M, Minkkinen J, Kajanti M, Kostiainen S, Rissanen P. Operative finding, treatment, and prognosis of carcinoma of the pancreas: an analysis of 267 cases. J Surg Oncol 1983; 23:143-50. [PMID 6865434]
- Björck S, Svensson JO, Macpherson S, Edlund Y. Cancer of the head of the pancreas and choledochoduodenal junction: a clinical study of 88 Whipple resections. Acta Chir Scand 1981; 147:353-9. [PMID 7324762]
- Cooperman AM, Herter FP, Marboe CA, Helmreich ZV, Perzin KH. Pancreatoduodenal resection and total pnacreatectomy--an institutional review. Surgery 1981; 90:707-12. [PMID 7281009]
- Bergstrand O, Ahlberg J, Ewerth S, Hellers G, Holmström B. A retrospective study of carcinoma of the pancreas with special reference to the results of surgical treatment. Acta Chir Scand Suppl 1978; 482:26-8. [PMID 80089]
- Hermreck AS, Thomas CY 4th, Friesen SR. Importance of pathologic staging in the surgical management of adenocarcinoma of the exocrine pancreas. Am J Surg 1974; 127:653-7. [PMID 4134052]
- Longmire WP Jr, Shafey OA. Certain factors influencing survival after pancreaticoduodenal resection for carcinoma. Am J Surg 1966; 111:8-12. [PMID 5901380]
- Gouma DJ, van Geenen RC, van Gulik TM, de Haan RJ, de Wit LT, Busch OR, Obertop H. Rates of complications and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg 2000; 232:786-95. [PMID 11088073]
- Birkmeyer JD, Warshaw AL, Finlayson SR, Grove MR, Tosteson AN. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Surgery 1999; 126:178-83. [PMID 10455881]
- Gordon TA, Bowman HM, Bass EB, Lillemoe KD, Yeo CJ, Heitmiller RF, et al. Complex gastrointestinal surgery: impact of provider experience on clinical and economic outcomes. J Am Coll Surg 1999; 189:46-56. [PMID 10401740]
- Simunovic M, To T, Theriault M, Langer B. Relation between hospital surgical volume and outcome for pancreatic resection for neoplasm in a publicly funded health care system. CMAJ 1999; 160:643-8. [PMID 10101998]
- Glasgow RE, Mulvihill SJ. Hospital volume influences outcome in patients undergoing pancreatic resection for cancer. West J Med 1996; 165:294-300. [PMID 8993200]
- Imperato PJ, Nenner RP, Starr HA, Will TO, Rosenberg CR, Dearie MB. The effects of regionalization on clinical outcomes for a high risk surgical procedure: a study of the Whipple procedure in New York State. Am J Med Qual 1996; 11:193-7. [PMID 8972936]
- Wade TP, Halaby IA, Stapleton DR, Virgo KS, Johnson FE. Population-based analysis of treatment of pancreatic cancer and Whipple resection: Department of Defense hospitals, 1989-1994. Surgery 1996; 120:680-5. [PMID 8862378]
- Lieberman MD, Kilburn H, Lindsey M, Brennan MF. Relation of perioperative deaths to hospital volume among patients undergoing pancreatic resection for malignancy. Ann Surg 1995; 222:638-45. [PMID 7487211]
- Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relation between surgical volume and mortality. N Engl J Med 1979; 301:1364-9. [PMID 503167]
- Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I, et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002; 346:1128-37. [PMID 11948273]
- van Heek NT, Kuhlmann KF, Scholten RJ, de Castro SM, Busch OR, van Gulik TM, et al. Hospital volume and mortality after pancreatic resection: a systematic review and an evaluation of intervention in the Netherlands. Ann Surg 2005; 242:781-8. [PMID 16327488]
- Makary MA, Winter JM, Cameron JL, Campbell KA, Chang D, Cunningham SC, et al. Pancreaticoduodenectomy in the very elderly. J Gastrointest Surg 2006; 10:347-56. [PMID 16504879]
- Bathe OF, Caldera H, Hamilton-Nelson K, Franceschi D, Sleeman D, Levi JU, Livingstone AS. Influence of Hispanic ethnicity on outcome after resection of carcinoma of the head of the pancreas. Cancer 2001; 91:1177-84. [PMID 11267964]
- Eloubeidi MA, Desmond RA, Wilcox CM, Wilson RJ, Manchikalapati P, Fouad MM, et al. Prognostic factors for survival in pancreatic cancer: a populationbased study. Am J Surg 2006; 192:322-9. [PMID 16920426]
- Safi F, Schlosser W, Falkenreck S, Beger HG. Prognostic value of CA19-9 course in pancreatic cancer. Hepatogastroenterology 1998; 45:253-9. [PMID 9496523]
- Safi F, Schlosser W, Falkenreck S, Beger HG. CA 19-9 serum course and prognosis of pancreatic cancer. Int J Pancreatol 1996; 20:155-61. [PMID 9013275]
- Montgomery RC, Hoffman JP, Riley LB, Rogatko A, Ridge JA, Eisenberg BL. Prediction of recurrence and survival by post-resection CA 19-9 values in patients with adenocarcinoma of the pancreas. Ann Surg Oncol 1997; 4:551-6. [PMID 9367020]
- Ni XG, Bai XF, Shao YF, Wu JX, Shan Y, Wang CF, et al. The clinical value of serum CEA, CA19-9 and CA242 in the diagnosis and prognosis of pancreatic cancer. Eur J Surg Oncol 2005; 31:164-9. [PMID 15698733]
- Berger AC, Meszoely IM, Ross EA, Watson JC, Hoffman JP. Undetectable preoperative levels of serum CA 19-9 correlate with improved survival for patients with resectable pancreatic adenocarcinoma. Ann Surg Oncol 2004; 11:644-9. [PMID 15197014]
- Sewnath ME, Birjmohun RS, Rauws EA, Huibregtse K, Obertop H, Gouma DJ. The effect of preoperative biliary drainage on postoperative complications after pancreaticoduodenectomy. J Am Coll Surg 2001; 192:726-34. [PMID 11400966]
- Jagannath P, Dhir V, Shrikhande S, Shah RC, Mullerpatan P, Mohandas KM. Effect of preoperative biliary stenting on immediate outcome after pancreaticoduodenectomy. Br J Surg 2005; 92:356-61. [PMID 15672425]
- Sanfilippo F, Spees EK, Vaughn WK. The timing of pretransplant transfusions and renal allograft survival. Transplantation 1984; 37:344-50. [PMID 6369662]
- Opelz G, Sengar DP, Mickey MR, Terasaki PI. Effect of blood transfusions on subsequent kidney transplants. Transplant Proc 1973; 5:253-9. [PMID 4572098]
- Opelz G, Terasaki PI. Improvement of kidneygraft survival with increased numbers of blood transfusions. N Engl J Med 1978; 299:799-803. [PMID 357971]
- Strumper-Groves D. Perioperative blood transfusion and outcome. Curr Opin Anaesthesiol 2006; 19:198-206. [PMID 16552228]
- Jagoditsch M, Pozgainer P, Klingler A, Tschmelitsch J. Impact of blood transfusions on recurrence and survival after rectal cancer surgery. Dis Colon Rectum 2006; 49:1116-30. [PMID 16779711]
- Hishinuma S, Ogata Y, Tomikawa M, Ozawa I, Hirabayashi K, Igarashi S. Patterns of recurrence after curative resection of pancreatic cancer, based on autopsy findings. J Gastrointest Surg 2006; 10:511-8. [PMID 16627216]
- Phoa SS, Tilleman EH, van Delden OM, Bossuyt PM, Gouma DJ, Laméris JS. Value of CT criteria in predicting survival in patients with potentially resectable pancreatic head carcinoma. J Surg Oncol 2005; 91:33-40. [PMID 15999356]
- Pawlik TM, Abdalla EK, Barnett CC, Ahmad SA, Cleary KR, Vauthey JN, et al. Feasibility of a randomized trial of extended lymphadenectomy for pancreatic cancer. Arch Surg 2005; 140:584-9. [PMID 15967906]
- Hirai I, Kimura W, Ozawa K, Kudo S, Suto K, Kuzu H, Fuse A. Perineural invasion in pancreatic cancer. Pancreas 2002; 24:15-25. [PMID 11741178]
- Pour PM, Brand RE, Kimura W, Bell R. Is there any stage I disease of the pancreas? Pancreatology 2002; 2:342.
- Verbeke CS, Leitch D, Menon KV, McMahon MJ, Guillou PJ, Anthoney A. Redefining the R1 resection in pancreatic cancer. Br J Surg 2006; 93:1232-7. [PMID 16804874]
- Alexakis N, Halloran C, Raraty M, Ghaneh P, Sutton R, Neoptolemos JP. Current standards of surgery for pancreatic cancer. Br J Surg 2004; 91:1410- 27. [PMID 15499648]
- Stocken DD, Büchler MW, Dervenis C, Bassi C, Jeekel H, Klinkenbijl JH, et al. Meta-analysis of randomised adjuvant therapy trials for pancreatic cancer. Br J Cancer 2005; 92:1372-81. [PMID 15812554]
- Oettle H, Neuhaus P. Adjuvant therapy in pancreatic cancer: a critical appraisal. Drugs 2007; 67:2293-310. [PMID 17983252]
- Kleeff J, Michalski CW, Friess H, Büchler MW. Surgical treatment of pancreatic cancer: the role of adjuvant and multimodal therapies. Eur J Surg Oncol 2007; 33:817-23. [PMID 17331695









