Keywords
Memantine; Donepezil; Concomitant therapy; SPECT; Cerebral blood flow; BPSD
Introduction
Six years have passed since the glutamate NMDA receptor (NMDA-R) antagonist, memantine hydrochloride (Memary), was first approved for use in Japan for the treatment of Alzheimer's disease (AD). Memantine has since been administered to numerous AD patients, and has been frequently reported to be more effective against the behavioral and psychological symptoms of dementia (BPSD) than against its core symptoms.
In the U.S. and Europe, where it has been used for more than ten years, multicenter trials have been conducted reporting that memantine is effective against BPSD [1,2]. On the other hand, the results of a six-study meta-analysis on the usefulness of memantine against moderate to severe AD demonstrated that memantine exhibits ameliorative effects not only on BPSD, but also on cognitive function and general clinical symptoms [3].
Moreover, memantine can be used in combination with acetyl cholinesterase inhibitor (AchE-I) since it has a different mechanism of action, and the efficacy of this combination has also been reported overseas [4-7]. In Japan it is approved that we administer memantine alone or add on to donepezil for AD.
We examined memantine, either alone or in combination with donepezil, on both clinical efficacy on cognitive functions & the behavioral and psychological symptoms of dementia (BPSD) and the changes in cerebral blood flow in patients with AD.
Materials and Methods
Comparison of changes in cerebral blood flow
Subject cases
• Single administration of memantine: 12 cases who were diagnosed with probable AD according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) diagnostic criteria, consisting of outpatients of this department who had entered a domestic phase III clinical trial and had been administered 20 mg/days for 6 months of memantine (average age: 78.2, average MMSE score: 21.4).
• Concomitant administration of memantine and donepezil: 26 cases consisting of AD who were diagnosed with probable AD according to the NINCDS-ADRDA diagnostic criteria, outpatients of this department who were additionally administered 20 mg/days for 6 months of memantine after having taken donepezil for average 14.2 months ( from 6.0 to 18.4 months , average age : 80.4, average MMSE score: 20.6 ).
• Single administration of donepezil: 45 cases consisting of AD who were diagnosed with probable AD according to the NINCDS-ADRDA diagnostic criteria, outpatients of this department who were administered 5 mg of donepezil (average age: 79.4, average MMSE score: 22.4).
Measurement Method
SPECT scans using 99mTc-ECD were performed prior to and six months after administration of each drug.
Comparisons of cerebral blood flow were performed between two groups before and after administration using software Statistical Parametric Mapping (SPM8) that is able to quantify the CBF and to indicate the increase or decrease of CBF on the template after statistical processing [8], running on the MATLAB platform developed by MathWorks, and a comparative study was made between sites of increased and decreased cerebral blood flow.
Changes in cognitive function
MMSE and ADAS-Jcog examinations were performed on two occasions before and roughly six months after additional administration of memantine on 35 cases consisting of outpatients of this department who received additional administration of memantine at up to 20 mg/day following administration of donepezil.
Changes in symptoms following administration were determined through interviews with caregivers. The statistical analysis was used by paired T-test.
Ethical considerations
Informed written consent was obtained from all subjects and their families for blood collection, brain imaging, and psychological testing.
Results
Effect on cerebral blood flow
Changes in cerebral blood flow after single administration of memantine: Changes in cerebral blood flow after administration of memantine at 20 mg/day for six months are shown (Figure 1).
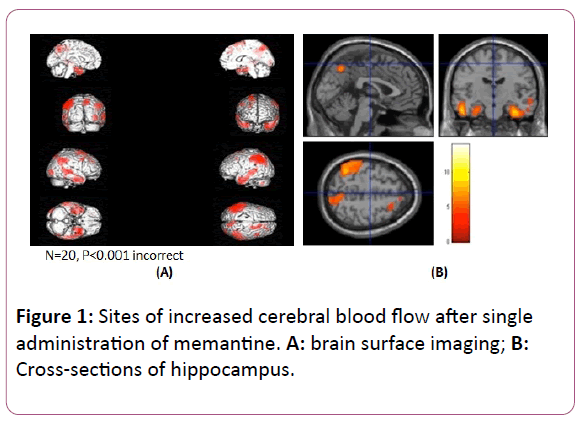
Figure 1: Sites of increased cerebral blood flow after single administration of memantine. A: brain surface imaging; B: Cross-sections of hippocampus.
Although brain surface imaging indicated left dominance after administration, significant increases in blood flow were observed bilaterally over a comparatively wide range from the angular gyrus to the inferior, middle and superior temporal gyrus, bilaterally from the posterior cingulate gyrus to the precuneus, and locally in the right frontal lobe and occipital lobe (Figure 1A). In central cross-sections of the hippocampus, significant increases in blood flow were observed bilaterally in the hippocampus and Para hippocampal gyrus (Figure 1B). Significant increases in blood flow were observed bilaterally with left dominance from the angular gyrus to the inferior, middle and superior temporal gyrus, bilaterally from the posterior cingulate gyrus to the precuneus and in the right frontal lobe and occipital lobe.
Cross-sections of the hippocampus revealed significant bilateral increases in blood flow in the hippocampus and Para hippocampal gyrus.
Changes in cerebral blood flow after single administration of donepezil: Figure 2 indicates changes in cerebral blood flow six months after administration of donepezil. Although significant increases in blood flow were indicated bilaterally with left dominance in the supramarginal gyrus, in the right superior frontal gyrus and bilaterally in cerebellar hemisphere, there were no changes in blood flow observed in the hippocampus (Figure 2A and 2B).
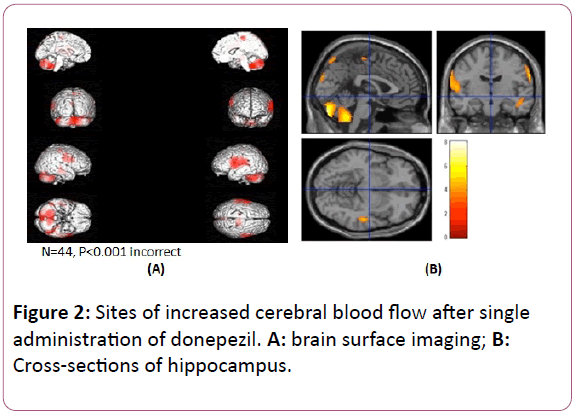
Figure 2: Sites of increased cerebral blood flow after single administration of donepezil. A: brain surface imaging; B: Cross-sections of hippocampus.
Significant increases in blood flow were indicated bilaterally with left dominance in the supramarginal gyrus, in the right superior frontal gyrus, and bilaterally in the cerebellar hemisphere. There were no changes in blood flow observed in the hippocampus.
Changes in cerebral blood flow after additional administration of memantine: Significant increases in blood flow were observed bilaterally over a wide range extending from the orbital gyrus to the anterior cingulate gyrus, bilaterally in a portion of the parietal lobe, from the left angular gyrus to the middle and inferior temporal gyrus, and in the inferior pontine of the brainstem (Figure 3A). In central cross-sections of the hippocampus, increased blood flow was indicated bilaterally over a wide range of the hippocampus (with left dominance) (Figure 3B). A summary of the significant increasing CBF area was showed in Table 1.
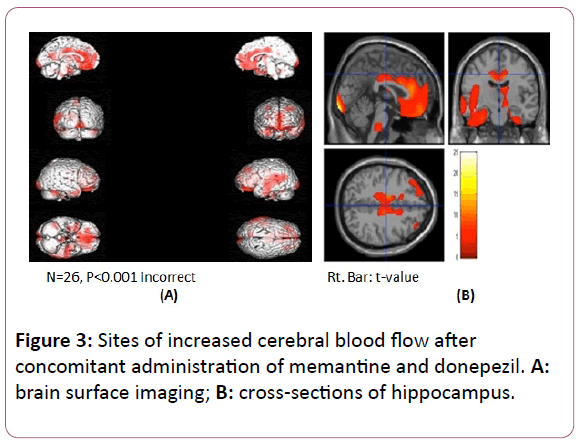
Figure 3: Sites of increased cerebral blood flow after concomitant administration of memantine and donepezil. A: brain surface imaging; B: cross-sections of hippocampus.
| |
Brain area of increases in CBF |
Brodmann area |
| Memantine single |
Bil. angular, inferior,middle and superior temporal gyrus |
Bil. 7, 21, 22, 38, 40 |
| |
Bil. posterior cingulate and precuneus. Rt. frontal and occipital lobe |
Rt. 9, 18 |
| |
Bil. hippocampus and parahippocampal gyrus |
|
| Donepezil single |
Lt. supramarginal gyrus |
Lt. 40 |
| |
Rt. superior fronatal gyrus |
Rt. 5 |
| |
Bil. cerebellar hemisphere |
|
| Memantine + Donepezil |
Bil. orbital, anterior cingulate gyrus and parietal lobe |
Bil. 12,21,22, 32,33 |
| |
Lt. angular, middle and inferior temporal gyrus |
Lt. 39,40 |
| |
Inferior pontine |
|
| |
Hippocampus |
|
Table 1: The area of significant increases in CBF following administration of donepezil and memantine single use, and combination donepezil and memantine.
Significant increases in blood flow were observed over a wide area extending bilaterally from the orbital gyrus to the anterior cingulate gyrus, bilaterally in a portion of the parietal lobe, from the left angular gyrus to the middle and inferior temporal gyrus, and in the inferior pontine of the brainstem. Cross-sections of the hippocampus revealed bilaterally increased blood flow over a wide range of the hippocampus with left dominance.
Changes in cognitive function and symptoms
• Cognitive function: Average MMSE scores changed from 20.6 to 20.1 while average ADAS-Jcog scores changed from 18.0 to 16.4 before and after administration of memantine, and although ADAS-Jcog scores exhibited slight improvement, significant differences were not obtained.
• Changes in dementia symptoms: On the basis of interviews conducted with caregivers, some degree of improvement of symptoms was observed in 30 of 35 cases (85.7%) following additional administration of memantine (Table 2).
| Effective |
30 cases ( 85.7% ) |
| No change |
5 cases ( 14.3% ) |
| Ineffective, Deterioration |
0 cases ( 0% ) |
Table 2: The degree of improvement of symptoms.
Improvement was observed with respect to increased conversation, reduced irritation and agitation, increased motivation, elimination or reduction of wandering, elimination of hallucinations and delusions and improvement of memory impairment, with ameliorative effects consisting primarily of improvement of BPSD (Table 3).
| Improved symptoms |
No. of cases |
% |
| Increased conversation |
11 |
31.4 |
| Reduced irritation and agitation |
12 |
34.3 |
| Increased motivation |
6 |
17.1 |
| Elimination or reduction of wandering |
4 |
11.4 |
| Elimination of hallucinations and delusions |
4 |
11.4 |
| Improvement of memory impairment |
2 |
5.7 |
Table 3: Improvement of symptoms after administration of memantine. Improvement of at least some symptoms was observed in 85.7% of the cases following additional administration of memantine. These effects consisted mainly of improvement of BPSD.
Discussion
Characteristics of memantine and cognitive function
Memantine is an antagonist of an intracerebral excitatory neurotransmitter in the form of NMDA-R, a type of glutamate receptor. NMDA-R are densely located in the hippocampus and are thought to be deeply involved in the relationship with longterm potentiation (LTP) considered to be required for memory and learning [8]. In AD, accumulation of amyloid β (Aβ) extends to NMDA-R, and ends up directly damaging nerve cells by causing an excessive influx of calcium into the cells as a result of damaging these receptors [9]. In addition, persistent increases in glutamate levels result in over-activation of NMDA-R, thereby causing memory and learning impairment as a result of interfering with normal neurotransmission signals [10]. Memantine acts to improve memory and protect nerve cells without inhibiting LTP by gently binding to NMDA-R.
Although increases in blood flow were observed from the hippocampus to the parahippocampal gyrus following administration of memantine, it is unlikely that memantine directly causes an increase in blood flow in the hippocampus, but rather the increase in blood flow is presumed to be the result of protecting nerve cells of the hippocampus. This increase in blood flow around the hippocampus was not observed following administration of donepezil (Figure 2), and well-defined post-administration increases in blood flow in the hippocampus were also not obtained in similar studies that we conducted on other Ach-E inhibitors consisting of galantamine and rivastigmine. These findings suggest that memantine will be the only drug causing a change in blood flow around the hippocampus in the future as well.
Moreover, in addition to the hippocampus, although increased blood flow was also observed with left dominance from the angular gyrus to the superior, middle and inferior temporal gyrus, it is interesting to note that these findings correlate with the results (literature) of a phase III clinical trial conducted in Japan on changes in categories of the SIB-J that indicated significant improvements in the areas of attention, execution, visual-spatial ability and language in a memantine dose group in comparison with a placebo group11). The correlation between improvement of language as determined according to the SIB-J and increased blood flow in Wernicke's area observed in this study is particularly interesting.
Concomitant effects of memantine and donepezil
With respect to changes in clinical symptoms after additional administration of memantine following administration of donepezil, although improvement of cognitive function in terms of the MMSE and ADAS-Jcog evaluation scales was not observed in the study conducted by the authors, concomitant administration of memantine and donepezil was clearly determined to have an effect on BPSD based on interviews with caregivers. Improvement of positive parameters such as reduced irritation and agitation and elimination of hallucinations and delusions was more conspicuous than improvement of negative parameters such as decreased motivation. In addition, increases in the amount of conversation were observed in more than 30% of the cases following concomitant administration of memantine. The following provides a discussion of the correlation between improvement of these symptoms and increased cerebral blood flow.
The amount of conversation was clearly demonstrated to increase following concomitant administration of donepezil in the same manner as in the domestic clinical trial using single administration of memantine. As shown in Figure 3, this is thought to be due to memantine inducing increased blood flow in the left temporal lobe, which correlates with Wernicke's area.
Moreover, remarkable improvement of blood flow was obtained bilaterally from the orbital gyrus to the anterior cingulate gyrus following administration of memantine. The orbitofrontal cortex of the orbital gyrus is considered to be involved in integration of sensory information and decisionmaking [12-14], and unnatural decreases in glutamate activity levels in the anterior cingulate cortex [15] and excessive increases in glutamate activity levels in other areas are observed in patients with obsessive-compulsive disorder. On the basis of these findings, the possibility is suggested that increased blood flow in the anterior cingulate gyrus results in reduced agitation, delusions and hallucinations.
In an overseas study on the concomitant use of donepezil and memantine [16], although significant improvement in comparison with single administration of donepezil was demonstrated in the three categories of memory, execution and language with respect to changes in the scores of individual categories of the SIB, improvement of memory as determined according to the SIB-J was not obtained in a domestic clinical trial on single administration of memantine [11]. The advantageous action of improving memory attributable to concomitant use of memantine and donepezil in comparison with donepezil alone may be able to be explained based on the increase in blood flow in the anterior cingulate gyrus following additional administration of memantine and the prominent enhancement of blood flow in the hippocampus accompanying concomitant use of memantine and donepezil (Figure 3).
Increases in blood flow were unable to be obtained in the region from the orbital gyrus to the anterior cingulate gyrus with single administration of memantine or donepezil, and as a result, donepezil and memantine are thought to have some type of synergistic effect. Although the mechanism responsible for this is unclear, when acetylcholine concentrations were measured in the cerebral cortex and hippocampus following administration of donepezil and memantine to fasting rats, an amount equal to twice the total attributable to the two administered drugs is reported to have been detected [17]. Although these results were obtained from an animal study, these are interesting results that suggest the possibility that the action of memantine and donepezil is enhanced by concomitant administration.
In this study, although increases in blood flow following single administration of donepezil were observed at sites localized in the left supramarginal gyrus, upper right frontal lobe and cerebellar hemisphere, according to the results of a study by the authors focusing on the efficacy of administering 10 mg of donepezil on advanced AD [18], a prominent increase in blood flow was observed from the right parietal lobe to the occipital lobe after increasing the dosage of donepezil from 5 mg to 10 mg. This result is thought to suggest that the action of increasing cerebral blood flow attributable to donepezil exhibits dosedependency to a certain degree.
Conclusion
Since memantine is effective against BPSD associated with AD, it is thought to be a drug that can be good news for both patients and caregivers. In addition, since memantine has the unique mechanism of gradually inhibiting NMDA-R, it also demonstrates the action of protecting nerve cells, thereby also having the potential for use in disease modifying therapy. Since memantine has been used in the U.S. and Europe since 2003, although there are numerous papers describing the efficacy of concomitant use with donepezil, papers have also been published indicating that concomitant use with donepezil is not useful, perhaps in consideration of health economics19). Since concomitant studies have also been conducted in Japan following the release of donepezil and memantine, it is expected that study results indicating the usefulness of concomitant administration will be obtained in the near future.
References
- Gauthier S, Loft H, Cummings J (2008) Improvement in behavioral symptoms in patients with moderate to severe Alzheimer's disease by memantine: a pooled data analysis. Int J Geriatr Psychiatry 235: 537-545.
- Wilcock GK, Ballard CG, Cooper JA, Loft H (2008) Memantine for agitation/aggression and psychosis in moderately severe to severe Alzheimer's disease: a pooled analysis of 3 studies. J Clin Psychiatry 69: 341-348.
- Winblad B1, Jones RW, Wirth Y, Stöffler A, Möbius HJ (2007) Memantine in moderate to severe Alzheimer's disease: a meta-analysis of randomized clinical trials. Dement Geriatr Cogn Disord 24: 20-27.
- Cummings JL, Schneider E, Tariot PN, Graham SM. Memantine MEM-MD-02 (2006) Study Group Behavioral effects of memantine in Alzheimer disease patients receiving donepezil treatment. Neurology 67: 57-63.
- Tariot PN, Farlow MR, Grossberg GT, Graham SM, McDonald S, et al. (2004) Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 291: 317-324.
- Lopez OL, Becker JT, Wahed AS, Saxton J, Sweet RA, et al. (2009) Long-term effects of the concomitant use of memantine with cholinesterase inhibition in Alzheimer disease. J Neurol Neurosurg Psychiatry 80: 600-607.
- Patel L, Grossberg GT (2011) Combination therapy for Alzheimer's disease. Drugs Aging 28: 539-546.
- William D Penny (2006) Statistical Parametric Mapping: The Analysis of Functional Brain Images.
- Bliss TV, Lomo T (1973) Long-lasting potentiation of synaptic transmission in the dentate area, of the anaesthetized rabbit following stimulation of the perforant path. J Physiol 2: 331-356.
- Cowburn RF, Wiehager B, Trief E, Li-Li M, Sundström E (1997) Effects of beta-amyloid- (25-35) peptides on radioligand binding to excitatory amino acid receptors and voltage-dependent calcium channels: evidence for a selective affinity for the glutamate and glycine recognition sites of the NMDA receptor. Neurochem Res 22: 1437-1442.
- Le WD, Colom LV, Xie WJ, Smith RG, Alexianu M, et al. (1995) Cell death induced by beta-amyloid 1-40 in MES 23.5 hybrid clone: the role of nitric oxide and NMDA-gated channel activation leading to apoptosis. Brain Res 686: 49-60.
- Yu Nakamura Y, Kitamura S, Homma A, Shiosakai K, Matsui D (2014) Efficacy and safety of memantine in patients with moderate-to-severe Alzheimer's disease: results of a pooled analysis of two randomized, double-blind, placebo-controlled trials in Japan. Expert Opin Pharmac Other 15: 913-925.
- Kringelbach ML (2005) The orbitofrontal cortex: linking reward to hedonic experience. Nature Reviews Neuroscience 6: 691-702.
- Bush G, Luu P, Posner MI (2000) Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn Sci 4: 215-222.
- Posner MI, DiGirolamo GJ (1998) Executive attention: Conflict, target detection, and Cognitive Control.
- Nieuwenhuis S, Ridderinkhof KR, Blom J, Band GP, Kok A (2001) Error-related brain potentials are differentially related to awareness of response errors: evidence from an antisaccade task. Psychophysiology 38: 752-760.
- Schmitt FA, van Dyck CH, Wichems CH, Olin JT (2006) Memantine MEM-MD-02 Study Group Cognitive response to memantine in moderate to severe Alzheimer disease patients already receiving donepezil: an exploratory reanalysis. Alzheimer Dis Assoc Disord 20: 255-262.
- Ihalainen J, Sarajärvi T, Rasmusson D, Kemppainen S, Keski-Rahkonen P, et al. (2011) Effects of memantine and donepezil on cortical and hippocampal acetylcholine levels and object recognition memory in rats. Neuropharmacology 61: 891-899.
- Kanaya K, Abe S, Sakai M, Fujii H, Koizumi K, et al (2012) Efficacy of a high dosage of donepezil for Alzheimer's disease as examined by single-photon emission computed tomography imaging. Psychogeriatrics 12: 172-178.
- Howard R, McShane R, Lindesay J, Ritchie C, Adams J, et al. (2012) Donepezil and memantine for moderate-to-severe Alzheimer's disease. N Engl J Med 366: 893-903.

