Ilias N Karampelas1, Kostas N Syrigos2, Muhammad Wasif Saif3
1Oncology Department, Athens Medical Group, Athens, Greece.
2Oncology Unit, Third Department of Medicine, University of Athens. Athens, Greece.
3Section of GI Cancers and Experimental Therapeutics, Tufts University School of Medicine. Boston, MA, USA
- *Corresponding Author:
- Ilias N Karampelas
Oncology Department
Athens Medical Group
Athens
Greece
E-mail: iliasnkarampe@gmail.com
Keywords
Cancer; Diabetes; Hyperinsulinemia; Pancreatic Cancer
What Did We Know Before ASCO 2014?
Neuroendocrine tumors (NETs) are uncommon, with an estimated incidence of 2.5-5 per 100,000 people per year and prevalence of 35 per 100,000 [1]. Survival rates vary by primary site and are higher in patients with well-differentiated tumors, and with locoregional versus distant disease [2]. Most of the tumors are insulinomas, glucagonomas, gastrinomas, somatostatinomas, VIPomas, pancreatic polypeptidomas and cholecystokininomas. Based on histology they are divided in three categories, well differentiated/low grade, well differentiated/ intermediate grade and poorly differentiated/high grade. Although, resection of localized disease can prove curative, metastases are already present, in most of the cases, in the time of the diagnosis, so the tumor is unresectable just from the beginning [3]. For patients with well differentiated or moderately differentiated pancreatic NETs (pNETs) with distant metastatic disease, the median survival time is 24 months [3]. In April 2011 the FDA approved molecularly targeted agents, everolimus, tyrosine kinases, mammalian target of rapamycin (mTOR), and vascular endothelial growth factor receptors (VEGFR) have been used with success in the treatment of gastroenteropancreatic NET. This approval was based on RADIANT-3 study, which was first reported at the ASCO GI Symposium in January 2011 [4]. A phase III trial looked at sunitinib in unresectable pNET and found an improvement in progression free survival from 5.5 to 11.4 months when compared to placebo [5]. Concerning to somatostatin analogs, can be used to control symptoms associated with carcinoid syndrome [6]. Short and long acting octreotide remains the most widely used somatostatin analog. In 2009, the PROMID trial demonstrated that the use of octreotide improved median time to progression to 14.3 months [7]. In 2013, follow up data of PROMID trial improve an increasing overall survival [8]. In 2013, Bajetta et al. presented a phase II data suggesting that the addition of everolimus to octreotide therapy benefits progression free survival (16.3 months) in the first line setting when treating advanced gastroenteropancreatic NET [9].
What We Learn at ASCO 2014?
This paper summarizes the recent work presented at the 2014 ASCO Annual Meeting, regarding in targeted agents in treatment of neuroendocrine tumors of pancreas. The purpose of this paper is to present the data of the two presented abstracts.
Updated Overall Survival and Time to Progression Results in Nets Treated with Everolimus Combination with Octreotide LAR as First-Line Treatment.
Emilio Bajetta et al. performed an analysis to evaluate the objective response rate (ORR), a further prolongation of the median time to progression (TTP) and the overall survival (OS), suggesting a possible long term benefit of the combination of everolimus with octreotide LAR as first-line treatment (Abstract #15160 [10]) (Table 1). A total of 50 patients with advanced well differentiated, previously untreated NETs of a gastroenteropancreatic (GEP) tract and of a lung were studied, for a period of 17.8 months. They received everolimus in combination with octreotide LAR. The results of the study shows that the treatment was effective and well tolerate. One patient had a complete response, 16% partial response and 72% stable disease. Eleven patients with NETs of the GEP tract are still benefiting from the treatment. However, more research on this combination is required.
Durable Disease Control with Sunitinib and Everolimus in Well-Differentiated Neuroendocrine Tumors of the Pancreas with a High ki67 Index.
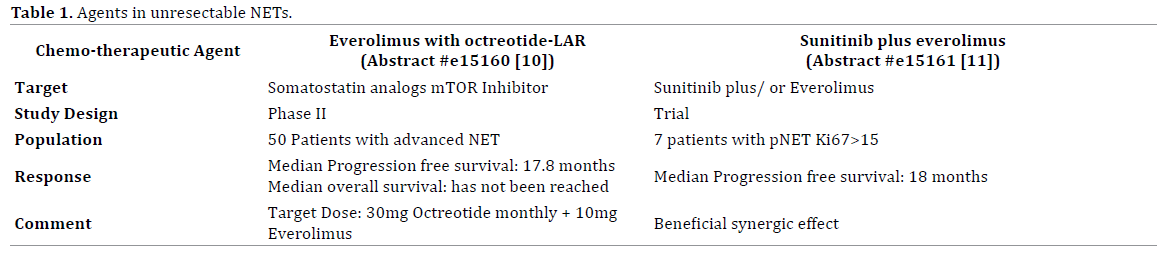
Karen Paula Geboes et al. presented the results of a study, analyzing patients with well-differentiated neuroendocrine tumors of the pancreas, with a high ki67 index, who received sunitinib and everolimus in order to control durable disease (Abstract #15161 [11]) (Table 1). Furthermore, patients had an uptake of lesions on octreoscan and/or gallium68 dotatoc. A total of 7patients with advanced well differentiated NET of the pancreas, with median ki67 index 23 (IQR: 16–38%), were studied. The disease was controlled for a median of 18 (14-23) months on sunitinib and/or everolimus. The longer duration of disease control in more patients warrants further investigation.
Discussion
Surgical resection remains the gold standard of treatment for patients with localized disease. However, most NETs are unresectable at diagnosis or progress after local treatment and there have been relatively few treatments options. Traditional systemic treatment options for pancreatic NETs include somatostatin analogs or cytotoxic chemotherapy. Patients with pNETs have been reported to cause response 23%-70%. [12]. New treatments have come up recently. Everolimus, an mTOR inhibitor which inhibits cell growth, proliferation, and angiogenesis, and has been shown to prolong progression free survival compared to placebo. Sunitinib is a multi-kinase inhibitor effective in NET through inhibition of VEGF [13]. Both agents provide clinical benefit for patients with NETs. Somatostatin analogs have been shown to be efficacious in the treatment of gastroenteropancreatic NET. Previously presented phase II study data shows that the combination of everolimus and octreotide LAR in the first line treatment for advanced NETs is an active and a safe solution [9]. It was necessary to know if there is a further prolongation of the median time to progression (TTP), suggesting a possible long term benefit of this combination. In Abstract #e15160 [10], Emilio Bajetta et al. demonstrated that there is a prolonged benefit of everolimus in combination with long acting somatostatin analogs in NETs. Interestingly, this trial showed that everolimus could be combined with somatostatin analogs without affecting the safety profile of either everolimus or somatostatin analogs.
Tumors with a high histologic grade, a mitotic count >20 per 10 high-powered fields (HPF), or a Ki-67 proliferation index of >20% represent aggressive neuroendocrine carcinomas that have a different natural history and response to treatment compared to low-grade, welldifferentiated tumors. In Abstract #e15161 [11], Geboes et al. reported that there was benefit of sunitinib and/ or everolimus in durable disease control in patients with a well differentiated NET of the pancreas. The beneficial synergistic effect, on durable disease, when combining everolimus with sunitinib, presents us promising possibilities in treating our patients with pancreatic NETs. This opens the door to using mTOR inhibitors with other molecularly targeted agents.
Conflict of Interest
Authors declare to have no such conflict of interest.
References
- KjellÖberg, Daniel Castellano. Current knowledge on diagnosis and staging of neuroendocrine tumors. Cancer and Metastasis Reviews, March 2011, Volume 30, Issue 1 Supplement, 3-7.
- Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Ann Oncol. 2008; 19: 1727-1733.
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, Abdalla EK, et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J ClinOncol. 2008; 26:3063-3072. [PMID:18565894]
- Shah MH, Ito T, Lombard-Bohas C, Wolin EM, Van Cutsem E, Sachs C, Winkler RE, et al. Everolimus in patients with advanced pancreatic neuroendocrine tumors: Updated results of a randomized, doubleblind, placebo-controlled multicenter phase III trial (RADIANT-3). J ClinOncol. 2011; 29(Suppl. 4):158.
- Rubin J, Ajani J, Schirmer W, Venook AP, Bukowski R, Pommier R, Saltz L, et al. Octreotide acetate long-acting formulation versus open-label subcutaneous octreotide acetate in malignant carcinoid syndrome. J ClinOncol. 1999; 17(2):600. [PMID:10080605]
- Raymond E, Dahan L, Raoul J-L, Bang YJ, Borbath I, Lombard- Bohas C, Valle J, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:501-13.
- Rinke A, Müller HH, Schade-Brittinger C, Klose KJ, Barth P, Wied M, Mayer C, et al. Placebocontrolled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J ClinOncol. 2009; 27(28):4656. [PMID:19704057]
- Arnold R, Wittenberg M, Rinke A, Schade-Brittinger C, Aminossadati B, Ronicke E, Gress TM, et al. Placebo controlled, double blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors (PROMID): Results on long-term survival. ASCO 2013 Abstract No: # 4030.
- Bajetta E, Catena L, Fazio N, Pusceddu S, Biondani P, Blanco G, Ricci S, et al. Everolimus in combination with octreotide LAR as the first-line treatment for advanced neuroendocrine tumors: A phase II trial of the I.T.M.O. (Italian Trials in Medical Oncology) group. ASCO 2013 Abstract No: #4136.
- Bajetta E, Catena L, Pusceddu S, Spada F, Fazio N, Blanco G, Ricci S, et al. Updated overall survival and time to progression results in NETs treated with everolimus combination with octreotide LAR as first-line treatment. J ClinOncol. 32, 2014 (suppl; abstr#e15160).
- Geboes KP, Laurent S, Verroken C, Cesmeli E, Lambert B, Smeets P, Vanlander A, et al. Durable disease control with sunitinib and everolimus in well-differentiated neuroendocrine tumors of the pancreas with a high ki67 index. J ClinOncol. 32, 2014 (suppl; abstr#e15161).
- Kulke MH. Systemic therapy for advanced pancreatic neuroendocrine tumors. SeminOncol. 2013; 40(1): 75-83. [PMID:23391115]
- Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell. 2005; 8: 299-309. [PMID:16226705]

