Keywords
Carcinoma, Islet Cell; Neuroendocrine Tumors
Abbreviations
NEC neuroendocrine carcinoma; NET neuroendocrine
tumor; panNEC pancreatic neuroendocrine carcinoma
INTRODUCTION
According to the World Health Organization (WHO)
2010 classification of tumors of the digestive system,
pancreatic neuroendocrine neoplasm (panNEN) is
classified into NET-G1, NET-G2, or neuroendocrine
carcinoma (NEC) based on its proliferative activity
evaluated by mitotic counts or Ki67 labeling index (LI)
[1]. However, the category of pancreatic NEC (panNEC;
equivalent to NEN-G3) has been shown by multiple studies
to include two clinically and genetically different types
of tumors, and the WHO 2017 classification of tumors of
endocrine organs divided panNEC into neuroendocrine
tumor (NET)-G3 and neuroendocrine carcinoma (NEC)-G3.
Although a number of studies have investigated the
characteristics of the NET-G3 and NEC-G3 subgroups in
terms of imaging, genetics, and treatment regimens, many
points still remain unclear.
In this review, we refer to WHO2010-NEC as NEN-G3
and divide this into NET-G3 and NEC-G3 that will be incorporated into to the WHO 2017 classification. We
review the clinical and genetic characteristics of pancreatic
NEN-G3 and discuss appropriate medical therapies.
DIAGNOSIS AND CLINICOPATHOLOGICAL FEATURES
OF NEN-G3
Problems with the WHO 2010 Classification
Ki67 is a powerful prognostic marker for panNEN [1]
and a major revision was therefore made from the 2000
WHO classification system to the WHO 2010 terminology
system, in which mitotic count and/or Ki67 LI were adopted
as pivotal indicators of stratification [1]. The revised WHO
classification 2010 [2] has since become the standard and
has been widely applied. In this WHO classification, NENs
with Ki67 LI >20% or mitotic index >20/10 high-power
fields were categorized as neuroendocrine carcinoma
(NEC).
However, in 2013, the first clinical report was made
by a Nordic group indicating that gastroentero-pancreatic
(GEP) NECs according to the 2010 WHO classification is
clinically a heterogeneous category based on 305 patient
records from hospital charts from 12 Nordic hospitals [3].
In their study, the group with Ki67 LI <55% showed lower
response rate to platinum-based chemotherapy (15% vs.
42%; P<0.01), and longer overall survival (MST, 14 months
vs. 10 months; P<0.01) compared with the Ki67LI ≥55%
group. Although no detailed histological subclassification
was performed in that study, it became the first paper
to question the uniform application of platinum-based chemotherapy for NEC (WHO2010-NEC). Subsequent to
that report, National Comprehensive Cancer Network
(NCCN) guidelines provided a general recommendation in
footnotes that NECs, with high Ki67 LI (>50%), be treated
with small cell lung cancer regimens, such as cisplatin/
etoposide or carboplatin/etoposide. However, evolving
data suggest that tumors with intermediate Ki67 levels in
the range of 20-50% may not respond as well to platinum/
etoposide as those with small cell histology or extremely
high Ki67, and clinical judgment should thus be used [4].
The French group of Velayoudom et al. [5] subsequently
examined 28 cases of WHO2010-NEC including
gastroenteropancreatic (GEP), lung and pharyngeal/
laryngeal tumors in 2014. They showed that NEC that was
morphologically well differentiated and resembled NET
G2, but with Ki67 LI >20%, could be termed as “G3-welldifferentiated
NET (G3-WDNET; equivalent to the current
NET-G3).” They reported that response to platinum-based
chemotherapies and the prognosis of G3-WDNET differed
greatly from G3 poorly differentiated NEC (G3-PDNEC;
equivalent to current NEC-G3). After that report, the
presence of NET-G3 attracted substantial attention, with
some articles reported over the course of 4 years [5, 6, 7, 8, 9, 10, 11, 12, 13]. The frequency of panNET-G3 among
panNEN-G3 was 30-49%, and the frequency of GEPNET-
G3 among GEP-NEN-G3 was 18-42%. Although the
selection bias due to study design should be considered,
panNETs-G3 may not be rare in NENs-G3.
Clinical Differences between NET-G3 and NEC-G3
Differences
panNEC-G3 progresses rapidly, with frequent early
metastasis to other organs. Although there have been a
few reports of surgical resection as attempted curative
therapy, in most cases the cancer has recurred and
the prognosis is extremely poor. These clinical and
pathological characteristics, as well as its sensitivity to
chemotherapy, possess similarities to those of SCLC and
NSNLC. The symptoms of panNEC-G3 are dependent on
the presence of metastasis, and include not only local
symptoms such as pain and jaundice but also cachexic
symptoms similar to those seen in pancreatic carcinoma,
including loss of appetite, malaise, and weight loss.
NEC is non-functioning in almost all cases, and rarely
exhibits hormonal symptoms [14]. NEC-G3 is also almost
never found in combination with the MEN type 1 or VHL
hereditary neoplastic syndromes. In contrast, cachexia
is seldom evident in patients with panNET-G3 and it
may be functioning; it may also stem from a hereditary
neoplastic syndrome. panNEC-G3 also has a higher rate
of metastasis than panNET, and one study found that
distant metastasis was already present at diagnosis in
46.3% of cases [14]. The liver is the most common site of
metastasis, and other metastatic sites include the lymph
nodes, bone, lungs, skin, and brain [15]. A report from
the Surveillance, Epidemiology, and End Results (SEER)
database found that the median overall survival of 2546
patients with poorly differentiated gastroenteropancreatic neuroendocrine carcinoma (GEPNEC-G3) was 14 months
(95% CI: 13–15 months] for patients with advanced local
disease (including lymph node metastasis and invasion
of the surrounding tissue) and 5 months (95% CI: 4.5–
5.5 months) for those with distant metastasis. Overall
survival for panNEC-G3 is conventionally considered to
be 8.5–21 months [7, 16, 17, 18]. Some studies have found
no difference in survival between SCNEC and LCNEC
[19], but others have found that the duration is shorter
for LCNEC [8], and no consensus has yet been reached.
Overall survival for panNET-G3 is 41–52 months [5, 7, 8, 11]. Considering limitations including sample size and
potential selection bias, further studies on the prognostic
difference would be needed.
Imaging Differences between NET-G3 and NEC-G3
Imaging findings for panNEC-G3 have little in common
with those for panNET. On CT and EUS, panNET typically
appears as a clearly demarcated, internally homogeneous,
hypervascular tumor, whereas one study found that in 80%
of cases panNEC-G3 exhibited a hypovascular pattern on
contrast-enhanced CT, with stenosis of the main pancreatic
duct visible in 65% of cases, and 81.8% of cases were
preoperatively diagnoses as pancreatic carcinoma [9]. On
MRI, compared with panNET, panNEC-G3 was hyperintense
on diffusion-weighted imaging (DWI) and apparent
diffusion coefficient (ADC) values were significantly lower
than either healthy pancreatic parenchyma or panNET, a
finding that is useful for differentiating between the two
[20].
panNET has a low uptake rate of 29% on FDG-PET [21],
whereas NEC-G3 has an FDG-PET positive rate of over
80% [22], a difference that is useful for the local diagnosis
and staging of tumors. A positive FDG-PET reflects
tumor grade, and tends to indicate shorter progressionfree
survival and overall survival from the start of
chemotherapy [23, 24]. Somatostatin receptor scintigraphy
(SRS) reveals expression in 67%–92% of NET-G3 tumors
compared with only 40%–50% of NEC-G3 tumors [5, 7, 11, 13]. A relatively new PET/CT technique, using
somatostatin analogs labeled with the positron emitting
isotope, 68Ga (68Ga-DOTA peptides), has been shown to
offer advantages over conventional imaging modalities
as well as additional important quantitative and
qualitative diagnostic information [25, 26]. However, for
both FDG-PET and SRS/68Ga-DOTA peptides, whether or
not uptake will be present is unknown before imaging is
performed. A recent study has reported that scoring on
the basis of the performance of both imaging modalities
(NETPET grade) is associated with prognosis [27].
Ki67 Differences between NET-G3 and NEC-G3
In 1996, La Rosa et al. showed that patients with NET
expressing the MIB-1 epitope of Ki67 in >2% of cells
displayed poorer prognosis compared with NET patients
with MIB-1/ Ki67% <2% [28]. This finding was confirmed
in other studies [29]. A 20% threshold was established
during the Frascati consensus to define NEC [30, 31], and this ratio was validated during the validation clinical
studies [32, 33].
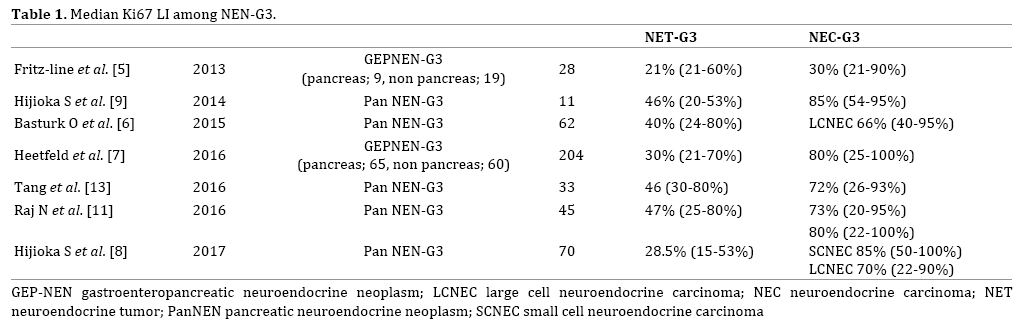
Is it possible to distinguish NET-G3 from NEC based
on the Ki67 LI alone? Table 1 shows the median Ki67 LI
among NEN-G3 reported in each article. Seven articles (four
on panNEN-G3, three on GEPNEC-G3) mentioned Ki67 for
NET-G3 and NEC-G3 [5, 6, 7, 8, 9, 11, 13]. Median Ki67 for
NET-G3 was 21-47%, and median Ki67 for NEC-G3 was 30-
85%. From these results, setting a cut-off of Ki67 LI to 55%
for dividing NET-G3 and NEC-G3 appears suitable [10], but
still there is an overlap between the two and it would be
difficult to separate NEC and NET-G3 based on the Ki67 LI
alone, particularly tumors whose LI range between 20%
and 50%. In addition, as Fazio et al. [34] mentioned, setting
a clear-cut cut-off value of Ki67 LI seems difficult because
of the various factors that affect the evaluation of Ki67,
including formalin fixation time, measuring method on
Ki67 LI [35, 36], and the existence of heterogeneity within
tumors [37].
A recent study has investigated changes in Ki67
at reassessment at the time of disease progression.
According to this, 16.7% of panNETs transformed from
NET-G2 to NET-G3, and the results suggested that tumors
may transform from NET-G2 to NET-G3 with disease
progression [38].
Genetic and Immunohistological Alterations of
NET-G1/2 and NEC
Thanks to recent advances in the sequencing
technologies and computational analyses of large-scale
genomic data, key differences in genetic characteristics
between NEC-G3 and well-differentiated NET G1/G2
have gradually been revealed. Although our knowledge
on the molecular features of NET-G3 is limited because
of the recent recognition and rare occurrence, studies
consistently suggest that NET-G3 has similar molecular
features of NET G1/G2 rather than those of NEC-G3.
Whole-exome sequencing of well-differentiated
panNENs was first performed by Jiao et al. in 2011 [39].
First, somatic inactivating mutations in MEN1 were
detected in 44% of cases. Second, somatic inactivating
mutations in ATRX (thalassemia/mental retardation
syndrome X-linked) and DAXX (death-domain-associated protein) were detected in 43% (18% and 25% of cases,
respectively) [39]. Subsequent studies revealed a strong
correlation between the inactivation of ATRX or DAXX and the telomerase-independent telomere maintenance
mechanism termed “alternative lengthening of telomeres”
(ALT) and chromosomal instability [39, 40, 41]. Third,
somatic mutations in genes associated with the mTOR
pathway were detected in 18% of patients [39]. Specifically,
the prevalence of mutations was 7% for PTEN, 9% for TSC2 and 1% for PIK3CA. These findings were confirmed
by other whole-exome and whole-genome sequencing
studies [42]. Scarpa et al. reported the results of wholegenome
sequencing for 102 panNETs [42]. Based on that
report, clinically sporadic panNETs appear to contain a
larger-than-expected proportion of germline mutations,
including previously unreported mutations in the DNA
repair genes MUTYH, CHEK2 and BRCA2. Together with
mutations in MEN1 and VHL, these mutations are present
in 17% of patients. Somatic mutations were commonly
found in genes involved in four main pathways: chromatin
remodeling; DNA damage repair; activation of mTOR
signaling (including previously undescribed EWSR1 gene
fusions); and telomere maintenance.
In addition to these key alterations, other recurrent
mutations of NET-G1/G2 have also been reported,
including YY1 (in insulinomas), SETD2, etc. [43].
In contrast, NEC appears to have distinct genetic and
immunohistological features from NET-G1/G2 [44, 45].
Yachida et al. [45] performed immunohistochemical
and mutational analyses for 19 poorly differentiated
panNEC cases, and found abnormal immunolabeling of
the p53 protein and Rb protein in 95% and 74% of cases,
respectively. They also noted overexpressed Bcl-2 protein
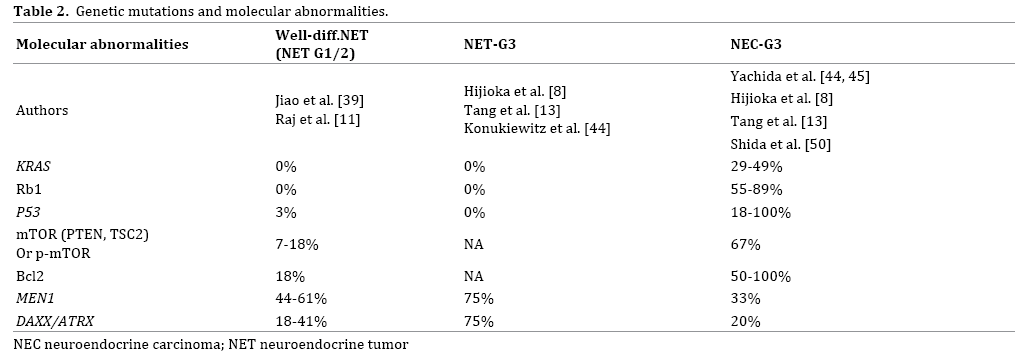
in 74% of cases. Other studies followed, consistently
showing the recurrent mutations of TP53, Rb1 and KRAS in NECs, which were rarely found in NET-G1/G2 (Table
2). Taken together, NET-G1/G2 is characterized by
frequent mutations of MEN1, DAXX, and ATRX, while NEC
by mutations of TP53, Rb1, and KRAS. This feature gives
reasonable grounds for the categorization of NET-G3
discussed below. NEC and pancreatic carcinoma possess
genetic similarities, with NEC exhibiting the same “big
four” genetic mutations (TP53, KRAS, CDKN2A, and SMAD4)
seen in normal-type pancreatic carcinoma. However, the frequency of KRAS mutations, which are present in
almost all cases of pancreatic carcinoma, is comparatively
low in NEC, suggesting that pancreatic carcinoma and
panNEC-G3 may have different genetic backgrounds.
Tang et al. have proposed a diagnostic algorithm for
panNEC-G3 that incorporates genetic data in addition to
conventional morphological diagnosis [46]. Tumors with the
morphological characteristics of NET that have lost DAXX and ATRX expression are classified as NET-G3, and those with Rb1 deletion or abnormal TP53 expression as NEC-G3. This
may improve diagnostic accuracy in cases where diagnosis is
difficult on the basis of morphology alone.
Data on genetic mutations may thus both improve
diagnostic yield and provide predictive factors for
response to treatment and prognosis. From the viewpoint
of treatment strategy, too, accurate specimen collection
and pathological diagnosis on the basis of EUS-FNA and
resected samples will also become more important when
starting chemotherapy for panNEC-G3.
Genetic and Immunohistochemical Abnormalities in
NET-G3 (Table 2)
There are a few studies to date that focused on the
genetic and immunohistochemical abnormalities in
NET-G3. Tang et al. [13] performed targeted sequencing
of RB1, DAXX, ATRX and MEN1 in 4 pancreatic welldifferentiated
NETs with high-grade component and found DAXX/ATRX/MEN1 mutations in three of four pancreatic
WDNETs in the high-grade component (NET-G3) as well
as its lower-grade counterpart. RB1 gene mutations,
along with loss of Rb protein expression or abnormal p53
expression on immunohistochemistry, were not detected
in WDNETs of any grade within the tumors.
Hijioka and Hosoda et al. [8] examined 70 patients,
analyzing 21 NETs-G3 (30%) and 49 NECs-G3 (70%).
NET-G3 showed no abnormal Rb expression (0%), and
no mutations in KRAS (0%), whereas NEC-G3 showed
frequent Rb loss (54.5%) and KRAS mutations (48.7%).
Konukiewitz et al. analyzed TP53 mutation and
immunohistochemistry of 9 cases of WDNET-G3, and found abnormal expression of DAXX or ATRX in 4/9 cases. The
TP53 gene and immunolabeling of Rb1 and p53 proteins
were intact in all cases [44].
NEC-G3 presents TP53 mutation found in 18-100%
and KRAS mutation in 29-49% [45, 47], whereas NET-G3
does not show such mutation [8, 9, 13, 39]. Taken together,
these molecular studies consistently support the view that
NET-G3 is closely related to NET-G1/G2 rather than NEC.
Moreover, these molecular features may serve as adjunct
markers of distinction of NET-G3 from PDNEC, particularly
large-cell NEC, when histological distinction between them
was challenging [8, 12, 13, 44].
Response of NET-G3 to Platinum-Based Chemotherapy
(Table 3)
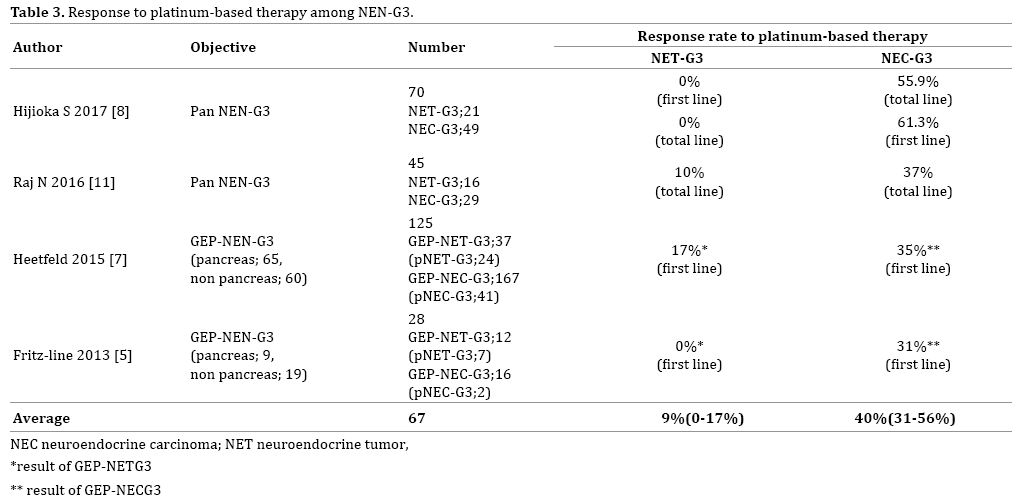
Vélayoudom-Céphise et al. [5] investigated 20 patients
with gastroenteropancreatic and thoracic NEC who had
been treated with platinum-based chemotherapies. No
cases of NET-G3 exhibited response to platinum-based
chemotherapy (0%), whereas 31% (5 of 16) large cell
NECs showed response. Heetfeld et al. [7] reported 12
patients with gastroenteropancreatic (GEP) NET-G3
and 113 patients with GEP-NEC treated using platinumbased
chemotherapy and revealed that the response rate
was lower for GEP NET-G3 (17%) than for GEP NEC-G3
(35%; P=0.18). Nitya et al. [48] reported that one of
10 panNET-G3 patients (10%) responded to platinumbased
chemotherapies, whereas 10 panNET-G3 patients
(37%) responded to platinum-based chemotherapies. In
a Japanese panNEN-G3 study, response to platinum-based
chemotherapy for NET-G3 was extremely poor, with a
RR of 0%. In comparison, the RR for NEC-G3 was good, at
55.9% (P<0.001).
Taken together, the distinction between NET-G3 and
NEC-G3 is extremely important in determining treatment
options for patients with panNEN-G3, and platinum-based
chemotherapy should not be used as the first-line therapy
for NET-G3.
In addition, when stratifying PanNEN-G3 according
to Rb and KRAS status, panNEN-G3 with Rb loss or with mutated KRAS showed significantly higher RR to platinumbased
chemotherapy than those without (Rb loss, 80% vs. normal Rb, 24%, p=0.006; mutated KRAS, 77% vs.
wild-type, 23%, p=0.023). Rb was a predictive marker of
response to platinum-based chemotherapy even in NEC-G3
(P=0.035). As a result, Rb and KRAS offer promising
predictors of response to platinum-based chemotherapy
for PanNEN-G3, and Rb also predicts response for NEC-G3.
CHEMOTHERAPY FOR NEN-G3
Chemotherapy for NET-G3
As mentioned above, cases of NET-G3 show poor
response to platinum-based chemotherapy. So, what is a
useful regimen for NET-G3?
Among panNET patients, the PI3-K/AKT/mTOR
pathway is reportedly activated, and expressions of
TSC2 or PTEN inhibiting activity of the mTOR pathway
are decreased in most cases of panNET. These patients
reportedly show a shortened progression-free survival
period [46].
However, as in well-differentiated NET, mutation to the
PI3K/AKT/mTOR pathway has been found in small-cell
lung cancer [49]. Furthermore, overexpression of mTOR
has been reported in 67-80% of pancreas NEC [50, 51].
From these findings, some degree of efficacy is anticipated
for everolimus, an mTOR inhibitor for panNEC-G3. Actually,
some reports have noted that everolimus was effective for
NET-G3 and high-grade NEC [52, 53], and NECTOR studies
[54] are ongoing in Japan. Also, in more recent years, the
RR to alkylating agent among 45 pancreas NET-G3 was
50% [48]. The 2016 European Neuroendocrine Tumor
Society (ENETS) guidelines recommend alkylating
agent-based combination therapy e.g. STZ+ 5-FU or
temozolomide (TMZ)+capecitabine(CAP) for panNET-G3
[55]. Recently, multicenter study evaluated the response of STZ based, platinum-based and dacarbazine/TMZbased
chemotherapy regimens as first-line treatment in
74 patients with pNETs and KI-67 LI > 10% (31% included
NET-G3) [56]. There was no difference in the PFS between
the three regimens; shorter NET-G3 cases (HR 2.15, 95%
CI: 1.18-3.92, p=0.012) and age above 55 years (HR 1.84,
95% CI: 1.06-3.18, p=0.030) were associated with shorter
median PFS.
Multiple clinical trials are ongoing for GEP-NETG3.
The ECOG-ACRIN Cancer Research Group is performing
a randomized, controlled phase II study of etoposide
+cisplatin vs. temozolomide+capecitabine for non-small
cell carcinoma and GEPNET-G3. The registration was
started with the goal of 126 cases from 2015. TEM+CAP
can be expected to achieve high response from NET-G3.
Haukeland University Hospital is performing a phase II
study of everolimus+TEM for GEPNET-G3 (Ki67, 20-55%)
in 40 patients from 2014 (primary endpoint, DCR).
Preliminary evidence of immune dysregulation in
the NET microenvironment has been recently provided.
Expression of programmed death-ligand 1 (PD-L1) and
programmed death-ligand 2 (PD-L2) by tumor cells [57, 58, 59] may drive immune evasion in GEP-NETs, and immune
checkpoint inhibitors are currently under intensive
clinical investigation (NCT02955069, NCT02939651,
NCT02923934).
Because NET-G3 is a new disease classification, little
evidence is available for treatment regimens in particular,
and this is an important topic for future studies.
Chemotherapy for NEC-G3
Regarding drug therapy for NET G1 and G2, therapeutic
drugs differ for the pancreas and gastrointestinal tract, but
the treatment strategy for NEC-G3 is basically the same as
for the pancreatic/gastrointestinal tract.
As noted earlier, poorly differentiated NEC (small
cell carcinoma or large cell carcinoma) occurs in organs
such as the lung, pancreas and gastrointestinal tract, but
regardless of the organ, the biological malignancy and
genetic background are similar. The loss of RB protein
expression seen in lung small cell carcinoma has been
reported even in pancreatic NEC [16, 25].
For these reasons, and likewise for extrapulmonary
NEC, various guidelines recommend administering the
same platinum-based regimens used for chemotherapy for
small cell lung cancer (European Neuroendocrine Tumor
Society [55], NCCN Clinical Practice 2017 version 3 [4]).
The current standard chemotherapy for small cell lung
cancer is cisplatin+etoposide combination therapy (EP
therapy) or cisplatin+irinotecan combination therapy (IP
therapy). EP therapy has mainly been used in the United
States and Europe. ENETS guidelines recommend EP
therapy for NEC, regardless of the organ [55]. However,
cytotoxic drug treatment for small cell lung cancer has
shown little improvement in therapeutic results over
many years.
So, what are the treatment results of platinum regimens
for panNEC? To date, no results have been obtained from
prospective clinical trials, and studies have mainly been
retrospective. The Nordic NEC study [3] in Northern
Europe and the multicenter GEP-NEC retrospective study
by Yamaguchi et al. [16] are instructive. In the Nordic
NEC study [3], the most frequently used methods were EP
therapy at 51%, followed by etoposide+CBDCA therapy at
27%, showing the frequent use of etoposide. Meanwhile,
the Japan GEP-NEC study was characterized by the fact
that IP therapy was overwhelmingly used, at a rate of
62%, followed by EP therapy at 18%. Response rates to IP
therapy and EP therapy in the treatment of hepatobiliarypancreatic
NEC were reported as 39% (7/18) and 12%
(4/34), respectively. The reason why RR with platinum
chemotherapies were low is considered that not only
NEC-G3, NET-G3 cases were also included in this report.
Gene mutations in the PI3-K/AKT/mTOR pathway
were found not only in well-differentiated NET but
overexpression of mTOR was reported in 67% (6/9)
to 80% (29/36) of panNEC patients [50]. Based on this
background, everolimus, an mTOR inhibitor, is expected to
prove effective even for NEC-G3.
Emerging Issues Regarding NEC-G3
In the Japan PanNEN-G3 study, KRAS gene mutation
and loss of Rb protein expression were each found in about
half of NEC-G3 patients: 48.7% and 54.5% [8]. Moreover,
the first-line response rate to platinum-based regimens for
NEC-G3 was 61.3%. Conversely, about 40% of panNEC-G3
does not respond to platinum-based regimens. Based
on these results, predictive factors of platinum-based
regimens for the response to NEC-G3 is important.
When we excluded NET G3 and analyzed 49 patients
diagnosed with NEC-G3, only retained Rb immunolabeling
group showed significantly worse response for platinumbased
chemotherapy compared with loss of Rb (P=0.031).
Loss of Rb immunolabeling was only a predictor of
platinum-based chemotherapy response even in NEC-G3
(OR=7.7; 95% CI, 1.16–51.1; P=0.035). Indeed, response
to platinum-based regimens for NEC-G3 without retained
Rb immunolabeling group (abnormal Rb group) was
80% (12 of 15), whereas response to platinum-based
regimens for NEC-G3 with retained Rb immunolabeling
group (normal Rb group) was significantly lower (38.4%;
5 of 13) than abnormal Rb group (P=0.031). From genetic
and morphological perspectives—as shown in Table 4.
NEC-G3 may be divided into two groups, with NEN-G3 as a
whole divided into 3 groups.
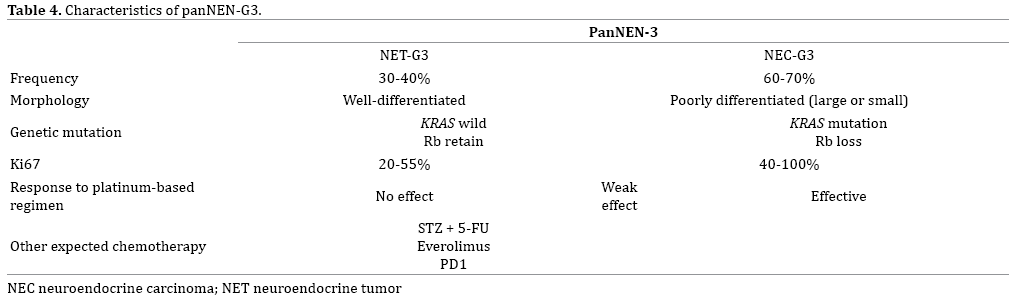
As for NET-G3, the NEC-G3 group without Rb abnormality
is less likely to respond to platinum chemotherapy.
Accordingly, future studies need to elucidate whether the
same treatment as for NET-G3 should be used, or whether
new treatment options are required.
Financial Support
This research was supported by the Practical Research
for Innovative Cancer Control from Japan Agency for
Medical Research and development, AMED.
Conflict of Interest
S. Hijioka has received honoraria from Pfizer, Novartis,
Fuji film, Novel pharma, and research funding from Teijin
and Novartis.
C. Morizane received honoraria from Pfizer, Novartis,
Fujifilm, Novel pharma, Yakult Honsha and research funding from GlaxoSmithKline, Pfizer, Nobelpharma,
Eisai, Yakult Honsha, ONO PHARMACEUTICAL, Taiho
Pharmaceutical.
N.Mizuno has received research funding from Zeria
Pharmaceutical, Taiho Pharmaceutical Co. Ltd., Merck
Serono, AstraZeneca, NanoCarrier, Eisai, and MSD, and
honoraria from Taiho Pharmaceutical Co. Ltd., Elli Lilly
Japan K.K., Yakult Honsha, Novartis, Pfizer, and Kyowa-
Hakko Kirin.
T Okusaka received honoraria from Novartis Pharma,
Taiho Pharmaceutical Merck Serono, Eli Lilly, Dainippon
Sumitomo Pharma, Bayer Yakuhin, Yakult, Nobelpharma,
Nippon Kayaku, Baxter, Astellas Pharma, FUJIFILM RI
Pharma, AstraZeneca, Ono Pharmaceutical, EA Pharma,
Nippon Chemiphar, Daiichi Sankyo, Celgene, Eli Lilly Japan
K.K., and research funding from Eisai, Novartis Pharma,
Yakult Honsha, Taiho, Nippon Boehringer Ingelheim, Kowa
Company, Kyowa Hakko Kirin.
W hosoda and K hara does not have conflict-of-interest.
References
- Pape UF, Jann H, Müller-Nordhorn J, Bockelbrink A, Berndt U, Willich SN, et al. Prognostic relevance of a novel TNM classification system for upper gastroenteropancreatic neuroendocrine tumors. Cancer 2008;113:256-65. [PMID: 18506737].
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system: World Health Organization; 2010.
- Sorbye H, Welin S, Langer SW, Vestermark LW, Holt N, Osterlund P, et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Ann Oncol 2013;24:152-60. [PMID: 22967994].
- Network. NCC. Neuroendocrine Tumors (Version3.2017). [Available from: https://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf].
- Vélayoudom-Céphise F-L, Duvillard P, Foucan L, Hadoux J, Chougnet CN, Leboulleux S, et al. Are G3 ENETS neuroendocrine neoplasms heterogeneous? Endocr Relat Cancer 2013;20:649-57.
- Basturk O, Yang Z, Tang LH, Hruban RH, Adsay V, McCall CM, et al. The high-grade (WHO G3) pancreatic neuroendocrine tumor category is morphologically and biologically heterogenous and includes both well differentiated and poorly differentiated neoplasms. Am J Surg Pathol 2015;39:683-90.[PMID: 25723112].
- Heetfeld M, Chougnet CN, Olsen IH, Rinke A, Borbath I, Crespo G, et al. Characteristics and treatment of patients with G3 gastroenteropancreatic neuroendocrine neoplasms. Endocr Relat Cancer 2015;22:657-64. [PMID: 26113608].
- Hijioka S, Hosoda W, Matsuo K, Ueno M, Furukawa M, Yoshitomi H, et al. Rb loss and KRAS mutation are predictors of the response to platinum-based chemotherapy in pancreatic neuroendocrine neoplasm with grade 3: A Japanese multicenter pancreatic NEN-G3 study. Clin Cancer Res 2017. [PMID: 28455360].
- Hijioka S, Hosoda W, Mizuno N, Hara K, Imaoka H, Bhatia V, et al. Does the WHO 2010 classification of pancreatic neuroendocrine neoplasms accurately characterize pancreatic neuroendocrine carcinomas? J Gastroenterol 2014;50:564-72. [PMID: 25142799].
- Milione M, Maisonneuve P, Spada F, Pellegrinelli A, Spaggiari P, Albarello L, et al. The Clinicopathologic Heterogeneity of Grade 3 Gastroenteropancreatic Neuroendocrine Neoplasms: Morphological Differentiation and Proliferation Identify Different Prognostic Categories. Neuroendocrinology 2017;104:85-93. [PMID: 26943788].
- Raj N, Valentino E, Capanu M, Tang LH, Basturk O, Untch BR, et al. Treatment Response and Outcomes of Grade 3 Pancreatic Neuroendocrine Neoplasms Based on Morphology: Well Differentiated Versus Poorly Differentiated. Pancreas 2017;46:296-301. [PMID: 27759713].
- Tang LH, Basturk O, Sue JJ, Klimstra DS. A Practical Approach to the Classification of WHO Grade 3 (G3) Well-differentiated Neuroendocrine Tumor (WD-NET) and Poorly Differentiated Neuroendocrine Carcinoma (PD-NEC) of the Pancreas. Am J Surg Pathol 2016; 40:1192-202.[PMID: 27259015].
- Tang LH, Untch BR, Reidy DL, O'Reilly E, Dhall D, Jih L, et al. Well-Differentiated Neuroendocrine Tumors with a Morphologically Apparent High-Grade Component: A Pathway Distinct from Poorly Differentiated Neuroendocrine Carcinomas. Clin Cancer Res 2016;22:1011-7. [PMID: 26482044].
- Ito T, Igarashi H, Nakamura K, Sasano H, Okusaka T, Takano K, et al. Epidemiological trends of pancreatic and gastrointestinal neuroendocrine tumors in Japan: a nationwide survey analysis. J Gastroenterol 2014;50:58-64. [PMID: 24499825].
- Brenner B, Tang LH, Klimstra DS, Kelsen DP. Small-cell carcinomas of the gastrointestinal tract: a review. J Clin Oncol 2004;22:2730-9. [PMID: 15226341].
- Yamaguchi T, Machida N, Morizane C, Kasuga A, Takahashi H, Sudo K, et al. Multicenter retrospective analysis of systemic chemotherapy for advanced neuroendocrine carcinoma of the digestive system. Cancer Sci 2014;105:1176-81. [PMID: 24975505].
- Terashima T, Morizane C, Hiraoka N, Tsuda H, Tamura T, Shimada Y, et al. Comparison of chemotherapeutic treatment outcomes of advanced extrapulmonary neuroendocrine carcinomas and advanced small-cell lung carcinoma. Neuroendocrinology 2012;96:324-32. [PMID: 22572060].
- Strosberg JR, Cheema A, Weber J, Han G, Coppola D, Kvols LK. Prognostic validity of a novel American Joint Committee on Cancer Staging Classification for pancreatic neuroendocrine tumors. J Clin Oncol 2011;29:3044-9. [PMID: 21709192].
- Basturk O, Tang L, Hruban RH, Adsay V, Yang Z, Krasinskas AM, et al. Poorly differentiated neuroendocrine carcinomas of the pancreas: a clinicopathologic analysis of 44 cases. Am J Surg Pathol 2014;38:437-47. [PMID: 24503751].
- Guo C, Chen X, Xiao W, Wang Q, Sun K, Wang Z. Pancreatic neuroendocrine neoplasms at magnetic resonance imaging: comparison between grade 3 and grade 1/2 tumors. Onco Targets Ther 2017;10:1465-74. [PMID: 28331340].
- Santhanam P, Chandramahanti S, Kroiss A, Yu R, Ruszniewski P, Kumar R, et al. Nuclear imaging of neuroendocrine tumors with unknown primary: why, when and how? Eur J Nucl Med Mol Imaging 2015;42:1144-55. [PMID: 25771906].
- Oh S, Prasad V, Lee DS, Baum RP. Effect of Peptide Receptor Radionuclide Therapy on Somatostatin Receptor Status and Glucose Metabolism in Neuroendocrine Tumors: Intraindividual Comparison of Ga-68 DOTANOC PET/CT and F-18 FDG PET/CT. International journal of molecular imaging 2011;2011:524130. [PMID: 22121482].
- Severi S, Nanni O, Bodei L, Sansovini M, Ianniello A, Nicoletti S, et al. Role of 18FDG PET/CT in patients treated with 177Lu-DOTATATE for advanced differentiated neuroendocrine tumours. Eur J Nucl Med Mol Imaging 2013;40:881-8. [PMID: 23443937].
- Binderup T, Knigge U, Loft A, Federspiel B, Kjaer A. 18F-fluorodeoxyglucose positron emission tomography predicts survival of patients with neuroendocrine tumors. Clin Cancer Res 2010;16:978-85. [PMID: 20103666].
- Sadowski SM, Neychev V, Millo C, Shih J, Nilubol N, Herscovitch P, et al. Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites. J Clin Oncol 2016;34:588-96. [PMID: 26712231].
- Olsen IH, Langer SW, Federspiel BH, Oxbol J, Loft A, Berthelsen AK, et al. (68) Ga-DOTATOC PET and gene expression profile in patients with neuroendocrine carcinomas: strong correlation between PET tracer uptake and gene expression of somatostatin receptor subtype 2. Am J Nucl Med Mol Imaging 2016;6:59-72. [PMID: 27069766].
- Chan DL, Pavlakis N, Schembri GP, Bernard EJ, Hsiao E, Hayes A, et al. Dual Somatostatin Receptor/FDG PET/CT Imaging in Metastatic Neuroendocrine Tumours: Proposal for a Novel Grading Scheme with Prognostic Significance. Theranostics 2017;7:1149-58. [PMID: 28435454].
- Rosa S, Capella C, Sessa F, Riva C, Leone BE, Klersy C, et al. Prognostic criteria in nonfunctioning pancreatic endocrine tumours. Virchows Archiv 1996;429:323-33. [PMID: 8982376].
- Rigaud G, Missiaglia E, Moore PS, Zamboni G, Falconi M, Talamini G, et al. High resolution allelotype of nonfunctional pancreatic endocrine tumors: identification of two molecular subgroups with clinical implications. Cancer Res 2001;61:285-92. [PMID: 11196176].
- Rindi G, Klöppel G, Couvelard A, Komminoth P, Körner M, Lopes J, et al. TNM staging of midgut and hindgut (neuro) endocrine tumors: a consensus proposal including a grading system. Virchows Archiv 2007;451:757-62. [PMID: 17674042].
- Steinmüller T, Kianmanesh R, Falconi M, Scarpa A, Taal B, Kwekkeboom DJ, et al. Consensus guidelines for the management of patients with liver metastases from digestive (neuro) endocrine tumors: foregut, midgut, hindgut, and unknown primary. Neuroendocrinology 2008;87:47-62. [PMID: 18097131].
- Rindi G, Falconi M, Klersy C, Albarello L, Boninsegna L, Buchler M, et al. TNM staging of neoplasms of the endocrine pancreas: results from a large international cohort study. J Natl Cancer Inst 2012. [PMID: 22525418].
- Scarpa A, Mantovani W, Capelli P, Beghelli S, Boninsegna L, Bettini R, et al. Pancreatic endocrine tumors: improved TNM staging and histopathological grading permit a clinically efficient prognostic stratification of patients. Mod Pathol 2010;23:824-33. [PMID: 20305616].
- Fazio N, Milione M. Heterogeneity of grade 3 gastroenteropancreatic neuroendocrine carcinomas: New insights and treatment implications. Cancer Treat Rev 2016;50:61-7. [PMID: 27636009].
- Mikami Y, Ueno T, Yoshimura K, Tsuda H, Kurosumi M, Masuda S, et al. Interobserver concordance of Ki67 labeling index in breast cancer: Japan Breast Cancer Research Group Ki67 ring study. Cancer Sci 2013;104:1539-43. [PMID: 23905924].
- Dowsett M, Nielsen TO, A’Hern R, Bartlett J, Coombes RC, Cuzick J, et al. Assessment of Ki67 in breast cancer: recommendations from the International Ki67 in Breast Cancer working group. J Natl Cancer Inst 2011. [PMID: 21960707].
- Hasegawa T, Yamao K, Hijioka S, Bhatia V, Mizuno N, Hara K, et al. Evaluation of Ki-67 index in EUS–FNA specimens for the assessment of malignancy risk in pancreatic neuroendocrine tumors. Endoscopy 2014;46:32-8. [PMID: 24218309].
- Panzuto F, Cicchese N, Partelli S, Rinzivillo M, Capurso G, Merola E, et al. Impact of Ki67 re-assessment at time of disease progression in patients with pancreatic neuroendocrine neoplasms. PloS one 2017;12:e0179445. [PMID: 28644861].
- Jiao Y, Shi C, Edil BH, de Wilde RF, Klimstra DS, Maitra A, et al. DAXX/ATRX, MEN1, and mTOR pathway genes are frequently altered in pancreatic neuroendocrine tumors. Science (New York, NY) 2011;331:1199-203. [PMID: 21252315].
- Heaphy CM, de Wilde RF, Jiao Y, Klein AP, Edil BH, Shi C, et al. Altered telomeres in tumors with ATRX and DAXX mutations. Science (New York, NY) 2011;333:425. [PMID: 21719641].
- Marinoni I, Kurrer AS, Vassella E, Dettmer M, Rudolph T, Banz V, et al. Loss of DAXX and ATRX are associated with chromosome instability and reduced survival of patients with pancreatic neuroendocrine tumors. Gastroenterology 2014;146:453-60.e5. [PMID: 24148618].
- Scarpa A, Chang DK, Nones K, Corbo V, Patch AM, Bailey P, et al. Whole-genome landscape of pancreatic neuroendocrine tumours. Nature 2017;543:65-71. [PMID: 28199314].
- Cao Y, Gao Z, Li L, Jiang X, Shan A, Cai J, et al. Whole exome sequencing of insulinoma reveals recurrent T372R mutations in YY1. Nat Commun 2013;4:2810. [PMID: 24326773].
- Konukiewitz B, Schlitter AM, Jesinghaus M, Pfister D, Steiger K, Segler A, et al. Somatostatin receptor expression related to TP53 and RB1 alterations in pancreatic and extrapancreatic neuroendocrine neoplasms with a Ki67-index above 20. Mod Pathol 2017;30:587-98. [PMID: 28059098].
- Yachida S, Vakiani E, White CM, Zhong Y, Saunders T, Morgan R, et al. Small cell and large cell neuroendocrine carcinomas of the pancreas are genetically similar and distinct from well-differentiated pancreatic neuroendocrine tumors. Am J Surg Pathol 2012;36:173. [PMID: 22251937].
- Missiaglia E, Dalai I, Barbi S, Beghelli S, Falconi M, dellaPeruta M, et al. Pancreatic endocrine tumors: expression profiling evidences a role for AKT-mTOR pathway. J Clin Oncol 2010;28:245-55. [PMID: 19917848].
- Ohmoto A, Rokutan H, Yachida S. Pancreatic neuroendocrine neoplasms: basic biology, current treatment strategies and prospects for the future. Int J Mol Sci 2017;18:143. [PMID: 28098761].
- Raj N, Valentino E, Capanu M, Tang LH, Basturk O, Untch BR, et al. Treatment Response and Outcomes of Grade 3 Pancreatic Neuroendocrine Neoplasms Based on Morphology: Well Differentiated Versus Poorly Differentiated. Pancreas 2016. [PMID: 27759713].
- Umemura S, Mimaki S, Makinoshima H, Tada S, Ishii G, Ohmatsu H, et al. Therapeutic priority of the PI3K/AKT/mTOR pathway in small cell lung cancers as revealed by a comprehensive genomic analysis. J Thorac Oncol 2014;9:1324-31. [PMID: 25122428].
- Shida T, Kishimoto T, Furuya M, Nikaido T, Koda K, Takano S, et al. Expression of an activated mammalian target of rapamycin (mTOR) in gastroenteropancreatic neuroendocrine tumors. Cancer Chemother Pharmacol 2010;65:889-93. [PMID: 19657638].
- Catena L, Bajetta E, Milione M, Ducceschi M, Valente M, Dominoni F, et al. Mammalian target of rapamycin expression in poorly differentiated endocrine carcinoma: clinical and therapeutic future challenges. Target Oncol 2011;6:65-8. [PMID: 21468754].
- Fonseca PJ, Uriol E, Galvan JA, Alvarez C, Perez Q, Villanueva N, et al. Prolonged clinical benefit of everolimus therapy in the management of high-grade pancreatic neuroendocrine carcinoma. Case Rep Oncol 2013;6:441-9. [PMID: 24019785].
- Tanaka H, Matsusaki S, Baba Y, Isono Y, Kumazawa H, Sase T, et al. Neuroendocrine tumor G3: a pancreatic well-differentiated neuroendocrine tumor with a high proliferative rate. Clin J Gastroenterol 2015;8:414-20. [PMID: 26439620].
- Ikeda M, Okuyama H, Takahashi H, Ohno I, Shimizu S, Mitsunaga S, et al. Chemotherapy for advanced poorly differentiated pancreatic neuroendocrine carcinoma. J Hepatobiliary Pancreat Sci 2015; 22:623-7. [PMID: 25755102].
- Garcia-Carbonero R, Sorbye H, Baudin E, Raymond E, Wiedenmann B, Niederle B, et al. ENETS Consensus Guidelines for High-Grade Gastroenteropancreatic Neuroendocrine Tumors and Neuroendocrine Carcinomas. Neuroendocrinology 2016;103:186-94. [PMID: 26731334].
- Roquin G, Baudin E, Lombard-Bohas C, Cadiot G, Dominguez S, Guimbaud R, et al. Chemotherapy in Well-Differentiated Pancreatic Neuroendocrine Tumours with Ki-67 >/=10%: Is there a More Effective Antitumor Regimen A Retrospective Multicentric Study of the French Group of Endocrine Tumours (GTE). Neuroendocrinology 2017. [PMID: 28152531].
- Cives M, Strosberg J. Treatment Strategies for Metastatic Neuroendocrine Tumors of the Gastrointestinal Tract. Curr Treat Options Oncol 2017;18:14. [PMID: 28286921].
- Kos-Kudla B, Cwikla J, Ruchala M, Hubalewska-Dydejczyk A, Jarzab B, Krajewska J, et al. Current treatment options for gastroenteropancreatic neuroendocrine tumors with a focus on the role of lanreotide. Contemp Oncol (Pozn) 2017;21:115-22. [PMID: 28947880].
- Kim ST, Ha SY, Lee S, Ahn S, Lee J, Park SH, et al. The Impact of PD-L1 Expression in Patients with Metastatic GEP-NETs. J Cancer 2016;7:484-9. [PMID: 26958083].

