Elizabeth Kirkland*
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Jingwen Zhang
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Elisha Brownfield
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Marc Heincelman
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Samuel Schumann
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Andrew Schreiner
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Kinfe Bishu
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Patrick D Mauldin
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
William P Moran
Department of Medicine, Division of General Internal Medicine, Medical University of South Carolina, Charleston, SC, USA
Corresponding Author:
Elizabeth Barnhardt Kirkland, MD MSCR
Department of Medicine, Division of General Internal Medicine
Medical University of South Carolina, 135 Rutledge Ave, MSC 591
12th Floor RT, Charleston, SC, USA 29425, USA
Tel: +01 (843) 876-8653
E-mail: kirklane@musc.edu
Submitted date: August 03, 2017; Accepted date: September 28, 2017; Published date: October 05, 2017
Keywords
Patient-centered care; Healthcare disparities; Hypertension; Quality improvement
How this fits in with quality in primary care?
What do we know?
Health disparities, particularly with regards to chronic disease control, persist in modern medicine. This is partly due to barriers to healthcare access.
What does this paper add?
This study suggests that multidisciplinary, patient-centered care can improve chronic disease rates. These benefits are sustained over five years and do not appear to be dependent on traditional office visits.
Introduction
Despite advances in medicine and access to care over the past several decades, hypertension (HTN) remains a leading cause of morbidity and mortality in the U.S. As recently as 2012, nearly 20% of hypertensive American adults were unaware of their diagnosis, 25% were untreated, and nearly 50% of American adults with HTN were uncontrolled. Perhaps even more concerning is that the age-adjusted rate of HTN-related deaths actually rose by more than 20% from 2000 to 2013 [1]. This is a critical public health concern warranting action, especially as a recent model estimates that treatment of HTN would prevent the largest number of deaths when compared to numerous common preventative services [2]. While all racial and ethnic groups are affected by HTN, there are significant racial disparities in blood pressure (BP) control and HTN-related morbidity and mortality. National health statistics and surveys consistently demonstrate a higher prevalence of HTN [3] and lower age-adjusted rates of HTN control [4] for non-Hispanic blacks compared to non-Hispanic whites. In 2009, black men and women in the US suffered a death rate from high blood pressure (BP) two to three times higher than the overall national population [5]. Multiple factors contribute to these disparities, many of which remain poorly understood. Even more elusive are methods to eliminate those disparities.
One intervention that has been proposed as a strategy to improve patient- and population-level healthcare is the patient centered medical home (PCMH). The Agency for Healthcare Research and Quality (AHRQ) defines PCMH as “a model of the organization of primary care that delivers the core functions of primary health care” with the ultimate goal of achieving “high-quality, accessible, efficient health care for all Americans” (AHRQ) [6]. Early studies suggest that PMCH status is associated with increased healthcare access and quality of care measurements [7,8]. These same factors, access and quality of care, have been cited as factors underlying persistent racial disparities in healthcare provision and outcomes [9]. As such, the PCMH has been touted as a possible means of reducing disparities in healthcare for the American population [8]. Despite the promising findings regarding access and quality, this does not necessarily correlate with clinical outcomes. In fact, current data regarding the association between the PCMH and clinical outcomes are inconclusive [10]. Now, ten years after the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physician, and American Osteopathic Association released a joint statement defining the principles of a PCMH [11], it is critical to assess the impact of this care system on patient-level health.
This quality improvement initiative aimed to measure the effectiveness of PCMH-based interventions on systolic BP (SBP) and HTN control rates for adult Internal Medicine patients with baseline uncontrolled HTN. Additionally, it sought to identify and reduce the magnitude of healthcare disparities between non-white and white patients with respect to HTN control. We hypothesized that PCMH-based quality improvement initiatives would lower quarterly mean SBP and rates of uncontrolled BP for all patients regardless of race. Further, we hypothesized that increased access to care, as indicated by the volume of clinic visits, would lower BP and improve control rates.
Methods
Study population
This quality improvement initiative was conducted at an academic hospital-based primary care Internal Medicine clinic located in the southeast. This clinic cares for approximately 10,000 adult patients, with approximately 38,000 visits per year. All patients aged 18 and older with at least two office visits in the three years prior to PCMH certification were evaluated for inclusion. This led to identification of 9,552 patients who were seen in this clinic between January 2014 and December 2016. Only 5,892 of those patients had a recorded SBP during the one year prior to PCMH certification in October 2011. For those patients, a mean SBP was calculated from all outpatient SBPs recorded during the quarter (three calendar months) prior to PMCH certification. Patients were included in the inception cohort if this quarterly mean SBP was ≥ 140 mm Hg (n=1,702). This cutoff was used to define uncontrolled BP, in accordance with the Eighth Joint National Committee (JNC8) guidelines for adults under 60 years of age [12]. Based on this definition, 100% of the inception cohort had uncontrolled BP during the quarter prior to PCMH certification. In order to calculate change in control rate and SBP value after the intervention, the average of the four quarterly means prior to PCMH certification (a total of 12 months data) served as the baseline measurement.
In October 2011, the clinic became certified as a Level 3 PCMH. Interventions initiated as part of the PCMH specific to hypertension control included identification of patients with uncontrolled SBP. The intervention also included dissemination of this list to medical providers, weekly multidisciplinary team meetings to review at-risk patients and targeted outreach by a patient navigator. The multidisciplinary team included 4 advanced practice providers, 8 registered nurses, 10 licensed practical nurses or certified medical assistants, 3 Doctors of Pharmacy, 2 clinical support staff, 5 registrars, 14 faculty physicians, 96 resident physicians, 1 social worker and 1 outreach navigator. All patients were eligible for the same set of interdisciplinary, PCMH-based interventions, focused mainly on improving blood pressure control by identifying and reducing barriers to care as well as enhancing access through individualized patient outreach and assistance with scheduling follow up appointments. Treatment plans for HTN were determined on a case-by-case basis through provider and patient discussion. There were no treatment algorithms utilized for BP control.
Outcome measures
Once the inception cohort was identified, mean SBP was calculated on a quarterly basis in longitudinal fashion, averaging all recorded BPs during each quarter, from 3rd quarter of 2011 until 3rd quarter of 2016. Both quantitative SBP (in mm Hg) and control rate (defined as proportion of cohort with mean SBP<140 mm Hg) were measured. The primary outcomes included the change in SBP and the change in the proportion of the cohort with BP control over the course of the study. These values were compared based on total number of office visits per year and age categories.
Covariates
Age, gender, race, marital status and smoking status were retrieved from EHR and coded as indicator or continuous variables. Insurance was coded as a category variable including Medicare, Medicaid and Commercial. The average number of office visits per year was calculated based on the total number of visits during the five-year follow-up period divided by five. Patient age was grouped into: age 18-59 years and 60 and older.
Statistical analysis
Proportions of baseline characteristics were compared using Chi-square analysis. Two sample t-test was performed to compare differences between the two independent groups based on presence of normal distribution. One-way ANOVA was used to compare multiple groups, with regards to number of visits. Missing data from quarterly mean SBP were handled using simple imputation via the last quarterly mean carried forward. Statistical significance was determined at the 5% level. Statistical analysis was performed using SAS version 9.3 (SAS Institute, Cary, NC, US). The study was submitted to the MUSC Internal Review Board; it was deemed to fall under the umbrella of quality improvement, and thus the Internal Review Board advised that approval for human research was not required.
Results
Prior to PMCH certification in October 2011, the quarterly mean SBP of all clinic patients (n=9,552; 51.3% non-white, 48.72% white) was 134 mm Hg for non-white adults and 128 mm Hg for white adults. Of these patients, there were 1,702 patients (63% black, 36% white, 1% Asian or other) who met inclusion criteria and thus were included in the inception cohort. Table 1 shows the baseline characteristics of the inception cohort based on racial groups. The mean age of white adults was approximately 67 years while the mean age of nonwhite adults was approximately 63 years. The proportion of males was higher for white adults compared with nonwhite adults (47% vs. 25%, respectively). Medicare and commercial insurance were more frequent among white adults compared with nonwhite adults. Non-white adults were more likely to be unmarried, have Medicaid coverage, smoke cigarettes and have an average of two or more visits per year compared with white adults.
| |
White (n=609) |
Non-white (n=1093) |
P value^ |
| Age (years) |
67.3 ± 13.9 |
62.6 ± 14.8 |
<0.001 |
| Male, n (%) |
287 (47.1%) |
272 (24.9%) |
<0.001 |
| Unmarried, n (%) |
221 (36.3%) |
795 (72.7%) |
<0.001 |
| Insurance, n (%) |
|
|
<0.001 |
| Medicare |
423 (69.7%) |
708 (64.9%) |
|
| Medicaid |
19 (3.1%) |
183 (16.8%) |
|
| Commercial |
165 (27.2%) |
200 (18.3%) |
|
| Smoker, n (%) |
52 (8.5%) |
156 (14.3%) |
<0.001 |
| Average number of visits/year, n |
|
|
<0.001 |
| 0 |
90 (14.8%) |
139 (12.7%) |
|
| 1 = visits<2 |
197 (32.4%) |
256 (23.4%) |
|
| 2 = visits<3 |
147 (21.1%) |
264 (24.2%) |
|
| 3 = visits<4 |
101 (16.6%) |
188 (17.2%) |
|
| Visits = 4 |
74 (12.2%) |
246 (22.5%) |
|
^Chi square analysis
Table 1: Characteristics of inception cohort.
Of the inception cohort, the baseline mean SBP was 149 mm Hg for nonwhites and 145 mm Hg for whites. The final mean SBP was 143 mm Hg for nonwhites and 139 mm Hg for whites. Using these baseline and final values, there was a 6.0 mm Hg reduction in mean SBP for nonwhites and a 6.1 mm Hg reduction for whites (Figure 1a). There was not a significant difference in the absolute BP reduction (p=0.9371). Baseline rates of uncontrolled SBP taken from the 3 quarters prior to inception cohort identification were 70.9% for nonwhites and 64.5% for whites. The rates of uncontrolled SBP during the final four quarters were 52.7% for nonwhites and 45.5% for whites, representing 18.2% and 19.0% absolute reductions, respectively, compared with the baseline control rates (Figure 1b).
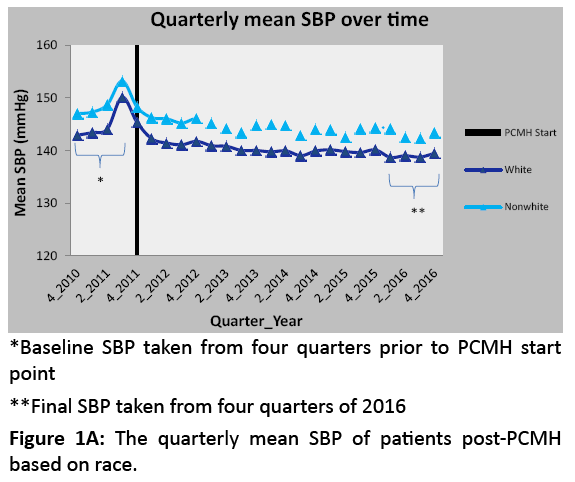
Figure 1A: The quarterly mean SBP of patients post-PCMH based on race.
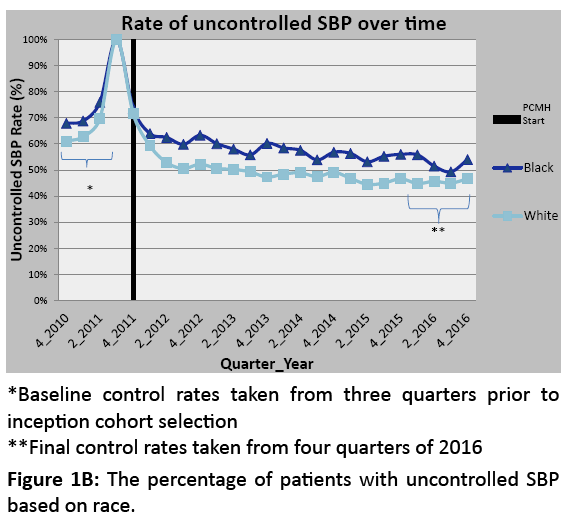
Figure 1B: The percentage of patients with uncontrolled SBP based on race.
Analysis by visit frequency
The decrease in quarterly mean SBP for white and nonwhite patients by average visit number is presented in Table 2. There was no significant difference in SBP reduction based on visit number for white patients (p=0.416) or for nonwhite patients (p=0.489). Additionally, there was no significant difference in the degree of BP reduction for white versus nonwhite patients when adjusted for number of clinic visits.
| # of Visits/Year |
White |
Nonwhite |
p value* |
| visits 0 |
9.1 |
8.4 |
0.750 |
| visits 1 = N<2 |
6.1 |
5.4 |
0.682 |
| visits 2 = N<3 |
5.2 |
6.0 |
0.629 |
| visits 3 = N<4 |
5.0 |
5.4 |
0.849 |
| visits N = 4 |
6.0 |
5.5 |
0.800 |
| p value^ |
0.416 |
0.489 |
|
^One-way analysis of variance (ANOVA) *two sample t-test
Table 2: Decrease in SBP (in mm Hg) from pre-PCMH to 5 years post-PCMH implementation.
Analysis by age
The quarterly mean SBP decreased for all groups over the 5 years, regardless of race and age (Figure 2). The degree of quarterly mean SBP reduction, measured in mmHg, for white and non-white patients by age is presented in Table 3. Among patients aged 18 to 59, there was an average SBP decrease of 9.8 mm Hg for whites and 6.9 mm Hg for nonwhites over the five-year follow-up period. This does not meet statistical significance, but does suggest a trend in the direction favoring a greater BP reduction for young white adults compared to young nonwhite adults (p=0.0683). Among the older cohort, ages 60 and up, there was no significant difference in SBP reduction for whites versus nonwhites (p=0.6017).
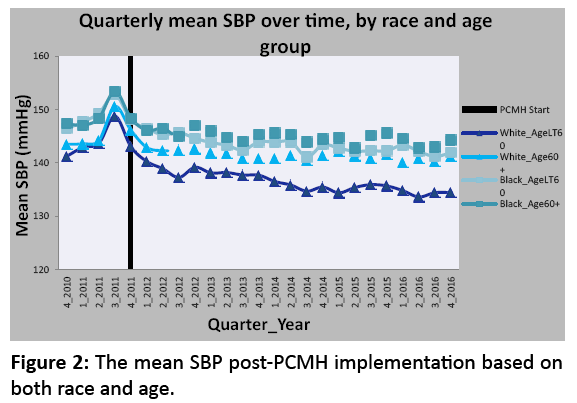
Figure 2: The mean SBP post-PCMH implementation based on both race and age.
When comparing the age cohorts within the same racial group, young white adults had a greater BP reduction than their older white counterparts which met statistical significance at the p<0.05 level (9.8 mm Hg versus 4.9 mm Hg SBP reduction for young versus older white adults (Table 3). In comparison, there was not a statistically significant difference in the SBP reduction for young versus older nonwhite adults (6.9 mm Hg and 5.4 mm Hg SBP reduction, respectively; p=0.1530).
Discussion
Level 3 PCMH status and implementation of PMCH-based initiatives are associated with improved hypertension control in an academic-affiliated hospital-based primary care Internal Medicine clinic. These findings are consistent with those presented in a systematic review in which similar strategies of patient identification, outreach and follow up were shown to improve chronic disease control [13].
With regards to racial differences, both white and nonwhite patient populations demonstrated a significant reduction in quarterly mean SBP and rate of uncontrolled HTN over the five years following PCMH certification in October 2011. The degree of SBP reduction, 6 mm Hg, is similar to that reported in other studies and has been shown to improve HTN-related morbidity and mortality [13]. There was not a statistically significant difference in the degree of SBP reduction for white versus nonwhite adults, suggesting that the PCMH-based initiatives do not differentially affect one racial population compared to the other. The rate of SBP control was also improved for both racial groups to a similar degree. This is encouraging, as the current findings suggest that the quality improvement initiatives set forth by the PCMH are beneficial for patients of varying backgrounds. Similar findings have been reported by Shi et al. [10]. In that study, using HRSA’s 2009 Uniform Data System and Commonwealth Fund National Survey of Federally Qualified Health Centers, there was not a statistically significant difference in BP control rates among minority versus total populations in PCMH clinics.
Nevertheless, the results show that disparities in BP control persist despite equal effect of the intervention. The nonwhite population had a higher baseline mean SBP and lower rate of HTN control compared to their white counterparts. This pattern did not change after PCMH certification. At all-time points, the percentage of patients with controlled SBP was higher and the mean SBP was lower for whites compared to non-whites. Results from this cohort also show that the rate of HTN control varied across time for both groups.
Furthermore, the study results and analysis demonstrate that the threshold for “control” was not met for a larger proportion of the nonwhite population due to a higher baseline BP. Taken as a whole, the nonwhite adult population from the inception cohort had a starting mean SBP of 149 mm Hg and a final mean SBP of 143 mm Hg, representing a 6.0 mm Hg drop. Their white counterparts started with a mean SBP of 145 mm Hg and decreased by 6.1 mm Hg to 139 mm Hg. The final mean SBP for non-whites was just above the threshold for SBP control while the whites dropped just under the threshold. This underscores the importance of taking into account more than a dichotomous outcome or threshold.
Another important finding from the current study is that of BP reduction as it pertains to traditional office visits. Analysis of mean SBP based on number of visits suggests that the degree of SBP reduction is not dependent upon the number of office visits. This is true when analyzed by age and race independently. One explanation for this finding is that other means of outreach, such as unscripted motivational interviewing performed by an outreach coordinator, may prompt patients to improve medication compliance or make other lifestyle changes that reduce BP. Prior work has suggested that similar nurse-based intervention is effective in improving HTN control [14]. Regardless, these findings have implications for future quality improvement initiatives. This work suggests that bringing patients into the medical office may not be the most effective method to improve patient-centered outcomes. Similarly, this finding challenges the tendency to point to lack of access to care as a main driver of poorly controlled chronic disease.
Interestingly, when accounting for age and race together, the analysis of mean SBP reduction suggests that young white adults experience a greater BP improvement than older white adults. This may be explained by less aggressive treatment in keeping with JNC8’s more liberal blood pressure target of 150/90 for adults age 60 and up. There is also a trend towards greater BP reduction for young white adults compared to young nonwhite adults. There may be other variables influencing this trend that were unable to be analyzed in this study.
Strength
A strength is the duration of follow up. Five years is a significantly longer follow-up period than that used in the vast majority of hypertension studies performed to date. Given the difficulty in sustaining chronic disease control over time, these findings are unique and encouraging. Additionally, this study analyzes BP control with regards to frequency of traditional office visits. This is an area of particular interest as the Seventh Joint National Committee (JNC7) has advocated for monthly office visits until BP control is achieved [15]. A randomized trial aimed at further addressing this issue is currently underway [16].
Future investigation is needed to identify the factors that lead to improved BP control for those patients who have few office visits. The clinic in this study adopted a new electronic medical record in 2012. Patient-physician communication through this EMR was made accessible in the third quarter of 2012 and has been increasingly utilized by patients in recent years. It is possible that some of the BP reduction can be attributed to nontraditional modes of physician-patient communication, although it is unlikely that this fully explains the BP reduction. Determination of these factors will be critical to optimizing BP control in the future.
Limitations
This was a single-center, retrospective inception cohort study susceptible to selection bias and regression to the mean. Patients were included in the inception cohort based on an outof- control BP in the quarter prior to PCMH certification. By nature of this design, there is a high risk of regression to the mean. This is evidenced by the finding that patients who have <1 visit per year have the largest decrease in blood pressure (Table 2). In order to limit the inherent risk of regression to the mean, the averages of four quarterly SBP means were utilized as the baseline and final values.
Other limitations inherent to the study design are that of non-standardized BP measurement and missing data. Quarterly mean SBP was calculated based on any outpatient SBP available in the medical record during that quarter. These readings could have been from any outpatient clinic site, regardless of specialty or reason for visit. Elevations due to acute illness or differences in measurement technique could not be accounted for in this analysis. Additionally, not all patients had a recorded outpatient BP during every quarter of the follow up period. Missing data were handled via imputation, with the last quarterly mean carried forward.
Conclusion
The data presented herein suggest that PMCH-based quality improvement initiatives are equally effective in achieving SBP reduction and BP control among patients of differing racial backgrounds. While there is no evidence of a narrowing of disparities in BP control by race, the results are significant for improved BP control in both population groups. Additionally, the results suggest that access to traditional office visits does not affect BP control. This finding, in conjunction with the notable sustained BP reduction over five years, suggests that non-traditional models of care delivery may be the future of chronic disease management.
Ethical Approval
This project was deemed exempt from IRB approval based on its classification as a Quality Improvement Initiative.
Source of Funding
Internal funding support was provided by the Medical University of South Carolina. There was no external funding.
Acknowledgement
We thank Justin Marsden for data management and support and William Barry for patient outreach and care coordination.
References
- Kung HC, Xu J. Hypertension-related mortality in the United States, 2000-2013. NCHS Data Brief 2015; 2015: 1-8.
- Farley TA, Dalal MA, Mostashari F, Frieden TR. Deaths preventable in the U.S. by improvements in use of clinical preventive services. Am J Prev Med 2010; 38: 600-609.
- Yoon SS, Ostchega Y, Louis T. Recent trends in the prevalence of high blood pressure and its treatment and control, 1999-2008. NCHS Data Brief 2010; 2010: 1-8.
- Yoon SS, Burt V, Louis T, Carroll MD. Hypertension among adults in the United States, 2009-2010. NCHS Data Brief2012; 2012: 1-8.
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, et al. Heart disease and stroke statistics--2013 update: A report from the American Heart Association. Circulation 2013; 127: e6-e245.
- https://pcmh.ahrq.gov
- Reid RJ, Fishman PA, Yu O, Ross TR, Tufano JT, et al. Patient-centered medical home demonstration: A prospective, quasi-experimental, before and after evaluation. Am J Manag Care 2009; 15: e71-e87.
- Beal AC, Doty MM, Hernandez SE, Shea KK, Davis K. Closing the divide: How medical homes promote equity in health care, results from the commonwealth fund 2006 health care quality survey. The Commonwealth Fund 2007.
- Mueller M, Purnell TS, Mensah GA, Cooper LA. Reducing racial and ethnic disparities in hypertension prevention and control: What will it take to translate research into practice and policy? Am J Hypertens 2015; 28: 699-716.
- Shi L, Lock DC, Lee DC, Lebrun-Harris LA, Chin MH, et al. Patient-centered medical home capability and clinical performance in HRSA-supported health centers. Med Care 2015; 53: 389-395.
- Joint principles of the patient-centered medical home. Del Med J 2008; 80: 21.
- James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311: 507-520.
- Glynn LG, Murphy AW, Smith SM, Schroeder K, Fahey T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst Rev 2010; 2010: Cd005182.
- Rudd P, Miller NH, Kaufman J, Kraemer HC, Bandura A, et al. Nurse management for hypertension: A systems approach. Am J Hypertens 2004; 17: 921-927.
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, et al. The seventh report of the joint national committee on prevention, detection, evaluation and treatment of high blood pressure: The JNC 7 report. JAMA 2003; 289: 2560-2572.
- Fiscella K, Ogedegbe G, He H, Carroll J, Cassells A, et al. Blood pressure visit intensification study in treatment: Trial design. Am Heart J 2015; 170: 1202-1210.

