Keywords
Postsecondary academic courses; Contribution; Adults with ID; Crystallized and fluid tests; Cognitive Activity Theory
Theoretical Background
Following the Cognitive Activity Theory [1, 2] examined the impact of participation in leisure and cognitively-stimulating activities on the short-term cognitive performance of individuals with nonspecific intellectual disability (NSID) and with Down syndrome (DS). Hierarchal regressions indicated that participation in cognitively-stimulating activities contributed significantly to the explained variance of most of the crystallized and fluid tests. In this follow-up study, we investigated whether the participation of adults with intellectual disability (ID) with and without DS in postsecondary education (PSE) in the form of academic courses may contribute to their cognitive performance beyond other cognitively-stimulating activities in which they engage.
The 21st century introduced a new phenomenon among adults with ID. Improvements in medical care, nutrition, and public health policies have led to an increase in the life expectancy of the general population as well as of the population with ID with and without DS [3]. Even, adults with DS are experiencing greater longevity and may reach their seventies and eighties [4]. People with ID, estimated at approximately 60 million worldwide, represent one of the largest groups of people with lifelong disabilities. Their longer lifespan has presented researchers and care-providers with a new challenge: Development of healthservices, occupational, social, leisure and cognitive programs for this older adult population [3].
Compensation versus Stimulation Interventions for Delaying Old Age
Cognitive training for delaying old age of adults with typical development (TD) has grown significantly, leading to its implementation in hospitals, community programs, and institutions for the elderly [5]. Two types of cognitive interventions aimed at delaying aging in the general population: "Compensation-focused interventions" versus "Stimulation-non focused training" were distinguished [6]. The former type of intervention is designed to enhance frontal mediating functions or compensate for specific cognitive functions that are adversely affected by aging, and was applied in a population with ID. "Stimulation-non focused training" [6] consists of sensory or nonspecific stimulation which is not directed towards a specific cognitive skill, but is rather conducted indirectly through leisure activities. Our study focused on the latter type.
In a series of studies, Lifshitz and her colleagues found that adults with ID (CA=20-70; IQ 40-70) can benefit from focused cognitive interventions aimed at ameliorating specific cognitive skills that are prone to decline with age, such as verbal abstraction skills, orientation in time and space [7, 8] and analogical reasoning [9].
Based on these and other studies [10], developed the Compensation Age Theory (CAT). The CAT postulates that the weight of the chronological age (CA) plays an important role in determining the cognitive ability of individuals with ID beyond their mental age (MA). The CAT claims that in later years, there is compensation for the developmental delays experienced by individuals with ID in their early years. Furthermore, the cognitive ability of adults with ID can be modified at a critical period which was considered to be non-modifiable, even at an advanced age. The last statement of the CAT is that not only endogenous factors (age, etiology, IQ level), but also exogenous factors such as lifestyle (i.e., types of leisure activities), determine their cognitive functioning.
This study is the second to examine the impact of lifestyle, i.e., participation in various types of cognitively-stimulating activities, on the cognitive performance of adults with ID. Our argument is that years of schooling, greater maturity and cumulative life experience help them acquire skills that were previously absent from their behavioral repertoire.
The Structural Cognitive Modifiability Theory and the Mediated Learning Experience [11, 12], which is at the base of the Compensation Age Theory, postulate that the human organism is accessible to change as a result of environmental intervention, even in the presence of three formidable obstacles that are usually believed to prevent change: age, etiology, severity of limitation.
The Cognitive Reserve Theory [13] also underlies the Compensation Age Theory. The Cognitive Reserve Theory [14] postulates that individual differences in the way tasks are processed might provide a differential reserve against brain pathology or age-related changes. A sub-concept of the CR theory is the “neural reserve”, which represents the capacity to perform tasks or cope with increasing task difficulty. The viewpoint that “the adult brain is adaptive at any age and has lifelong capacity for change” is on the rise [5]. Individual differences in cognitive reserve may result from innate characteristics (e.g., intelligence), or may be modulated by life events such as educational or occupational experiences or leisure activities [13, 17] Due to their lower intelligence, fewer educational, occupational, and leisure activities opportunities, it is assumed that individuals with ID will exhibit less CR than their peers without ID [14]. However, studies questioned the applicability of the CR theory to individuals with ID. If people with ID have reduced CR compared with their peers with TD, by definition, then these persons would be expected to be at greater risk for dementia of the Alzheimer type (DAT) with increasing age than the general population [15]. However, several studies [14, 16, 17] found an equivalent or even lower risk of dementia among adults with ID with a nonspecific etiology (NSID). Based on the lower age for onset of DAT among individuals with ID, the above authors reached the conclusion that factors that determine intelligence may have little or no direct relationship to risk for dementia in individuals with NSID.
However, as stated, Lifshitz and colleagues [7-9] indicated that cognitive performance of adults with ID might be modulated by mediation and environmental intervention. The idea of a compensation mechanism developing with an increase in age in individuals with ID is also supported by genetic and brain studies. Head et al. (2007) suggested that in people with DS, overexpressed genes produce proteins that are critical for neuron and synapse growth, development and maintenance, thus providing further evidence for the activation of plasticity mechanisms in this etiology. With aging, these genes may paradoxically participate in molecular cascades supporting neuronal compensation. Our study is the first to address the effect of participation in nonfocused cognitively-stimulating activities on crystallized and fluid tests among adults with ID.
Cognitively-Stimulating Activities among Adults with ID
One of the most meaningful theories in modern gerontology is the Cognitive Activity Theory [2, 18] This theory postulates that participation in cognitive activities during midlife has short and long-term effects. This participation is associated with current cognitive functioning and with reducing the risk of cognitive decline which leads to Alzheimer's disease [2, 19]. Although the mechanisms underlying these associations are not well understood, cognitively-stimulating activities have been posited to contribute to the above-mentioned CR.
Wilson et al. [2] constructed a scale of pursuits that are more and less cognitively-stimulating. The hypothesis is that even external and novel stimuli can lead to rewiring or restoring synaptic connectivity in the brain [6] For instance, music or auditory stimulation might affect attention, auditory discrimination, working memory, or executive function [6].
The idea of using leisure activities to introduce cognitive concepts has not been envisioned in a population with ID until now. Leisure activities among adults with ID were used as a means for improving satisfaction and wellbeing [20], quality of life [21], or self-concept [22, 23].
Lifshitz et al. [1] examined the applicability of the Cognitive Activity Theory [19] among adults with NSID and with DS in the short term. Hierarchal regression indicated that not only the frequency, but also the cognitive load of the activities influenced their cognitive functioning. That is, less cognitively demanding activities (including painting, dancing) contributed significantly to the explained variance of only one cognitive test. However, participation in a number of cognitively demanding activities (including table games, watching TV, reading, using technological devices, participating in academic courses) contributed significantly to the explained variance of most of the crystallized and fluid tests.
Postsecondary Academic Courses for Adults with ID
Inclusion of people with disabilities [24], particularly those with ID, in postsecondary education (PSE) is on rise. The University of Alberta, Canada [25], was one of the first to open its gates to students with ID, followed by Flinders and Deakin universities in Australia [26] and New Zealand. In the US, there are 149 programs across 37 states that accept students with ID [24]. Students with ID attend and audit selected undergraduate classes or complete separate courses tailored to their level [25]. Other PSE programs focus on social and vocational skills [27]. These programs are considered to be leisure activities, since some are held in the afternoon and some in the morning. Students receive a certificate of participation in these programs.
While most PSE programs are intended for young adults with ID (CA 20-35), the age of the adults with ID who participate in academic courses at Bar-Ilan University is not limited, and currently ranges between 25 and 59. In our PSE program, students with mild ID attend the School of Education of the Bar- Ilan University once a week for two academic courses adapted to their level, such as: Developmental Psychology, Sociology, Geography, Self-advocacy, etc. In their second year, the students are included in a typical undergraduate research seminar on "Lifelong Learning of Individuals with Disability".
The educational objectives of our PSE program are for the participants to acquire knowledge on academic subjects that might be relevant for them, develop strategies for learning, and access the university's libraries, conduct small research projects and use the computer lab. The social objectives are to expose students with ID to students with TD in class and during breaks, expand the friendship circle of students with ID, empower and strengthen their self-image, confidence, and quality of life, as well as to construct positive attitudes towards individuals with disability among the regular students.
Research on the contribution of participation in PSE on the cognitive functioning of participants with ID is scant. Following the Cognitive Activity Theory [2, 18], we were eager to examine whether participation in PSE aiming to impart academic knowledge provides a unique contribution to the crystallized and fluid tests performance of adults with ID, beyond other cognitively-stimulating activities in which they engage during the week.
Crystallized and Fluid Intelligence in Adults with ID
Crystallized intelligence was redefined [28] as “a person’s acquired knowledge of the language, information and concepts of a specific culture’’ (p: 5). It is considered a “maintained” ability that increases into the 60s and then declines. Fluid intelligence is defined as “the use of deliberate and controlled mental operations to solve novel problems that cannot be performed automatically” (p: 5). Fluid intelligence is a “vulnerable” ability, peaking in the early 20s and then declining [29]. The crystallized and fluid tests in this study can be regarded as markers for these constructs.
Research on crystallized and fluid intelligence among adults with NSID and with DS is scant. In Devenny et al. [16], adults with NSID and DS improved their fluid scores until their 40s, and maintained them until their 50s. Contrary to the crystallized and fluid evolution in the general population, Kittler, Krinsky-McHale and Devenny [30] found deterioration in the verbal subtests of the WISC-R over a 7-year period among adults with ID. However, Facon [17] found a similar evolution of the WAIS-R verbal and performance scales among adults with NSID and with DS and that of adults with TD. These mixed results make it hard to predict differences in performance on fluid and crystallized tests between participants with ID with and without DS. There are no reports on differences in leisure activities between these etiologies.
The operative goals of this study were: (1) To examine the effect of participation in PSE versus other cognitively-stimulating activities on crystallized and fluid tests performance of adults with NSID and with DS, (2) To examine whether different patterns of performance on the crystallized and fluid tests would be found between participants with NSID and with DS, and (3) To examine whether differences in the crystallized and fluid tests would be found between two age groups (25-45 versus 45-59).
Method
Participants
The sample included 49 participants divided into two groups: Adults with ID who participated in the PSE academic program in Bar-Ilan University (experimental group: N=21), and adults with ID who participated in various types of cognitivelystimulating activities, but not in the PSE (control group: N=29). The participants in the experimental group were recruited from a larger study [31] examining the ability of adolescents and adults with ID with and without DS to acquire metaphorical language. We used their crystallized and fluid tests scores.
Chronological age: The CA range of the experimental group was CA=26-50; M=35.62, SD=6.81, and that of their controls was CA=25.5-59; M=37.10, SD=9.80, with no significant difference between groups, F (1,48)=0.36, p=0.55, ηp2=0.01.
Basic cognitive level: The two groups were matched according to two subscales of the "Abstract Verbal Thinking", a Hebrew verbal intelligence test [32] Synonyms and verbal analogies, with no significant difference between the groups. Table 1 presents the background characteristics of the two groups (Table 1).
| |
PSE (N=21) |
Control (N=29) |
|
| Background characteristic |
M |
SD |
Range |
M |
SD |
Range |
F |
p |
ηp2 |
| CA |
35.62 |
6.81 |
26-50 |
3 7 . 10 |
9 .8 0 |
2 5.5 -5 9 |
0.36 |
0.55 |
0.01 |
| Tables Game |
1.05 |
0.92 |
0-2 |
0.93 |
0.84 |
0-2 |
0.22 |
0.64 |
0.00 |
| TV |
0.86 |
.96 |
0-1 |
0.93 |
0.26 |
0-1 |
0.72 |
0.40 |
0.01 |
| Reading |
2.29 |
1.31 |
0-3 |
1.45 |
1.53 |
0-3 |
4.12* |
0.05 |
0.08 |
| Technological device |
2.86 |
1.85 |
0-4 |
2.03 |
2.01 |
0-4 |
2.18 |
0.15 |
0.04 |
| PSE–academic courses |
5 . 71 |
1. 31 |
0- 6 |
1.4 1 |
1. 55 |
0- 6 |
1 62 . 13 *** |
0.00 |
0.7 7 |
| Synonyms |
4. 71 |
2.63 |
1-10 |
4.34 |
1.65 |
2-8 |
0.37 |
0.54 |
0.01 |
| Analogy |
4.71 |
2.67 |
1-11 |
3.93 |
1.89 |
1-8 |
1.48 |
0.23 |
0.03 |
*p<0.05;***p<0.001
Table 1: Background characteristics (CA, cognitive level, cognitive activities) of participants in the PSE and control groups.
Etiology
Of the sample, 28 (56%) were individuals with NSID and 22 (44%) were individuals with DS, with no significant difference in etiology distribution between the experimental and control groups, χ2(1)=1.03, p=31. There was no significant difference in the CA between the two etiologies (MCA=35.66, SD=8.89; MCA=37.52; SD=8.37 for the NSID and DS etiologies, respectively) F (1,48)=0.57, p=0.45, ηp2=0.01.
All participants reside in community residence and work in vocational centers under the supervision of the Division of Intellectual Disability of the Israel Ministry of Welfare. They met the DSM-5 criteria of adults with mild/moderate ID [33] were independent in Activities of Daily Living (ADL) skills and were without maladaptive behavior. Both groups have the same background characteristics. As will be shown, the adults with ID in the two groups participated in the same four leisure activities (table’s games, watching TV, reading, using technological device). The experimental group participated in the PSE academic courses at the university. The control group participated in courses which deal with current events and the self-advocacy of adults with ID. The required strategies were PowerPoint and oral presentations (stages 1, 2 in the academic courses, Table 2). The courses were given by special education teachers.
| Activity |
The cognitive load and strategies |
Score |
| Table games Cards, puzzles, chess, checkers |
Basic concepts: Color, size, shape, comparison, classification, generalization Math concepts: Quantity, numbers, addition, subtraction, planning |
0.5-1 |
| Listening to the radio, watching television |
Bloom's taxonomy adapted for populations with ID (Luftig[36]), comprehension, remembering, association, analysis, synthesis |
1 |
| Reading short paragraphs, newspapers, short books |
Reading skills Bloom's taxonomy adapted for population with ID (Luftig[36]): Comprehension, remembering, association, analysis, synthesis |
2 |
| Using technology device iPad, tablet, computer for games, searching the internet, building a website |
Reading and writing Bloom's taxonomy adapted for population with ID (Luftig[36]): Comprehension, remembering, association, analysis, synthesis Searching skills, planning, organization+comprehension, remembering, association, application, analysis, synthesis, evaluation |
(Range 2-4) 2 2 Total: 4 |
| Participating in academic courses in the facilities/participating in PSE in colleges or universities (range 1-6) |
| PowerPoint comprehension |
Identification of titles, new words, keywords, distinguishing between principal and secondary details, asking and answering questions |
1 |
| Oral comprehension |
Bloom's cognitive taxonomy Remembering, comprehension, association, application, analysis, synthesis, evaluation |
1 |
| Reading comprehension of text |
Identification of titles, new words, keywords, distinguishing between principal and secondary details, asking and answering questions |
1 |
| Social interaction, evaluation and criticism |
Group work on tasks, discussions, asking and answering questions, association - giving personal examples, doing class work, self-evaluation |
1 |
| Studying for examination |
Focus on main topics, reading and summarizing written material, searching for the correct answer to questions |
1 |
| Meta cognitive skill and research tasks |
Planning, organization, implementation of previous knowledge, working memory and long-term memory, organization precision, focus on details, abstraction and expansion, comparison, drawing conclusions, and meta-cognitive processes |
1 |
| Total |
6 |
Table 2: The cognitive load of the five cognitively-stimulating activities.
The experimental group participated in the PSE program at Bar-Ilan University due to the fact that their services providers were aware of their need to participate in such a project at the university. It is possible that the control group will also participate in academic enrichment at the university in the coming year.
Assessment of Participation in Cognitively-Stimulating Leisure Activities
The Participation in Cognitively-Stimulating Activities Questionnaire [1] was used. The original scale is divided into two parts: (a) Participating in leisure activities which are more cognitively-stimulating and (b) activities which are less cognitivelystimulating. This study relates to the second part. The participants were asked whether and how often they engage in the following activities: Talking in the phone, listening to the radio, watching TV, playing puzzles, checkers, card games, reading, playing drama, using laptops/tablets/iPads, participating in academic courses at the facility or at the university. Answers were coded on a 5-point scale [2] (5) every day; (1) once a month.
In order to examine the unique contribution of each activity, we grouped the activities into five main activities (table games, watching TV, and reading, using technological devices, participating in academic courses). Lifshitz et al. [1] found that not only the frequency, but also the cognitive loads of the activities influence the cognitive performance of adults with ID. In this study, it was decided to assess the cognitive load of the cognitively-stimulating activities more systematically. There are several methods for assessing cognitive load. Since our study focused on a population with ID, estimation of the mental load was determined according to expert opinion [34, 35]. Six judges ranked the cognitive load of the five main activities on a scale from 0.5 (very low) to 6 (extremely high). A taxonomy of cognitive load for each of the five tasks was constructed, and included the following components: basic cognitive concepts, Bloom's taxonomy adapted for populations with ID [36] comprehension of academic material through PowerPoint or oral presentation, reading and writing abilities, self-management skills, metacognitive skills, and performing a research. Between-judges reliability ranged between .9-1.00. Table 2 presents the cognitive load of the five cognitively-stimulating activities (Table 2).
Based on the task taxonomy, significant differences in the cognitive load of the academic courses were found between the experimental and control groups in reading and participating in academic courses.
Cognitive Test Battery
Two tests were used to assess the basic cognitive level (independent variable). Six tests were used to examine crystallized and fluid abilities (dependent variables).
Basic cognitive level was measured by two sub-tests of the MANN Abstract Verbal Thinking Test [32] which examines verbal abstract thinking or verbal intelligence abilities. Synonyms [32] examines verbal abstract thinking or verbal intelligence abilities (12 items), and is highly correlated with the Wechsler Verbal Intelligence tests. Participants are presented with a key word and are asked to find a similar word from a list of five other words. Correct answers received 1 point (range 0-12). Lifshitz et al. [1] used this test in a population with ID (test-retest reliability=0.90; α=0.91).
Phonemic fluency test: The number of words generated in one minute for the letters bet (/b/), gimel (/g/), and shin (/š/) was obtained. Instructions were as follows: “I want you to say as many Hebrew words as possible that begin with a certain letter”. The score is the sum of the words generated for all three letters (test-retest reliability=0.86; α=0.91). The crystallized battery was comprised of semantic fluency, verbal analogies and HMGT [37]. These tests are composed of declarative verbal acquired knowledge and are based on previous learning and acculturation [38]. A pretest among 10 participants conducted for all the tests
Semantic fluency test: The number of words generated in one minute for each of the following three semantic categories: animals, fruits and vegetables, and vehicles were obtained. The score is the sum of the words generated for all three categories (test-retest reliability=0.86). Verbal analogies (12 items) examine the understanding of verbal analogies. The subject is presented with a pair of related words and is asked to construct a similar relation between two other words. A correct answer afforded one point. The scores ranged from 0-12 (test-retest reliability=0.80). found them suitable for individuals with ID.
Homophone Meaning Generation Test–HMGT [37] examines the ability to shift between the different meanings of a homophone (10 items in Hebrew). Participants were instructed to say all meanings of the homophone, e.g. "He wrote a letter". A correct answer afforded one point (range 1-10) (test-retest reliability=0.83).
The fluid battery included three tests: The Raven Matrices Test (SPM) and the Trail Making Test (TMT) A and B, which require the ability to deal with novelty. These are culturally-unbiased nonverbal tests [28].
The Standard Progressive Matrices SPM [39] assesses the ability to form comparisons, deduce relationships, correlates, and reason by analogy. It refers to fluid intelligence and is considered a measure of general intelligence g. Participants solved sets AB, B (RCM) C, D and E. A correct answer afforded one point. Scores were the sum of the raw scores.
Trail Making Test [40] examines executive function processes. Part A measures visual scanning and tracking, motor speed and focused attention. Participants are asked to connect between consecutive digits printed in scattered patterns on a page. Part B measures cognitive flexibility, set shifting and divided attention, and requires connecting between sequences of letters and digits (e.g., 1-A-2-B and so on). The total score is the time in seconds needed to complete the two tests.
Procedure
Consent for participation was obtained from the participants’ parents/guardians. Authorizations were obtained from the University Ethics Committee and the Division of Individuals with ID in the Ministry of Social Affairs and Social Services. The study's aim and procedure were explained to all participants, who signed an adapted informed consent form for participation in scientific research. The participants chose payment or a gift for participating in the study.
The synonyms, phonemic fluency and the Cognitive/Leisure Activity Questionnaire were administered individually to each participant by the second author in a small room in the vocational and residential facilities (this stage lasted about two hours). Several days later, the Verbal Analogies and TMT A, B [40] were administrated along with the HMGT [37]. After a 30-minute break, the Raven SPM [39] was administered (this stage also lasted about two hours).
Findings
A one-way MANOVA was conducted for the six dependent variables in order to examine whether differences would be found in the crystallized and fluid battery performance between participants in the experimental and the control groups. There was a significant differences between the two groups, F (6,43)=8.37, p<0.001, ηp2=0.54. Means and SD of the two groups are presented in Table 3. Performance on the Raven, semantic fluency and HMGT tests was significantly higher among participants in the experimental group than among the control group. No significant differences were found for the verbal analogy and the TMT tests (Table 2)
| |
Experimental group
(N=21) |
Control group
(N=29) |
|
| Dependent variable |
M |
SD |
Range |
M |
SD |
Range |
F |
p |
ηp2 |
| Semantic fluency |
31.71 |
8.65 |
17-45 |
25.38 |
8.38 |
12-44 |
6.77* |
0.01 |
0.12 |
| Phonemic fluency |
13.76 |
7.86 |
2-29 |
11.55 |
6.09 |
3-27 |
1.26 |
0.27 |
0.03 |
| HMGT |
12.48 |
3.52 |
6-19 |
10.45 |
2.03 |
7-16 |
6.63* |
0.01 |
0.12 |
| Raven |
22.29 |
6.51 |
15-39 |
13.17 |
2.93 |
10-20 |
44.61*** |
0.00 |
0.48 |
| TMT–A |
43.00 |
31.01 |
23-165 |
56.97 |
32.82 |
25-150 |
2.25 |
0.14 |
0.04 |
| TMT–B |
114.48 |
61.18 |
61.18-114.8 |
120.28 |
58.77 |
48-242 |
0.11 |
0.74 |
0.00 |
**p<0.01;***p<0.001
Table 3: Means (and SD) in the six tests, by group.
A one-way MANOVA for the six dependent variables indicated no significant differences between the groups, F (6,43)=0.74, p=0.62, ηp2=0.09. Comparison of the two etiology groups in each of the dependent variables separately did not demonstrate a significant difference in performances in all six tests (p=0.08-0.97).
We divided the sample into two groups according to the median CA (Mdn=35; 25-35, 35 and above). One-way MANOVA for the six dependent variables indicated no significant differences between the two CA groups, F (6,43)=0.85, p=0.54,ηp2=0.11. When comparing the two CA groups in each of the dependent variables separately, the performances in all six tests were not significantly different (p =0.10-0.98).
Contribution of CA, Etiology and Cognitive Activities to Crystallize and Fluid Tests
A series of mixed regressions was performed for each of the crystallized and fluid tests in order to find the contribution of the five main cognitive activities to the EPV of the crystallized and fluid tests, beyond CA and etiology. In the first step, the two background characteristics (CA and etiology) were entered. In the second step, the five cognitive activities were entered in a stepwise manner. The results are presented in Tables 4 and 5.
| Dependent variable |
Steps |
Independent variable |
B |
SE.B |
β |
t |
R2 |
ΔR2 |
| Semantic fluency |
1 |
CA |
-0.01 |
0.16 |
-0.01 |
-0.09 |
- |
- |
| |
Etiology |
4.52 |
2.61 |
0.25 |
1.73 |
0.063 |
0.063 |
| |
2 |
CA |
-0.01 |
0.15 |
-0.01 |
-0.06 |
- |
- |
| - |
Etiology |
4.02 |
2.52 |
0.22 |
1.60 |
- |
- |
| - |
Cognitive activities |
0.42 |
0.19 |
0.30 |
2.18* |
0.154* |
0.091* |
| Verbal analogies |
1 |
CA |
0.01 |
0.04 |
0.04 |
0.27 |
- |
- |
| |
Etiology |
-0.15 |
0.68 |
-0.03 |
-0.23 |
0.002 |
0.002 |
| HMGT |
1 |
CA |
0.36 |
0.88 |
0.06 |
0.41 |
- |
- |
| |
|
Etiology |
0.36 |
0.88 |
0.06 |
0.41 |
0.006 |
0.006 |
| |
2 |
CA |
0.01 |
0.05 |
0.04 |
0.29 |
- |
- |
| |
- |
Etiology |
0.13 |
0.81 |
0.02 |
0.16 |
- |
- |
| |
- |
Cognitive activities |
0.19 |
0.06 |
0.42 |
3.04** |
0.179* |
0.173** |
| Raven |
1 |
CA |
-0.17 |
0.12 |
-0.22 |
-1.49 |
- |
- |
| |
|
Etiology |
0.13 |
1.93 |
0.01 |
0.07 |
0.047 |
0.047 |
| |
2 |
CA |
-0.17 |
0.11 |
-0.21 |
-1.56 |
- |
- |
| |
- |
Etiology |
-0.31 |
1.82 |
-0.02 |
-0.17 |
- |
- |
| |
- |
Cognitive activities |
0.37 |
0.14 |
0.36 |
2.66* |
0.180* |
0.132* |
| TMT–A |
1 |
CA |
0.26 |
0.59 |
0.07 |
0.45 |
- |
- |
| |
|
Etiology |
0.49 |
9.91 |
0.01 |
0.05 |
0.005 |
0.005 |
| |
2 |
CA |
0.25 |
0.56 |
0.06 |
0.44 |
- |
- |
| |
- |
Etiology |
2.57 |
9.47 |
0.04 |
0.27 |
- |
- |
| |
- |
Cognitive activities |
-1.73 |
0.73 |
-0.34 |
-2.39* |
0.119 |
0.114* |
| TMT–B |
1 |
CA |
-0.29 |
1.07 |
-0.04 |
-0.27 |
- |
- |
| |
- |
Etiology |
2.35 |
17.81 |
0.02 |
0.13 |
0.002 |
0.002 |
*p<0.05;**p<0.01
Table 4: Mixed regressions for the six tests by background characteristics (CA and etiology) and the cognitive load of cognitive/leisure activities.
| Dependent variable |
Steps |
Independent variable |
B |
SE.B |
β |
t |
R2 |
ΔR2 |
| Semantic fluency |
1 |
CA |
-0.07 |
0.15 |
-0.07 |
-0.50 |
- |
- |
| - |
Etiology |
4.61 |
2.54 |
0.26 |
1.82 |
0.06 |
0.06 |
| |
2 |
CA |
0.00 |
0.14 |
0.00 |
0.01 |
- |
- |
| - |
Etiology |
3.85 |
2.42 |
0.21 |
1.59 |
- |
- |
| - |
PSE |
0.89 |
0.35 |
0.35 |
2.55* |
0.18* |
0.12* |
| Verbal analogies |
1 |
CA |
-0.00 |
0.04 |
-0.01 |
-0.04 |
- |
- |
| - |
Etiology |
-0.06 |
0.66 |
-0.01 |
-0.08 |
0.00 |
0.00 |
| HMGT |
1 |
CA |
-0.00 |
0.05 |
0.00 |
-0.00 |
- |
- |
| |
- |
Etiology |
0.44 |
0.85 |
0.08 |
0.52 |
0.01 |
0.01 |
| 2 |
CA |
0.03 |
0.05 |
0.08 |
0.61 |
- |
- |
| - |
Etiology |
0.15 |
0.79 |
0.02 |
0.19 |
- |
- |
| - |
PSE |
0.34 |
0.11 |
0.41 |
2.99** |
0.17* |
0.16** |
| Raven |
1 |
CA |
-0.19 |
0.11 |
-0.24 |
-1.72 |
- |
- |
| |
- |
Etiology |
0.43 |
1.86 |
0.03 |
0.23 |
0.06 |
0.06 |
| 2 |
CA |
-0.08 |
0.08 |
-0.10 |
-0.97 |
- |
- |
| - |
Etiology |
-0.70 |
1.33 |
-0.05 |
-0.52 |
- |
- |
| - |
PSE |
1.30 |
0.19 |
0.71 |
6.82*** |
0.53*** |
0.47*** |
| TMT–A |
1 |
CA |
0.38 |
0.56 |
0.10 |
0.69 |
- |
- |
| |
- |
Etiology |
-1.46 |
9.58 |
-0.02 |
-0.15 |
0.01 |
0.01 |
| 2 |
CA |
0.34 |
0.50 |
0.09 |
0.67 |
- |
- |
| - |
Etiology |
-1.85 |
8.68 |
-0.03 |
-0.21 |
- |
- |
| - |
Reading |
-9.76 |
2.92 |
-0.44 |
-3.35** |
0.20* |
0.19** |
| 3 |
CA |
0.02 |
0.51 |
0.00 |
0.03 |
- |
- |
| - |
Etiology |
1.92 |
8.53 |
0.03 |
0.22 |
- |
- |
| - |
Reading |
-10.91 |
2.86 |
-0.49 |
-3.82*** |
- |
- |
| |
T. Games |
11.17 |
5.16 |
0.29 |
2.17* |
0.28** |
0.08* |
| TMT–B |
1 |
CA |
-0.07 |
1.01 |
-0.01 |
-0.07 |
- |
- |
| |
Etiology |
-2.26 |
17.33 |
-0.02 |
-0.13 |
0.00 |
0.00 |
*p<0.05;**p<0.01
Table 5: Mixed regressions for the crystallized and fluid tests by background characteristics (CA and etiology) and participation in PSE.
None of the background characteristics contributed significantly to the EPV of the crystallized and fluid tests. However, participation in PSE courses added significantly to two crystallized tests: 11.6% to the EPV of semantic fluency (F (3,46)=3.44, p<0.05), 16.2% to the EPV of HMGT (F (3,46)=3.09, p<0.05). As for the fluid tests, participation in PSE added 47.3% to the EPV of the Raven (F (3,46)=17.44, p<0.001). The positive beta coefficients indicated that participation in the PSE leads to higher performance on the above tests. On the other hand, TMT–A was associated with reading, which added 19.4% to the EPV (F (3,46)=3.93, p<0.05) and table games which added 7.5% to the EPV (F(4,45)=4.36, p<0.01). The negative beta coefficient indicated that higher levels of reading lead to faster performance.
One could argue that there might be a reciprocal relationship between the performance of participants in the crystalized and fluid tests (including the Raven which is an intelligent test) and the participation in cognitive activities in which adults with ID engage. That is, the higher their performance in the cognitive tests of the participants, the more they participate in cognitive activities. This claim, was examined in the general population [41] might be also true for populations with ID. Path analysis with Structural Equation Modeling using AMOS software was conducted in order to examine the assumption of a reciprocal relation between the five cognitive activities and the cognitive tests. The research model (1) fit indexes demonstrated good fit to data (2?=19.1; p=0.11 df=13, p=0.11, CFI=0.90, TLI=0.81, GFI=0.91, RMSEA=0.09), and suggested that the five main activities predict performance on the crystallized (β=0.81**) and the fluid tests (β=0.72**). The model shows that the crystallized tests were composed of the semantic β=0.40** and the HMG β=0.60*. The fluid tests were composed of the Raven test, β=0.89** and TMT, β=-0.48** (the higher the score, the faster did participants solve the problem). It should be noted that REMSI should be 0.08 and the k measure=less. However, the REMSI is not acceptable only if it is above 0.1 [42]. In addition, the typical range for TLI lies between 0-1. TLI close to one like ours indicates a good fit.
The second model (2) was set in the same way as the first, albeit in the opposite direction. However, the opposite model was insufficient (χ2=29.49 df=25, p<0.01, CFI=0.69, GFI=0.87, TLI=0.50, RMSEA=0.16) and suggested that the five main activities were not Experimental group predicted by the crystallized tests. They were only predicted by the fluid test, β=0.57*, which is comprised of the Raven and the TMT, but with less power than in the first model (p<0.05). These findings clearly indicate that the five main cognitive activities contribute more to the dependent crystallized and fluid tests and not the opposite direction (Figures 1 and 2).
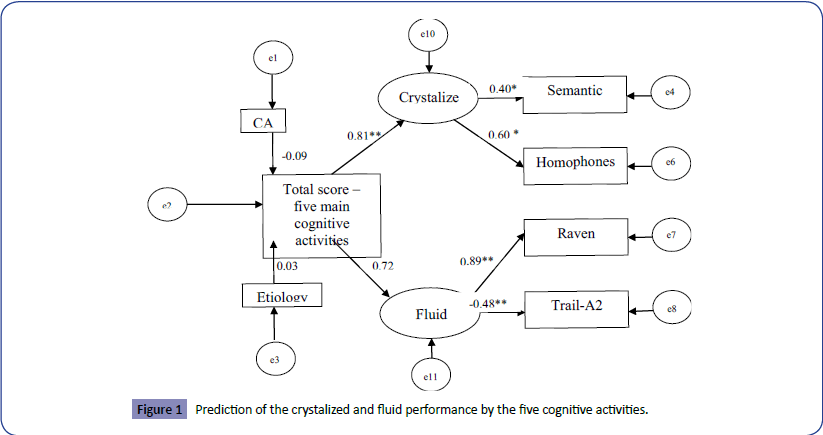
Figure 1: Prediction of the crystalized and fluid performance by the five cognitive activities.
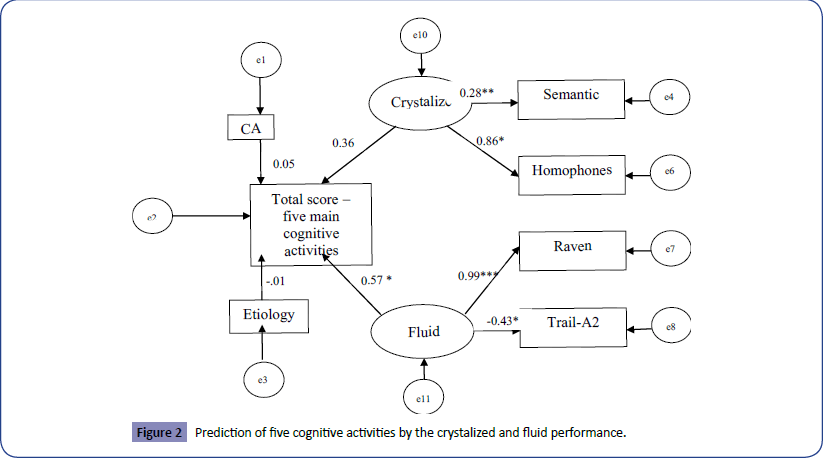
Figure 2: Prediction of five cognitive activities by the crystalized and fluid performance.
Discussion
Inclusion of persons with ID in PSE is increasing. Most studies focused on the social or vocational aspects [27]. To the best of our knowledge, this is the first study to address the cognitive outcomes of students with ID who participate in such programs. The CA of the PSE Empowerment Program at Bar-Ilan University ranges between 25-59. Thus, our vision of participation in PSE is two-fold: (a) In line with the Compensation Age Theory [10], the vision is to enable adults with ID to fulfill their cognitive potential; (b) In line with the Cognitive Activity Theory [19] participation of adults with ID in academic courses might impact their cognitive functioning in the short term, and might be a protective factor against accelerated decline in the future. Lishitz et al. [1] have recently reported that participation in cognitively-stimulating activities has an impact on crystallized and fluid tests performance. The present study examined the unique contribution of participation in the PSE academic courses on crystallized and fluid tests performance. Two issues will be at the core of the discussion: (a) The contribution of participation in PSE academic courses on crystallized and fluid tests; (b) The implications of our findings for adulthood and aging in populations with ID.
The impact of postsecondary academic courses on cognitive performance of adults with ID
The goal was to examine whether participation in PSE academic courses makes a unique contribution to the crystallized and fluid tests performance, beyond other cognitively-stimulating activities in which the participants engage during the week. The regressions indicated that participation in academic courses contributed significantly (50%) to semantic fluency, homophones and verbal analogies (crystallized battery) and to the Raven and Trail Making Test A (fluid battery).
In line with the Cognitive Activity Theory [19] and the CAT [10] the findings indicate that not only endogenous factors such as age and etiology, but also exogenous factor such as lifestyle determines the cognitive performance of adults with ID. Contrary to [2], and due to the special needs of the population with ID, the findings suggest that not only the frequency, but also the cognitive load of the activities contribute to their crystallized and fluid functioning. When relating to the contribution of each activity it was found that participation in academic courses contributed significantly to the EPV of the semantic fluency, homophones (crystallized test) and the Raven Test (fluid test-50%). However, Trail Making A (fluid test) was associated with reading and table games, which is self-explanatory. This finding indicates the role of participation in cognitively-stimulating activities in the life of adults with ID.
Scientists raised the question of whether academic knowledge is domain specific, i.e., the amount of its correlation with crystallized and fluid tests. In Ackerman [38], participants with a BA degree answered an academic knowledge test. It was found that science knowledge was mostly associated with fluid intelligence and less with crystallized intelligence. The opposite was found for social sciences. However, all knowledge tests were correlated with both intelligence measures. Ackerman postulated that there is a common variance in the academic knowledge which is correlated with both intelligence types. In line with Ackerman, our findings indicate that the academic enrichment acquired in the participants’ facilities, but mainly in the Empowerment Project at Bar-Ilan University, has an impact on both crystallized and fluid tests of adults with ID.
One could argue that there might be reciprocal relationships between the crystallized and fluid tests performance and the cognitive activities in which adults with ID engage. That is, the higher their crystallized and fluid scores, the more they participate in cognitive activities with greater cognitive load. This claim, which was not examined in the general population, might be true for populations with ID. Path analysis with Structural Equation Modeling indicated that the research model fit-indexes has a better fit to data and supports the claim that higher levels of five main cognitive activities contribute to higher performance in cognitive tests. The model fit-indexes for the opposite direction were insufficient. However, in this model, participation in the five cognitive activities was predicted only by the fluid tests, albeit with less power compared to the first model in which the five cognitive activities predict the crystallized and fluid tests performance. That is, participants with higher scores in the two fluid measures (Raven and Trail Making tests) were engaged in cognitive activities with greater cognitive load and mostly in the PSE. However, the power of prediction of the crystallized and fluid tests by the five cognitive activities was higher than the power of the opposite direction. This findings support also the application of the Cognitive Activity Theory in a population with ID.
Implications for adulthood and aging in populations with ID
Despite the broad age range of our participants (20-59), the findings did not reveal differences in any of the cognitive tests between the two age groups according to the median age nor between participants with NSID and those with DS. This finding was also supported in the regression and path analysis. Chronological age was not associated with any of the tests or with etiology. Our findings refute previous findings claiming a cognitive decline with increasing age among adults with ID, especially among adults with DS [14]. The findings empower the Compensation Age Theory [10], indicating stability of cognitive functioning among adults with ID with/without DS even at an advanced age, and support the Cognitive Activity Theory [19]. That is, frequent participation in cognitively-stimulating activities influences cognitive performance of adults with ID with and without DS.
Action should therefore be taken to introduce policy makers, administrators and care-giving personnel to the ideas of compensation and growth in adulthood of populations with ID. Cognitively-stimulating activities, especially participation in PSE programs, among adults with ID can be used not only as a mean for improving satisfaction and wellbeing and quality of life [20], but also as a mean for improving their cognitive functioning. Participation of adults with ID in PSE serves as a mean of fulfilling their cognitive potential. It may also have a long-term effect, and serve as a protective factor against their accelerated deterioration.
Limitations and Future Research
Generalization should be performed with caution, due to the small sample size. Future research, using a broader sample, would help validate the findings for populations with ID. The study supports the short-term implications of applying the Cognitive Activity Theory in the population with ID. A longitudinal study should be conducted in order to support the theory’s claim about reducing the risk of Alzheimer's disease with increasing age even among adults with ID. In this study, crystallized and fluid tests were limited to those that were used in the original study. Examining the effect of cognitively-stimulating activities on other intelligence tests, working and long-term memory, is recommended.
Our study is the first to address the applicability of the Cognitive Activity Theory among adults with ID. It is recommended to examine the application of this theory also for the autism spectrum disorder (ASD).
References
- VahavLH, Shnitzer S, Mashal N (2015) Participation in recreation and cognitive activitiesas a predictor of cognitive performance of adults with/without down syndrome. Aging and Mental Health.
- Wilson RS, Mendes De Leon CF, BarnesLL, Schneider JA, Bienias JL et al.(2002) Participation in cognitively stimulating activities and risk of incident alzheimer disease. JAMA 287: 742-748.
- Coppus AMW (2013) People with intellectual disability: what do we know about adulthood and life expectancy? Developmental Disability Research Review18: 6-16.
- Chicoine B, McGuire D (1997) Longevity in a woman with downsyndrome: a case study. Mental Retardation35: 477-479.
- Mahncke HW, Connor BB, Appelman J, Ahsanuddin ON, Hardy JL, et al. (2006) Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. States of America103: 12523-12528.
- Kim EY, Kim KW (2014) A theoretical framework for cognitive and non-cognitive interventions for older adults: Stimulation versus compensation. Aging and Mental Health18: 304-315.
- Lifshitz H, Rand Y (1999) Cognitive modifiability in adult and older people with mental retardation. Mental Retardation 37: 125-138.
- Lifshitz H, Tzuriel D (2004) Durability of effects of instrumental enrichment in adults with intellectual disabilities. Journal of Cognitive Education and Psychology3: 297-322.
- Lifshitz H, Weiss I, Tzuriel D, Tzemach M (2011) New model of mapping difficulties in solving analogical problems among adolescents and adults with intellectual disability. Research in Developmental Disabilities32: 326-344.
- VahavLH (2015) Compensation Age Theory (CAT): A monograph on the effect of chronological age in a population of intellectual disability. Education and Training in Autism and Developmental Disabilities50: 142-154.
- Feuerstein R (2003) Feuerstein's theory of cognitive modifiability and mediated learning. In:SengTO, ParsonsRD, Hinson SL, BrownDS (edn.) Educational psychology, a practitioner-researcher approach,Seng Lee Press, Singaporepp: 59-60
- Feuerstein R, Rand Y (1974) Mediated learning experience: an outline of proximal etiology for differential development of cognitive functions. International Understandingpp: 7-37.
- Stern Y, Habeck C, Moeller J, Scarmeas N, Anderson KE, et al. (2005) Brain networks associated with cognitive reserve in healthy young and old adults. Cerebral Cortex15: 394-402.
- Zigman WB, Schupf N, Devenny DA, Miezejeski C, Ryan R, et al. (2004) Incidence and prevalence of dementia in elderly adults with mental retardation without Down syndrome. American Association on Mental Retardation 109: 126-141.
- Snowdon DA, Greiner LH, Markesbery W (2000) Linguistic ability in early life and the neuropathology of Alzheimer’s disease and cerebrovascular disease: Findings from the Nun study. In Kalaria RN,Ince P (eds.)Vascular factors in Alzheimer’s disease: Annals NY Academy of Science, New York Academy of Sciences,New York903: 34-38.
- Devenny DA, Silverman WP, Hill AL, Jenkins E, Sersen EA, et al. (1996) Normal aging in adults with down's syndrome: a longitudinal study. Journal of Intellectual Disability Research 40: 208-221.
- Facon B (2008) A cross-sectional test of the similar-trajectory hypothesis among adults with mental retardation.Research in Developmental Disabilities 29:29-44.
- MarquineaMJ, Segawaa E, Wilson RS, Bennett D, Barnes LL (2012) Association between cognitive activity and cognitive function in older Hispanics. Journal of the International Neuropsychological Society 18: 1041-1051.
- Wilson RS, Barnes LL, Bennett DA (2007) Assessment of lifetime participation in cognitively stimulating activities. In Y. Stern(Ed.), Cognitive reserve, theory and practice,Taylor and Francis, New York pp: 100-115.
- Bergström H, Hochwälder J, Kottorp A, Elinder LS (2013) Psychometric evaluation of a scale to assess satisfaction with life among people with intellectual disabilities living in community residences. Journal Intellectual Disability Research 57: 250-256.
- Patterson I, Pegg S (2009) Serious leisure and people with intellectual disability: benefits and opportunities. Leisure Activities 28: 387-402.
- Duvdevany I, Arar E (2004) Leisure activity, friendship and quality of life of persons with intellectual disability: Foster homes vs. community residential setting. International Journal of Rehabilitation Research 27: 289-296.
- Faisal A, Croitoru T, Rimmerman A, Naon D (2011) Participation in leisure activities of jewish and arab adults with intellectual disabilities living in the community. International Journal of Social Welfare 20: 97-103.
- Plotner AJ, Marshall K J (2015) Postsecondary education programs for students with an intellectual disability: facilitators and barriers to implementation. Intellectual and Development Disabilities 53: 56-69.
- Uditsky B,Hugson E (2012) Inclusive postsecondary education-an evidence-based moral imperative. Journal of Policy and Practice in Intellectual Disabilities 9: 298-302.
- Sheppard-Jones K, Kleinert HL, Druckemiller W, Kovacevich Ray M (2015) Students with intellectual disability in higher education: adult service provider perspectives. Intellectual and Developmental Disabilities 53: 120-128.
- O’Connor B, Kubiak J, Espiner D, O’Brien P (2012) Lecturer responses to the inclusion of students with intellectual disabilities auditing undergraduate classes. Journal of Policy and Practice in Intellectual Disabilities 9: 247-225.
- McGrew K (2009) CHC theory and the human cognitive abilities project: standing on the shoulders of the giants of psychometric intelligence research. Intelligence 37: 1-10.
- Kaufman AS (2001) WAIS-III IQs, Horn’s theory, and generational changes from young adulthood to old age. Intelligence 29: 131-167.
- Kittler P,Krinsky-McHale SJ, Devenny DA (2004) Sex differences in performance over 7 years on the Wechsler Intelligence Scale for Children--Revised among adults with intellectual disability. Journal of Intellectual Disability Research48: 114-122.
- Shnitzer S, Lifshitz-Vahav H, Mashal N (submitted) Comprehension of visual and verbal metaphors among individuals with intellectual disability with and without Down syndrome.
- Glanz Y (1989) HachashivaKe’tifkudtlat-kivuni Thinking and three-directional functioning. Ramat Gan: Reches.
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5thedn.) Washington.
- Paas F, Van Merriënboer JJG, Adam JJ (1994) Measurement of cognitive load in instructional research. Perceptual and Motor Skills 79: 419-430.
- Xie B, Salvendy G (2000) Prediction of mental workload in single and multiple task environments. International Journal of Cognitive Ergonomics4: 213-242.
- LuftigRL (1987) Teaching the mentally retarded student, curriculum methods and strategies. Massachusetts: Allyn Bacon.
- Mashal N, Kasirer A (2011) Thinking maps enhance metaphoric competence in children with autism and learning disabilities. Research in Developmental Disabilities 32: 2045-2054.
- Ackerman FL (2000) Domain-specific knowledge as the “Dark Matter” of adult intelligence: Gf/Gc, personality and interest correlates. Journal of Gerontology 55B: 69-84.
- Raven JC, Court JH, Raven J (1986) Manual for raven's progressive matrices and vocabulary Scales. Oxford: Oxford Psychologists Press.
- Lifshitz-Vahav H, Shrira A, Bodner E (2016) Thereciprocal relationship between participation in leisure activities and cognitive functioning: the moderating effect of literacy. Aging and Mental Health 8: 1-8.
- Reitan RM, Davison LA (1974) Clinical neuropsychology: Current status and applications. Wiley, New York.
- Brown W, Cudex A (1993) Alternative way of assessing model fit. In Bollen KA&Elong JS (Eds)Testing structure equation models, Newbury Park, CA: Sagepp: 136-162.

