Nevin Oruc1, Janette Lamb1, Onur Cagri Kutlu4, M Michael Barmada2, Mary E Money5, Adam Slivka1, David C Whitcomb1,2,3
1Department of Medicine, Division of Gastroenterology, 2Human Genetics, 3Cell Biology and
Physiology, and the Center for Genomic Sciences, University of Pittsburgh. Pittsburgh, PA, USA.
4GATA Medical School, General Surgery Department. Ankara, Turkey.
5Washington County Hospital. Hagerstown, MD, USA
- *Corresponding Author:
- David C Whitcomb
Division of Gastroenterology
Hepatology and Nutrition Mezz. Level, C Wing
UPMC Presbyterian 200 Lothrop
St. Pittsburgh, PA USA
Phone +1-412.648.9604
Fax +1-412.383.7236
E-mail whitcomb@pitt.edu
Received July 14th, 2004 - Accepted September 7th, 2004
Keywords
Pancreatitis; Polymorphism (Genetics); Renin-Angiotensin System
Abbreviations
ACE: angiotensin converting enzyme; HIPAA: the Health Insurance Portability and Accountability Act; HP: hereditary pancreatitis; IRB: institutional review board; NAPS2: North American Pancreatitis Study 2; RAS: renin angiotensin system
INTRODUCTION
Chronic pancreatitis is an inflammatory disease which leads to pancreatic fibrosis and the destruction of the exocrine and the endocrine pancreas [1]. Pancreatitis appears to be a complex disorder reflecting the interaction of various genetic and environmental factors [2, 3]. However, the major common genetic risk factors have yet to be defined.
The renin-angiotensin system (RAS) is a circulatory cascade system primarily involved in the regulation of blood pressure and serum electrolytes [4, 5]. The key enzyme in this system is the angiotensin converting enzyme (ACE) which converts angiotensin I to the potent vasoconstrictor angiotensin II [4, 5, 6]. The RAS has been said to be involved in the pathogenesis of several diseases including fibrosis in the heart, kidney, lung and liver during chronic inflammation through the regulation of cell growth, inflammation, oxidative stress and fibrosis [7, 8, 9, 10].
The ACE gene insertion/deletion (I/D) polymorphism was first identified in 1990 [11]. The ACE-D, a deletion polymorphism of a 287-bp fragment of intron 16 of the ACE gene allele, has been shown to result in higher levels of circulating enzyme in a dose dependent manner [11]. The role of the ACE gene I/D polymorphism as a risk factor has been investigated in several diseases. The ACE deletion (DD) genotype, for example, results in a 1.3 fold increased risk of myocardial infarction [12]. Recent studies have shown that the RAS is intrinsically present in the pancreas [13] and its genetic expression is enhanced during acute pancreatitis and chronic pancreatic hypoxia in experimental animals [14, 15]. Furthermore, the pharmacological blockage of ACE significantly attenuated pancreatic fibrosis in an experimental model of chronic pancreatitis in rats [16]. Thus ACE may have a pathogenic role in the development of chronic pancreatitis. However, the prevalence of the ACE I/D polymorphism in chronic pancreatitis and its contribution to the course of the disease has not yet been defined. We therefore investigated the occurrence of the ACE I/D polymorphism in chronic pancreatitis patients and its relationship to the course of the disease.
METHODS
Patients
One hundred fifty five subjects were selected from the institutional review board (IRB) approved, Health Insurance Portability and Accountability Act (HIPAA) compliant, hereditary pancreatitis (HP) study and the North American Pancreatitis Study 2 (NAPS2) pilot study which included a patient group recruited through the University of Pittsburgh Medical Center clinics. Fifty-one cases had familial pancreatitis and 104 cases had sporadic chronic pancreatitis. In addition, 163 healthy controls were evaluated. The controls included spouses of affected individuals from both studies or communitybased controls over 50 years of age who had no prior history of digestive disease.
Data Recording
All subjects completed standardized questionnaires assessing family history, clinical history, environmental exposure (including alcohol consumption and smoking history) and detailed questions about recurrent acute and chronic pancreatitis. The 155 patients selected also provided medical records which included clinical notes, operative notes, discharge summaries, laboratory reports, abdominal imaging reports and pathology reports that elucidated the pattern of the pancreatic disease. The patient information was used to categorize the pancreatitis according to the etiology of pancreatitis, the risk factors and the severity of the disease.
Laboratory Procedure
Genomic DNA was purified from peripheral blood cells of the subjects using a commercially available kit (Puregene DNA isolation kit, Gentra systems, Minneapolis, MN, USA). The ACE genotype was determined by PCR amplification of a genomic DNA fragment on intron 16 of the ACE gene as previously described by Rigat et al. [11]. The forward and reverse primers used were 5- CTGGAGACCACTCCCATCCTTTCT, and 5-GATGTGGCCATCACATTCGTCAGAT, respectively. Amplified ACE gene fragments without insertion (D allele) and with insertion (I allele) of approximate 190 and approximate 490 bp, respectively, were detected on 1% agarose gel containing ethidium bromide. To increase the specificity of DD genotyping, PCR amplifications were performed with an insertion-specific primer pair (5- TGGGACCACAGCGCCCG CCACTAC and 5-TCGCCAGCCCTCCCATGCCCATAA), with 25 μL reactions (0.5 μg genomic DNA, 500 pmol of primers, 0.5 mM each deoxy- ATP, GTP, CTP, TTP, 1.5 mM MgCl2; 0.5 U Taq DNA polymerase), with 1 min of denaturation at 94°C, followed by 30 cycles of 30 s at 94°C, 45 s at 67°C, and 2 min at 72°C. The reaction yields no products in the samples of DD genotype [17]. Only the insertion (I) allele produces a 335-bp amplicon. The 335-bp fragment was identified on 1.5% agarose gel containing ethidium bromide.
ETHICS
The study was conducted with the approval of Institutional Review Board of the University of Pittsburgh. All patients and controls gave written informed consent,
STATISTICS
The results were given as mean±SD or allele frequencies. Data were analyzed by means of the logistic regression, the one- and two-way analysis of variance (ANOVA), and the hierarchical log-linear models. The odds ratios (OR) evaluated by the logistic regression together with their 95% confidence intervals (95% CI) were also reported. Twotailed P values of less than 0.05 were considered statistically significant. The study was powered to detect a relative risk of 3 in the familial pancreatitis group of 88% and in the sporadic chronic pancreatitis group of 97% (https://calculators.stat.ucla.edu/powercalc/)
RESULTS
A group of 51 familial pancreatitis patients (39.1±18.2 years old; F/M: 38/13, 74.5%/25.5%), 104 sporadic chronic pancreatitis (42.7±17.8 years old; F/M: 58/46, 55.8%/44.2%) and 163 healthy controls (60.5±13.3 years old; F/M: 97/66, 59.5%/40.5%) were evaluated. The mean age in the healthy controls was significantly higher than in both the familial and the sporadic chronic pancreatitis patients (P<0.001), while no significant difference was observed between the familial and the chronic pancreatitis patients (P=0.181). The comparison among the 3 groups showed a significantly lower frequency of males in the familial pancreatitis patients (P=0.029).
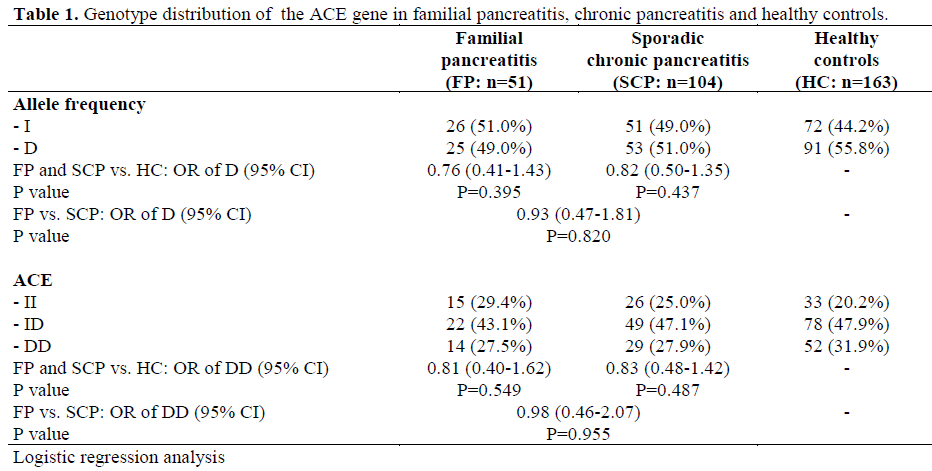
The distribution of the ACE genotype is summarized in Table 1. There were no significant differences in allele distribution among the three groups (overall P=0.601); the ACE-D allele frequency in familial pancreatitis patients (49.0%) was not significantly different (P=0.395) in comparison to controls (55.8%), while the sporadic chronic pancreatitis patients had a 51.0% ACE-D allele frequency (P=0.820 and P=0.437 vs. familial pancreatitis and controls, respectively). Familial pancreatitis cases, chronic pancreatitis cases and controls had a similar ACE-DD genotype frequency (overall P=0.720 among the 3 groups): 27.5% (14/51), 27.9% (29/104), and 31.9% (52/163), respectively (Table 1).
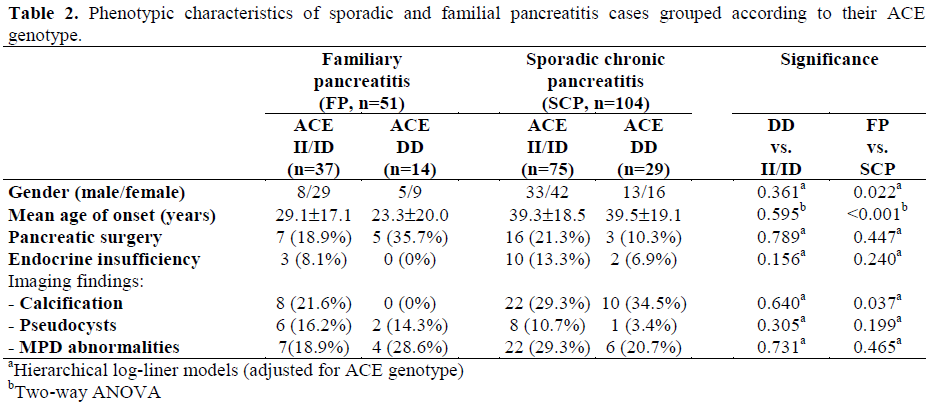
The clinical features of patients with different ACE genotypes are summarized in Table 2. The mean age of the disease onset was 27.5±17.9 in familial pancreatitis cases and 39.4±14.6 in sporadic pancreatitis cases (P<0.001). There was a significantly lower frequency of both male sex (25.5% vs. 44.2%; P=0.022) and calcification (15.7% vs. 30.8%; P=0.037) in patients with familial pancreatitis in comparison to those with sporadic chronic pancreatitis, while no significant differences were detected between patients with ACE-DD and ACE II/ID genotypes (P<0.595, P=0.361, and P=0.640 for age of the disease onset, gender and calcification, respectively). Surgical intervention was reported in 12 of the 51 familial pancreatitis cases and in 19 of the 104 sporadic pancreatitis cases due to pancreatitis-related complications. Endocrine insufficiency was present in 3 familial pancreatitis cases of whom none had the ACE-DD genotype and 12 sporadic pancreatitis cases of whom two had the ACEDD genotype (Table 2). Ten out of 32 sporadic pancreatitis cases with pancreatic calcifications have ACE-DD genotype. None of the familial cases with the ACE-DD genotype had pancreatic calcification. Pancreatic duct abnormalities were reported in 28 sporadic and 11 familial cases. There was no significant relationship between the ACE genotype and pancreatic imaging findings (Table 2).
In sporadic chronic pancreatitis subjects, 44.8% of patients with the DD genotype reported severe pain attacks vs. 53.5% of patients with the ID or II genotype (13/29 DD vs. 40/75 II/ID). Those ratios were 57.1% and 48.6% (8/14 DD vs. 18/37 II/ID) in familial pancreatitis cases, respectively. The differences between the ratios were not significant (P=0.437 and P=0.589 in the sporadic chronic pancreatitis and the familial pancreatitis patients, respectively).
DISCUSSION
The RAS, traditionally known as an endocrine system regulating blood pressure and body fluid homeostasis [18], is also a mediator of normal and pathophysiological processes in a variety of tissues [19]. The ACE plays a central role in this system by converting angiotensin I to the potent vasoconstrictor angiotensin II [20]. Angiotensin II stimulates the proliferation of mesangial cells, cardiac fibroblasts, and hepatic stellate cells and increases the synthesis of extracellular matrix proteins [8, 9, 10, 21]. Thus, RAS is involved in the pathogenesis of fibrosis in tissues including kidney, heart and liver [7, 8, 9, 10]. The deletion type polymorphism in the 16th exon of the ACE gene is associated with elevated serum and cellular ACE levels. The ACE DD genotype is associated with several disorders including cardiac and renal diseases [12, 17] although the magnitude of this association has been questioned [22]. However, the pathological risk of ACE DD genotypes also varies between populations with different genetic and environmental backgrounds [23], suggesting that the ACE DD genotype is acting as a disease modifier rather than as a disease susceptibility factor.
The RAS system has been shown to play an important role in the regulation of pancreatic exocrine and endocrine functions [24]. During acute and chronic inflammation of the pancreas, both circulating ACE activity and intrinsic pancreatic ACE activity is markedly elevated [15, 25, 26]. Recently, Nagashio et al. reported that an ACE directs pancreatic fibrogenesis in experimental animals [27]. Moreover, the inhibition of the RAS with an ACE inhibitor attenuates pancreatic fibrosis in an animal model of chronic pancreatitis [16], suggesting that RAS might play an important role in pancreatic fibrosis. Therefore, we hypothesized that functional the ACE-I/D polymorphism might be a genetic risk factor for chronic pancreatitis This is the first report investigating a potential role of the ACE polymorphism in the susceptibility or progression of chronic pancreatitis. There are notable differences in the distributions of the ACE genotype within and between different populations [28, 29]. In our study, ACE gene I/D allele frequency is similar to previously reported frequencies in American populations [30]. In order to estimate the contribution of the ACE polymorphism to the course of chronic pancreatitis, the clinical signs and symptoms were compared between patients with different ACE genotypes. In contrast to the published studies in renal failure patients [31], the chronic pancreatitis phenotype did not differ between patients with ACE- DD, II or ID genotypes.
Although the RAS participates in the development and the progression of chronic pancreatitis and the inhibition of the ACE appears to improve outcome in some animal models, the functional ACE-DD polymorphism did not appear to influence the susceptibility or the course of chronic pancreatitis in our human study. Several possible explanations were considered: 1) the ACE DD genotype may influence the expression of the ACE in the heart and kidneys but not in the pancreas; 2) the ACE DD genotype may modify the progression of chronic pancreatitis, but this was not detected due to the insensitivity of phenotyping the rate of disease progression in chronic pancreatitis; 3) ACE DD genotypes are an important cofactor in a gene-gene or geneenvironment model which has not yet been resolved, or 4) other RAS-associated enzymes may be more important in the pancreas than the ACE within the pancreas (e.g. portions of the pathway may be bypassed and distal steps in the system activated by digestive enzymes such as trypsin [32]). However, the current results suggest that factors other than ACE expression levels may be important in regulating the RAS system within the pancreas. The fact that the RAS system specifically affects the pancreas also suggests that local, rather than systemic effects, are important in pancreatic diseases.
In conclusion, although the RAS system seems to play a role in the development of pancreatic inflammation and fibrosis, the ACE I/D polymorphism does not play a dominant role in the pathogenesis and the progression of chronic pancreatitis.
Acknowledgements
This work was supported by NIH Grant DK061451 (DCW) and by a scholarship from the Turkish Gastroenterology Association (NO)
References
- Ammann RW, Akovbiantz A, Largiader F, Schueler G. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medicalsurgical series of 245 patients. Gastroenterology 1984; 86:820-8. [PMID 6706066]
- Whitcomb DC. Hereditary pancreatitis. New insights into acute and chronic pancreatitis. Gut 1999; 45:317-22. [PMID 10446089]
- Whitcomb DC, Gorry MC, Preston RA, Furey W, Sossenheimer MJ, Ulrich CD, et al. Hereditary pancreatitis is caused by a mutation in the cationic trypsinogen gene. Nat Genet 1996; 14:141-5. [PMID 8841182]
- Stroth U, Unger T. The renin angiotensin system and its receptors. J Cardiovascular Pharmacol 1999; 33:S21-8. [PMID 10028950]
- Pueyo ME, N`Diaye N, Michael JB. Angiotensin II elicited signal trans-duction via AT 1 receptors in endothelial cells. Br J Pharmacol 1996; 118:79-84. [PMID 8733579]
- Mii S, Ware JA, Mallette SA, Kent KC. Effect of angiotensin II on human vascular smooth muscle cell growth. J Surg Res 1994; 57:174-8. [PMID 8041134]
- Frishman WH, Fozailoff A, Lin C, Dike C. Renin inhibition: a new approach to cardiovascular therapy. J Clin Pharmacol 1994; 34:873-80. [PMID 7983230]
- Ruiz-Ortega M, Ruperez M, Esteban V, Egido J. Molecular mechanisms of angiotensin II-induced vascular injury. Curr Hypertens Rep 2003; 5:73-9. [PMID 12530939]
- Bataller R, Gines P, Nicolas JM, Gorbig MN, Garcia Ramealo E, Gasull X, et al. Angiotensin II induces contraction and proliferation of human hepatic stellate cells. Gastroenterology 2000; 118:1149-56. [PMID 10833490]
- Marshall RP, McAnulty RJ, Laurent GJ. Angiotensin II is mitogenic for human lung fibroblasts via activation of the type 1 receptor. Am J RespirCrit Care Med 2000; 161:1999-2004. [PMID 10852780]
- Rigat B, Hubert C, Alhenc-Gelas F, Corvol P, Soubrier F. An insertion/ deletion polymorphism in angiotensin converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Invest 1990; 86:1343-6. [PMID 1976655]
- Cambien F, Poirier O, Lecerf L, Evans A, Cambou JP, Arveiler D, et al. Deletion polymorphism in the gene for angiotensin converting enzyme is a potent risk factor for myocardial infarction. Nature 1992; 359:641- 4. [PMID 1328889]
- Nobiling R. The renin-angiotensin system: from the renal basis to an organ-specific subsystem in the pancreas. JOP. J Pancreas (Online) 2001; 2:9-12. [PMID 11862016]
- Leung PS, Chappell MC. A local pancreatic reninangiotensin system: endocrine and exocrine roles. Int J Biochem Cell Biol 2003; 35:838-46. [PMID 12676170]
- Chan WP, Fung ML, Nobiling R, Leung PS. Activation of local renin-angiotensin system by chronic hypoxia in rat pancreas. Mol Cell Endocrinol 2000; 160:107-14. [PMID 10715544]
- Kuno A, Yamada T, Masuda K, Ogawa K, Sogawa M, Nakamura S, et al. Angiotensin- Converting Enzyme attenuates pancreatic inflammation and fibrosis in male Bonn/Kabori rats. Gastroenterology 2003; 124:1010-9. [PMID 12671898]
- Yoshida H, Mitarai T, Kawamura T, Kitajima T, Miyazaki Y, Nagasawa R, et al. Role of deletion polymorphism of the angiotensin converting enzyme gene in the progression and therapeutic responsiveness of IgA nephropathy. J Clin Invest 1995; 96:2162-9. [PMID 7593601]
- Oparil S, Haber E. The renin-angiotensin system (first of two parts). N Engl J Med 1974; 291:389-401. [PMID 4367917]
- Matsusaka T, Hymes J, Ichikawa I. Angiotensin in progressive renal diseases: theory and practice. J Am Soc Nephrol 1996; 7:2025-43. [PMID 8915963]
- Matsusaka T, Ichikawa I. Biological functions of angiotensin and its receptors. Annu Rev Physiol 1997; 59:395-412. [PMID 9074770]
- Moriguchi Y, Matsubara H, Mori Y, Murasawa S, Masaki H, Maruyama K, et al. Angiotensin II induced transactivation of epidermal growth factor receptor regulates fibronectin and transforming growth factor beta synthesis via transcriptional and posttranscriptional mechanisms. Circ Res 1999; 84:1073-84. [PMID 10325245]
- Ioannidis JP, Trikalinos TA, Ntzani EE, Contopoulos-Ioannidis DG. Genetic associations in large versus small studies: an empirical assessment. Lancet 2003; 361:567-71. [PMID 12598142]
- Baudin B. New aspects on angiotensin converting enzyme : from gene to disease. Clin Chem Lab Med 2002; 40:256-65. [PMID 12005216]
- Leung PS Carlsson PO. Tissue renin- angiotensin system: its expression, localization, regulation and potential role in the pancreas. J Mol Endocrinol 2001; 26:155-164. [PMID 11432370]
- Leung PS, Chan HC, Nobiling R. Regulated expression of pancreatic renin angiotensin system in experimental pancreatitis. Mol Cell Endocrinol 2000; 166:121-128. [PMID 10996430]
- Ip SP, Kwan PC, Williams CH, Pang S, Hooper NM, Leung PS. Changes of angiotensin converting enzyme activity in the pancreas of chronic hypoxia and acute pancreatitis. Int J Biochem Cell Biol 2003; 35:944-54. [PMID 12676178]
- Nagashio Y, Asaumi H, Watanabe S, Nomiyama Y, Taguchi M, Tashiro M, et al. Angiotensin II type 1 receptor interaction is an important regulator for the development of pancreatic fibrosis in mice. Am J PhysiolGastrointest Liver Physiol 2004; 287:170-7. [PMID 15016612]
- O`Malley J, Maslen CL, Illingworth DR. Angiotensin converting enzyme DD genotype and cardiovascular disease in heterozygous familial hypercholesterolemia. Circulation 1998; 97:1780-3. [PMID 9603531]
- Pietinalho A, Furuya K, Yamaguchi E, Kawakami Y, Selroos O. The angiotensin converting enzyme DD gene is associated with poor prognosis in Finnish sarcoidosis patients. Eur Resp J 1999; 13:723-6. [PMID 10362030]
- Beohar N, Damaraju S, Prather A, Yu QT, Raizner A, Kleiman ND, et al. Angiotensin-I converting enzyme genotype DD is a risk factor for coronary artery disease. J Investig Med 1995; 43:275-80. [PMID 7614074]
- Navis G, van der Kleij FG, de Zeeuw D, de Jong PE. Angiotensin-converting enzyme gene I/D polymorphism and renal disease. J Mol Med 1999; 77:781-91. [PMID 10619438]
- Ohta T, Amaya K, Yi S, Kitagawa H, Kayahara M, Ninomiya I, et al. Angiotensin converting enzymeindependent, local angiotensin II-generation in human pancreatic ductal cancer tissues. Int J Oncol 2003; 23:593-8. [PMID 12888892]

