Key words
Obesity; Pancreatic Fistula; Pancreaticoduodenectomy
Abbreviations
PD: pancreaticoduodenectomy
Introduction
Obesity, whose incidence is growing at epidemic rates in the general population, has been considered a risk factor for surgical outcomes of patients undergoing abdominal surgery [1, 2, 3]. The presence of excessive fat tissue inside and outside the viscera has often increased operative times and blood losses while impairing surgical quality. Also, many authors have consistently reported a greater risk for leakage and postoperative complications in the obese population as compared to lean subjects [2, 3, 4, 5]. However, recent reports seem to challenge this long-held opinion [6, 7].
Pancreaticoduodenectomy (PD) is still considered a complex high-risk surgical procedure. Although its operative mortality is now decreased to less than 5% in highvolume institutions, its morbidity rates remain unchanged, ranging from 23 to more than 40% [8, 9]. A leading cause of this morbidity is represented by disruption of the pancreatic anastomosis, with subsequent pancreatic fistula, sepsis and hemorrhage [10, 11]. A substantial risk factor for pancreatic fistula after PD is the status of the pancreatic remnant. It has been verified that a soft pancreatic remnant without ductal dilatation is associated with a high risk of leakage [12, 13].
Performing PD in the obese patient is more challenging and hazardous. The presence of obesity impairs the surgical procedure as a result of massive fat deposition inside and outside the pancreas.
The purpose of the present study was to compare the results of PD in obese and nonobese patients and to investigate the specific impact of obesity on the technical aspects and postoperative outcome of this procedure.
PATIENTS AND METHODS
Between 1999 and 2006, among 116 consecutive patients who had had pancreaticoduodenal resection in the Department of Digestive Surgery at Hôtel- Dieu de France, 92 were included in the present study. Patients who underwent total pancreatectomy and patients who underwent PD for chronic pancreatitis were excluded. All procedures were carried out by the senior author (RN). A retrospective review of a prospectively maintained database was performed. The study population was divided into two groups (“Obese” and “Non-Obese”) according to the presence or the absence of a body mass index (BMI) value equal to or higher than 30 kg/m2.
Conventional PD was performed in all patients [14]. A pancreaticojejunostomy or pancreaticogastrostomy were performed endto- side using a single layer of Prolene® 5/0 either with the pancreatic stump cut surface (stump anastomosis) in patients with a small duct (less than 3 mm) or included the pancreatic ductal wall (ductal anastomosis) in patients with a dilated duct. Pancreatic duct stent and fibrin glue were not used. Hepaticojejunal anastomosis was performed end-to-side without stenting followed by a standard end-to-side gastrojejunostomy. In all patients, a silicone rubber closed-suction drain was placed in front of and behind the pancreatic anastomosis and the abdomen was closed with continuous sutures. Vagotomy, tubal gastrostomy or feeding jejunostomy were not performed on any patient. The majority of patients received erythromycin lactobionate as a prophylaxis for delayed gastric emptying and octreotide prophylaxis as a prophylaxis for pancreatic fistula.
After surgery, the patients were monitored in the intensive care unit and were returned to the wards at the discretion of the intensivist. Abdominal drainage fluids were stented for amylase and lipase levels when a pancreatic fistula was suspected. A routine abdominal CT scan was carried out at day 7 or on any patient with a suspected infected collection. All fluid collections were drained percutaneously with amylase dosage and bacteriologic cultures.
The main endpoints assessed were in-hospital mortality and morbidity rates, intraoperative data, incidence, nature and number of postoperative complications, and the length of hospital stay. Pancreatic fistula was defined as any measurable drainage (from an operatively placed drain or a subsequently placed percutaneous drain) having an amylase content greater than 3 times the upper limit of the reference serum amylase level requiring specific management (grade B and C fistulas according to the International Study Group on pancreatic fistula [15]). Surgical pathology specimens from the pancreatic neck of the obese group were studied further for the amount of intrapancreatic fat, and were graded from absent to massive on a 4-point pancreatic fat scale: 0-absent, 1-normal, 2- high, 3-massive.
ETHICS
The study was approved by the Ethics and Research Committee of the Hôtel-Dieu de France Hospital, Beirut, Lebanon. Oral informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the Declaration of Helsinki.
STATISTICS
All data and statistical procedures were carried out using the SPSS version 14.0 for Windows statistical package (SPSS Inc., Chicago, IL, USA). Results are reported as mean±SD and range or as frequencies, as appropriate. Statistical analysis was conducted by using the Fisher’s exact and the linear-by-linear association tests for qualitative variables, the ANOVA for the comparison of means, and the Spearman rank for testing correlations. Two-tailed P values less than 0.05 were considered to be significant.
RESULTS
Population Characteristics
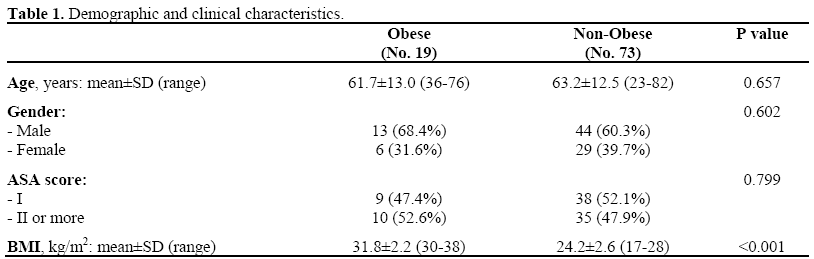
The study population included 92 patients with a mean age of 62.9±12.5 years (range: 23-82 years). There were 57 (62.0%) men and 35 (38.0%) women. Forty-seven (51%) patients were classified as American Society of Anesthesiology (ASA) score I. The Obese Group included 19 (20.7%) patients and the Non-Obese Group included 73 (79.3%) patients. The BMI was 31.8±2.2 kg/m2 (range: 30-38 kg/m2) vs. 24.2±2.6 kg/m2 (range: 17-28 kg/m2) in the Obese and Non- Obese groups, respectively (P<0.001). As shown in Table 1, the two groups were comparable in terms of demographics and ASA score.
Intraoperative Course
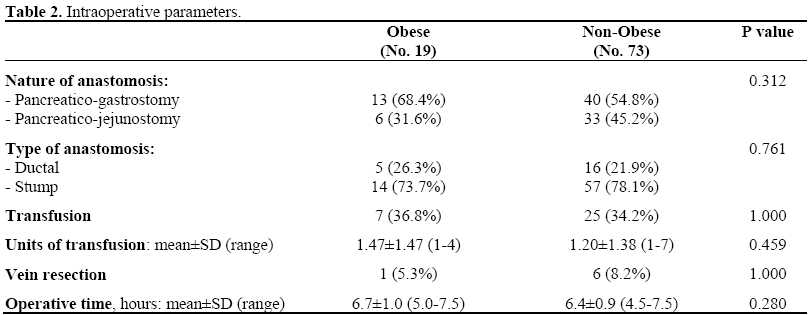
Pancreatico-gastrostomy was performed in 53 (57.6%) patients and pancreatico-jejunostomy in 39 (42.4%) patients. A pancreaticodigestive anastomosis was performed with the pancreatic stump cut surface in 71 (77.2%) and included the pancreatic ductal wall in 21 (22.8%). The intraoperative parameters of the two groups are listed in Table 2. The two groups were comparable according to the nature and type of pancreatico-digestive anastomosis. Sixty patients (65.2%) did not require a blood transfusion during surgery while the remaining 32 (34.8%) received blood transfusions with a mean of 1.26±1.38 units of red blood cells. Seven (7.6%) patients underwent resection of portions of either the portal vein or the superior mesenteric vein. Although the operating time was longer in the Obese Group (6.7±1.0 h) than in the Non- Obese Group (6.4±0.9 h), the difference did not reach the statistical significance (P=0.280).
Postoperative Course
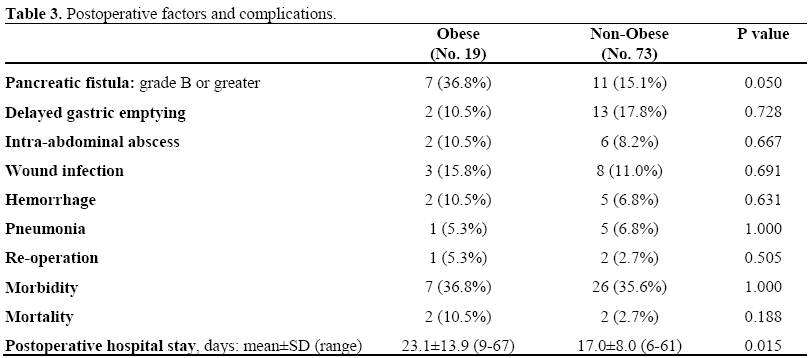
There were 4 postoperative deaths, 2 in each group for an in-hospital mortality rate of 4.3%. The cause of death was sepsis in the setting of pancreatic fistula in two patients of the Obese Group, a myocardial infarction and a death resulting from a catastrophic scenario following percutaneous biliary drainage in the Non-Obese Group.
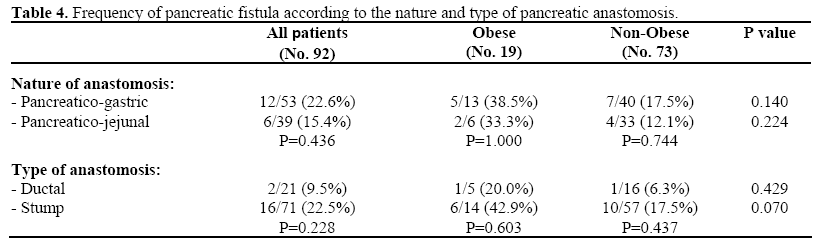
Thirty three (35.9%) patients developed a postoperative complication (Table 3). The overall rate of clinically relevant pancreatic fistula was 36.8% in the Obese Group and 15.1% in the Non-Obese Group (P=0.050). Analysis of the incidence of pancreatic fistula revealed that it was not significantly influenced by the nature (pancreaticogastrostomy vs. pancreaticojejunostomy) and the type (ductal vs. stump) of pancreatic anastomosis in all patients and within each of the two groups (Table 4). The incidence of the other postoperative complications was not significantly different between the two groups (Table 3). Seven (7.6%) patients presented postoperative hemorrhage (2 in the Obese group and 5 in the Non-Obese group). Three were re-operated on, including hemostasis of a bleeding artery of the pancreatic capsule in one obese patient, and completion pancreatectomy in two non-obese patients (one for early pancreatic anastomotic bleeding and one for a bleeding pseudoaneurysm of the gastroduodenal arterial stump in the setting of pancreatic fistula). Two patients necessitated embolization of the hepatic artery, the first (obese) for a bleeding pseudoaneurysm of the gastroduodenal arterial stump in the setting of pancreatic fistula which resulted in biliary ischemia, and the second (non-obese), who is included in the 4 in-hospital deaths, for uncontrollable hemobilia from a percutaneous transhepatic biliary drain which resulted in acute liver necrosis and death. The remaining 2 non-obese patients responded to conservative management. All the reoperations were performed for bleeding. The mean length of hospital stay was significantly longer (P=0.015) in the Obese Group (23.1±13.9 days; range: 9-67 days) as compared with the Non-Obese Group (17.0±8.0 days; range: 6-61 days).
The final pathologic diagnoses of the resected specimens revealed periampullary adenocarcinoma in 13 (68.4%) patients of the Obese Group and in 52 (71.2%) patients of the Non-Obese Group (P=0.785). Surgical pathology specimens from the pancreatic neck of the Obese group showed that the amount of intrapancreatic fat was increased in 10 patients (52.6%; pancreatic fat scale equal to 2 or 3) and correlated positively both with BMI (P=0.001; Figure 1) and with the occurrence of pancreatic fistula (P=0.003; Figure 2).
Figure 1. Correlation between BMI and intrapancreatic
fat graded from absent to massive on a four-point scale
(Spearman rank correlation test).
Figure 2. Correlation between the occurrence of
pancreatic fistula and intrapancreatic fat graded from
absent to massive on a four-point scale (linear-bylinear
association test).
DISCUSSION
Johns Hopkins Hospital, as well as other high-volume centers worldwide, have reported a substantial decrease in hospital mortality for PD, about 5% or lower [8, 9, 16, 17]. In addition to careful patient selection, improved surgical technique and improvements in perioperative care, the highvolume of PD made have contributed to this drop. The current series was performed in a tertiary care and academic institution having the aforementioned prerequisites and resulted in an operative mortality rate which is in accordance with experienced centers. During the last 5 years, the annual caseload has increased to more than 15 resections which might have contributed in part to the improved outcome. Furthermore, because of the high volume, intraoperative mishaps were not encountered, and operative time and blood administration were comparable to other series.
Despite a substantial drop in mortality after PD, the morbidity rates remained unchanged ranging from 23 to more than 40% and were led by the occurrence of a pancreatic fistula [8, 9, 16, 17, 18, 19]. It has repeatedly been demonstrated that both soft pancreatic remnant texture and small duct size are major risk factors for pancreatic fistula [12, 13]. Although, obesity was recently identified as an additional risk factor for leakage after distal pancreatectomy, the current study highlights the increased risk after PD [20]. Our results demonstrated that the presence of obesity more than doubled the risk of pancreatic fistula after PD despite a standardized technique which was performed by the same surgeon.
Obesity seems to affect both the texture of the pancreatic remnant and the quality of pancreatic anastomosis construction. It is well known that, in almost every individual, there is a variable amount of intrapancreatic fat which varies from 3 to 20%, according to the nutritional state [21]. Our results demonstrated that the amount of intrapancreatic fat was increased in 50% of our obese patients and that this increase correlated positively with BMI. As illustrated in Figure 3, fat infiltration of the pancreatic remnant makes it prone to laceration during suturing or tying. In addition, the presence of a bulky pancreatic remnant with obscure demarcation in a deep operating field would affect technical precision in anastomosis construction which are essential factors for the prevention of pancreatic fistula.
Figure 3. Typical histological specimen of the
pancreatic neck cut surface showing massive
intrapancreatic fat deposition (H&E, x4).
The impact of obesity on the technical difficulty of many abdominal procedures has previously been reported and has translated into longer operating times and increased blood losses than in lean subjects [5, 22]. In this study, we have noted that, in the obese patients, some stages of the procedure were more laborious, particularly transection of the mesentery of the first jejunal loop, complete excision of the retroportal pancreatic process as well as complete dissection of the right side of the superior mesenteric artery and of the portal vein. However, intraoperative difficulty has not significantly altered intraoperative parameters (blood transfusions and operating time) in the obese group. This is probably related to the fact that except for one mesentericoportal venous reconstruction, all were performed in the non-obese group. No one can ignore the fact that blood transfusions and operating time are increased in patients undergoing PD with venous reconstruction [23, 24].
Pancreatic fistula is the factor most strongly linked with death in the majority of case series and remains the leading cause of morbidity after PD [9, 25]. Analysis of the cause of mortality in the current series revealed that pancreatic fistula was responsible of one-half (2/4) of the deaths. In addition, pancreatic fistula resulted in two life-threatening bleeding pseudoaneurysms which are known to result from sepsis in the pancreatic bed [26, 27, 28]. According to our results, the pancreatic surgeon, while performing PD in an obese patient, must be prepared for an increased risk of anastomotic leak and for subsequent, often lethal, hemorrhage. Like others, we advocate trying to avoid vascular injuries during lymphadenectomy, meticulous anastomosis, wrapping of the dissected vessels and adequate abdominal drainage [27]. We also anticipate the problems related to interrupting the hepatic arterial flow after PD where its consequences may be disastrous as we observed in two of our patients [28, 29]. We therefore recommend a gastroduodenal arterial stump of at least 1 cm in length in order to enable safe microcoil embolization in the case of bleeding from the arterial stump. Postoperatively, percutaneous placement of a covered stent in the hepatic artery can arrest pseudoaneurysm bleeding while preserving common hepatic artery patency [30, 31].
The effects of obesity on surgical outcome after major abdominal surgery are becoming an increasingly relevant issue given the growing rate of obesity worldwide. In the current series, 19 out of 92 patients (21%) undergoing PD were obese (i.e., a BMI equal to or greater than 30 kg/m2). Obesity is known to affect surgical outcome through both procedure-related and general complications. In the present study, in addition to the increased risk of pancreatic fistula which lengthened the hospital stay in obese patients, one unexpected result was the same trend for general complications when compared to nonobese patients. Because the majority of obese patients were mildly obese (17 out of 19 patients had a BMI ranging from 30.0 to 34.9 kg/m2), associated comorbidity conditions such as cardiovascular disease, pulmonary dysfunction and diabetes were infrequent as reflected by the comparable ASA scores. Like others, we believe that obesity alone is not a risk factor for postoperative general complications [7, 32]. Rather, their likelihood seems more related to ASA score. In addition, we believe that mild obesity without associated comorbidities is relatively protective for patients undergoing PD for malignancy owing to relatively preserved nutritional and immunological status.
CONCLUSION
The current single-institution retrospective study showed that obese patients are at increased risk for developing pancreatic fistula after PD. Special surgical caution as well as vigilant postoperative monitoring are therefore recommended when performing PD in obese patients.
Conflict of interest
The authors have no potential conflicts of interest
References
- National Institute of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. 1998: (Update Planned). National Heart, Lung, and Blood Institute (NHLBI) Expert Panel Publication.
- Eichenberger A, Proietti S, Wicky S, Frascarolo P, Suter M, Spahn DR, Magnusson L. Morbid obesity and postoperative pulmonary atelectasis: an underestimated problem. AnesthAnalg 2002; 95:1788-92. [PMID 12456460]
- Benoist S, Panis Y, Alves A, Valleur P. Impact of obesity on surgical outcomes after colorectal resection. Am J Surg 2000; 179:275-81. [PMID 10875985]
- Kodera Y, Sasako M, Yamamoto S, Sano T, Nashimoto A, Kurita A; Gastric Cancer Surgery Study Group of Japan Clinical Oncology Group. Identification of risk factors for the development of complications following extended and superextended lymphadenectomies for gastric cancer. Br J Surg 2005; 92:1103-9. [PMID 16106493]
- Tsujinaka T, Sasako M, Yamamoto S, Sano T, Kurokawa Y, Nashimoto A, et al. Influence of overweight on surgical complications for gastric cancer: results from a randomized control trial comparing D2 and extended para-aortic D3 lymphadenectomy (JCOG9501). Ann Surg Oncol 2007; 14:355-61. [PMID 17146738]
- Scipione CN, Chang AC, Pickens A, Lau CL, Orringer MB. Transhiatalesophagectomy in the profoundly obese: implications and experience. Ann ThoracSurg 2007; 84:376-82. [PMID 17643603]
- Dindo D, Muller MK, Weber M, Clavien PA. Obesity in general elective surgery. Lancet 2003; 361:2032-5. [PMID 12814714]
- Gordon TA, Bowman HM, Tielsch JM, Bass EB, Burleyson GP, Cameron JL. Statewide regionalization of pancreaticoduodenectomy and its effect on inhospital mortality. Ann Surg 1998; 228:71-8. [PMID 9671069]
- Gouma DJ, van Geenen RC, van Gulik TM, de Haan RJ, de Wit LT, Busch OR, Obertop H. Rates of complications and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg 2000; 232:786-95. [PMID 11088073]
- Yeo CJ, Cameron JL, Maher MM, Sauter PK, Zahurak ML, Talamini MA, et al. A prospective randomized trial of pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy. Ann Surg 1995; 222:580- 92. [PMID 7574936]
- Yeo CJ, Cameron JL, Lillemoe KD, Sauter PK, Coleman J, Sohn TA, et al. Does prophylactic octreotide decrease the rates of pancreatic fistula and other complications after pancreaticoduodenectomy? Results of a prospective randomized placebo-controlled trial. Ann Surg 2000; 232:419-29. [PMID 10973392]
- Marcus SG, Cohen H, Ranson JH. Optimal management of the pancreatic remnant after pancreaticoduodenectomy. Ann Surg 1995; 221:635- 45. [PMID 7794068]
- Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol 2005; 11:2456-61. [PMID 15832417]
- Evans DB, Lee JE, Pisters PWT. Pancreaticoduodenectomy (Whipple Operation) and total pancreatectomy for cancer. In: Baker RJ, Fischer JE, Ed Mastery of Surgery, 4th Ed. New York: Lippincott Williams and Wilkins, 2001:1299-1318. [ISBN 0-7817-2328-0]
- Liang TB, Bai XL, Zheng SS. Pancreatic fistula after pancreaticoduodenectomy: diagnosed according to International Study Group Pancreatic Fistula (ISGPF) definition. Pancreatology 2007; 7:325-31. [PMID 17627097]
- Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006; 244:10-5. [PMID 16794383]
- Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J GastrointestSurg 2006; 10:1199-210. [PMID 17114007]
- DeOliveira ML, Winter JM, Schafer M, Cunningham SC, Cameron JL, Yeo CJ, Clavien PA. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann Surg 2006; 244:931-7. [PMID 17122618]
- Topal B, Aerts R, Hendrickx T, Fieuws S, Penninckx F. Determinants of complications in pancreaticoduodenectomy. Eur J Surg Oncol 2007; 33:488-92. [PMID 17145159]
- Sledzianowski JF, Duffas JP, Muscari F, Suc B, Fourtanier F. Risk factors for mortality and intraabdominal morbidity after distal pancreatectomy. Surgery 2005; 132:180-5. [PMID 15674199]
- Klimstra DS. Pancreas. In: Sternberg SS, Ed. Histology for Pathologist, 2nd Ed. Philadelphia, PA, USA: Lippincott Williams & Wilkins, 1997:613-47. [ISBN 0-3975-1718-1]
- Hawn MT, Bian J, Leeth RR, Ritchie G, Allen N, Bland KI, Vickers SM. Impact of obesity on resource utilization for general surgical procedures. Ann Surg 2005; 241:821-6. [PMID 15849518]
- Carrère N, Sauvanet A, Goere D, Kianmanesh R, Vullierme MP, Couvelard A, et al. Pancreaticoduodenectomy with mesentericoportal vein resection for adenocarcinoma of the pancreatic head. World J Surg 2006; 30:1526-35. [PMID 16855797]
- Ohwada S, Hamada K, Kawate S, Sunose Y, Tomizawa N, Yamada T, et al. Left renal vein graft for vascular reconstruction in abdominal malignancy. World J Surg 2007; 31:1215-20. [PMID 17453283]
- van Berge Henegouwen MI, De Wit LT, Van Gulik TM, Obertop H, Gouma DJ. Incidence, risk factors, and treatment of pancreatic leakage after pancreaticoduodenectomy: drainage versus resection of the pancreatic remnant. J Am CollSurg 1997; 185:18- 24. [PMID 9208956]
- Turrini O, Moutardier V, Guiramand J, Lelong B, Bories E, Sannini A, et al. Hemorrhage after duodenopancreatectomy: impact of neoadjuvantradiochemotherapy and experience with sentinel bleeding. World J Surg 2005; 29:212-6. [PMID 15654661]
- Maeda A, Ebata T, Kanemoto H, Matsunaga K, Bando E, Yamaguchi S, Uesaka K. Omental flap in pancreaticoduodenectomy for protection of splanchnic vessels. World J Surg 2005; 29:1122-6. [PMID 16132400]
- Noun R, Zeidan S, Tohme-Noun C, Smayra T, Sayegh R. Biliary ischemia following embolization of a pseudoaneurysm after pancreaticoduodenectomy. JOP. J Pancreas (Online) 2006; 7:427-3. [PMID 16832142]
- Tajima Y, Kuroki T, Tsutsumi R, Sakamoto I, Uetani M, Kanematsu T. Extrahepatic collaterals and liver damage in embolotherapy for ruptured hepatic artery pseudoaneurysm following hepatobiliary pancreatic surgery. World J Gastroenterol 2007; 13:408-13. [PMID 17230610]
- Kostro J, Zapasnik A, Siondalski P, Sledzinski Z. Hemorrhage from ruptured hepatic artery pseudoaneurysm co-occurring with pancreatic head tumor and portal vein thrombosis: surgical and endovascular treatment. SurgLaparoscEndoscPercutan Tech 2005; 15:256-8. [PMID 16082320]
- Maleux G, Pirenne J, Aerts R, Nevens F. Case report: hepatic artery pseudoaneurysm after liver transplantation: definitive treatment with a stent-graft after failed coil embolisation. Br J Radiol 2005; 78:453-6. [PMID 15845944]
- Casadei R, Zanini N, Morselli-Labate AM, Calculli L, Pezzilli R, Potì O, et al. Prognostic factors in periampullary and pancreatic tumor resection in elderly patients. World J Surg 2006; 30:1992-2001. [PMID 16957825]




