Keywords
Nomograms; Pancreatitis; Predictive Value of Tests
INTRODUCTION
Acute pancreatitis (AP) is usually a self-limiting process, however 25% present with severe acute pancreatitis (SAP) which has an associated mortality of up to 50% [1]. Prognostic scoring systems have been developed to identify patients at risk of developing SAP as these patients benefit from early intensive resuscitation as this leads to improved survival [2].
Traditional scoring systems such as the Imrie (Glasgow) score that depend on assessment of haematological and biochemical factors, and whilst easy to calculate, often only provide prognostic information 48 hours following admission. The Acute Physiology and Chronic Health Evaluation (APACHE II), which is often used as the standard comparator for prognostication, is cumbersome, not easily repeatable, and has a positive predictive value (PPV) of only 65-70% [3, 4]. Furthermore, the need for multiple serum measurements means that it is too slow to reflect rapid changes in SIRS and MODS thus reducing prognostic accuracy.
The poor prognosis in severe pancreatitis is due to a Systemic Inflammatory Response Syndrome (SIRS) response and Multi-Organ Dysfunction Syndrome (MODS) [5-8]. Newer scoring systems such as SOFA (Sequential Organ Failure Assessment) which reflect SIRS/MODS have been developed but these are best performed in the intensive care setting, and not suitable for routine use in all patients with pancreatitis [9].
A scoring system using bedside measurements (Early Warning Score, EWS) was developed in 2001 and initially evaluated in medical admissions and critically unwell patients [10]. EWS is calculated using hourly measurements of 6 bedside parameters (pulse, respiratory rate, temperature, conscious level, urine output and blood pressure) to provide a score of 0-20. The EWS has been evaluated and validated in AP and shown to provide comparable accuracy to APACHE II and Ranson scores [11, 12].
The Modified Early Warning Scores (MEWS), an amendment to the EWS, assesses 8 parameters including the 6 parameters used in EWS, and in addition, oxygen saturation and requirement for respiratory support requirement but does so on a less frequent basis, with 6-hourly recordings. Whilst the value of the EWS score has been examined in AP, the role of MEWS in predicting SAP has yet to be determined.
The objective of this study was to determine the accuracy of MEWS in predicting poor outcome in acute pancreatitis, and assess the optimal mode of using MEWS scores for this purpose.
METHODS
Sequential patients admitted with acute pancreatitis to our institution during the period January to December 2010 were included. All such patients were entered into a prospectively maintained AP database. AP was defined as elevation two of the following three features: (1) abdominal pain consistent with acute pancreatitis (acute onset of a persistent, severe, epigastric pain often radiating to the back); (2) serum lipase activity (or amylase activity) at least three times greater than the upper limit of normal; and (3) characteristic findings of acute pancreatitis on contrast-enhanced computed tomography (CECT) and less commonly magnetic resonance imaging (MRI) or transabdominal ultrasonography as per Atlanta classification. Patients were classified as mild or severe acute pancreatitis (SAP) as per the Atlanta classification [13]. MEWS were performed on admission and 6-hourly thereafter using 8 scored bedside measurements (Table 1 & Figure 1).
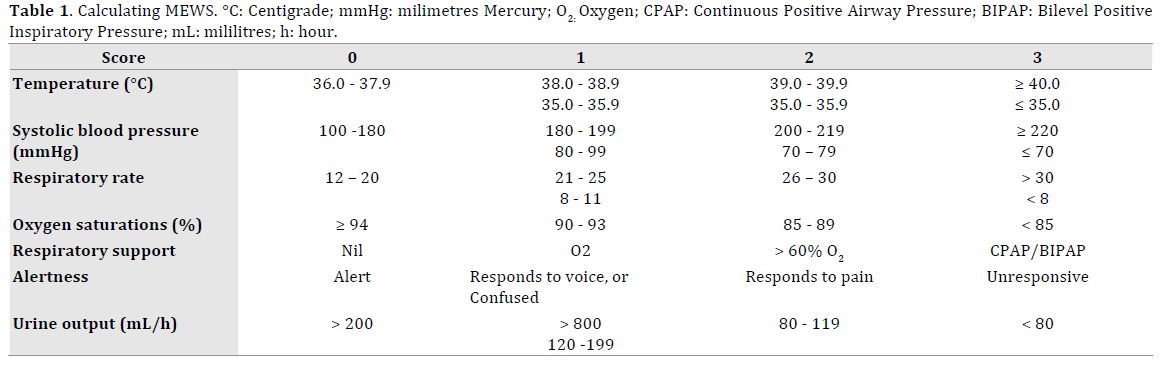
Figure 1. A MEWS chart as used in the study, illustrating the colour coding and points system utilized in generating a score.
The MEWS chart provides a recommended action depending on the cumulative score: MEWS = 3 - 4 requires 2-hourly observation plus junior medical review within 30 minutes; MEWS ≥5, or any single parameter scores ≥ 3; or total MEWS increases by ≥3 within 30 minutes requires senior medical opinion together with critical care outreach review.
STATISTICS
Sensitivity, specificity, negative NPV and PPV were calculated for the highest MEWS (hMEWS) in a 24-hour period and mean daily MEWS (mMEWS). The chi-squared test was used for categorical data, and the Student’s t-test for continuous data. Receiving operator characteristics (ROC) curves were generated with corresponding area under the curve (AUC) measurements and 95% confidence intervals (CI) calculations. ROC analysis provided optimal cut-off points to allow tradeoff between true positive and true negative rates.
SPSS (Statistical Package for Social Sciences, version 18; SPSS Inc, Chicago, Illinois, USA) was used to carry out the analyses. A p-value of < 0.05 was taken to indicate statistical significance.
RESULTS
One forty six-146 patients were admitted with acute pancreatitis with 4 excluded from the analysis due to incomplete data. Mean patient age was 56 years (Standard deviation, SD ± 20 years) with an equal gender distribution: 72 were male and 70 were female. The aetiology of pancreatitis was gallstones (89), alcohol (30), ERCP (3), cancer (1), benign stricture (1), hypercalcaemia (1), idiopathic (11), mixed gallstone and/or alcohol and /or drug-induced (5) pancreas divisum (1). 120 were classified as mild, and 22 were classified as SAP. There was no significant difference between mild and SAP groups for: age (54.8 years versus 63 years, p = 0.076); male gender (49% versus 59%) or aetiology. Renal and hepatic function tests were comparable as were blood glucose levels.
ROC analysis suggested a hMEWS > 2.5 per 24-hour period was the most accurate in predicting poor prognosis (AUC 0.924, 95% CI: 0.849 – 0.998). As MEWS= 2.5 is not possible given the whole number nature of MEWS scoring, the highest MEWS ≥ 3 in a 24-hour period was used as this was more accurate than MEWS ≥2 (Table 2).
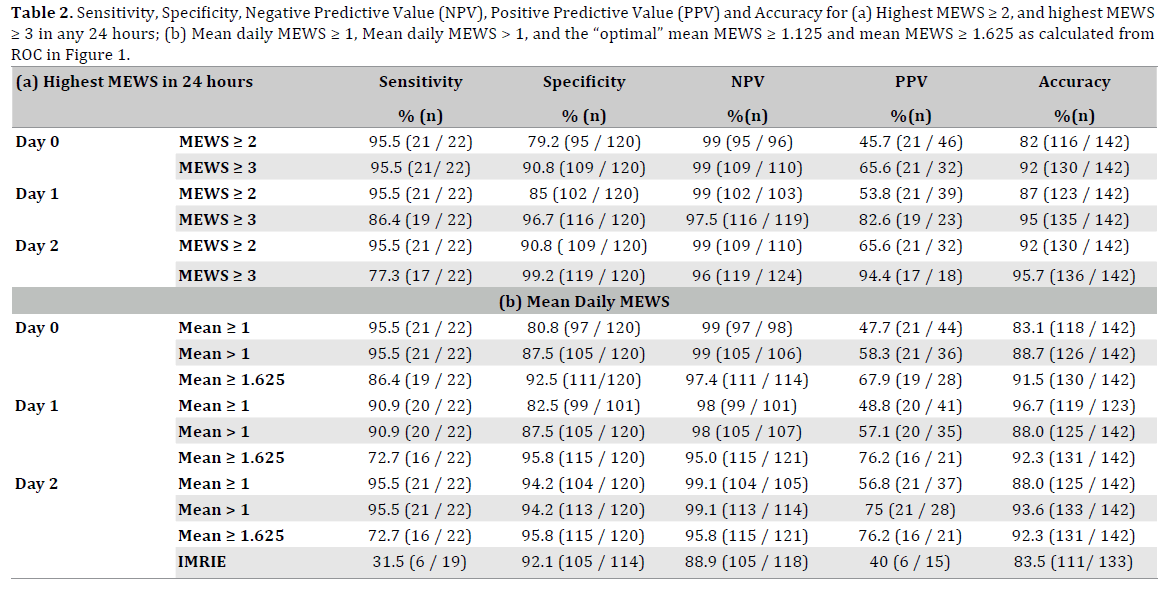
Furthermore, ROC analysis suggested an optimal mMEWS of 1.625 (Figure 2). The sensitivity, specificity, NPV, PPV and accuracy of each hMEWS and mMEWS is illustrated in Table 2. Daily hMEWS and mMEWS were higher in the SAP group on all 3 days. Six (4.2%) patients died, all with evidence of SAP. Causes of death included: cholangitis (n=1); pneumonia on background of extensive chronic airways disease (n=1); pancreatic necrosis with cardiac failure (n=1); psoas abscess (n=1); and MODS (n=2). The first 4 patients recorded first MEWS ≥3 on Day 0 and mMEWS >1 on Day 0. Of the remaining 2, the first patient had low hMEWS and mMEWS (Day 0, 1, 2) initially but developed pneumonia on Day 4 and rapidly deteriorated; the second patient had borderline MEWS (hMEWS = 2 and mMEWS = 0.5) on admission and also deteriorated rapidly with acute respiratory distress syndrome on day 3 that progressed to MODS.
Figure 2. Receiver Operator Characteristics (ROC) curve for mean MEWS on Day 1
(Mean 1), mean MEWS on Day 2
(Mean 2) and mean MEWS on Day 3
(Mean 3); AUC: Area Under Curve; SE: Standard Error; CI: Confidence Interval.
DISCUSSION
The primary finding of the study was that the MEWS was a reliable prognostic indicator allowing early identification of patients likely to develop SAP. In addition, the fact that it is easy to perform, instant, and dymamic, with a superior statistical profile to the Imrie score would indicate that this physiological score could replace the traditional serum- based means of assessment.
The MEWS, which is performed at the bedside, is potentially more accurate as it as it reflects a persistent SIRS response despite resuscitation that in turn, is a predictor of MODS. It is well documented that a persistent SIRS at 6 hours or the development of MODS and hypotension despite fluid resuscitation are equivalent if not stronger predictors of mortality than other physiological, haematological and biochemical variables used in alternative scoring systems [14-23] (Table 3). The frequency of MEWS, which is a minimum of 6-hourly, may also anticipate deterioration sooner than other scoring systems that are performed daily, or on admission and at 48 hours.
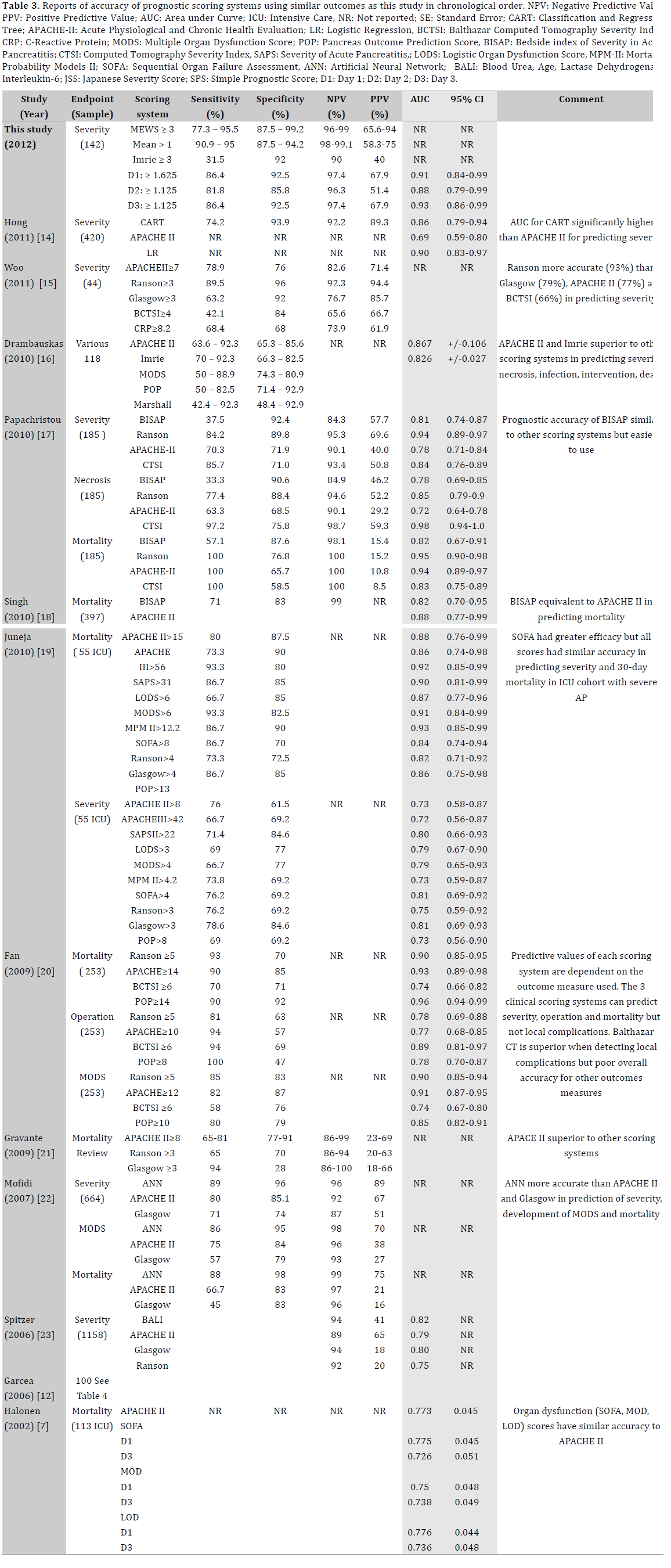
The MEWS has not previously been reported in relation to prognostication of severity in AP. We determined the optimal cut-off value using ROC analysis and this suggested an optimal hMEWS of 2.5 and mMEWS of 1.625. As MEWS scores are whole numbers, repeat analysis indicated a hMEWS (≥3) would be optimal. The severity prediction of hMEWS ≥3 at admission was comparable to that of scoring systems in previous studies (Table 3). Furthermore, the accuracy of hMEWS increased from day 0-2 as expected since a persistently high MEWS would reflect persistent SIRS, and hence be associated with a population with greater probability of developing SAP. When considering the recommended mMEWS >1.625, this had a high accuracy but was compromised by a lower sensitivity of 86%, that decreased over 72 hours to 70%, in the current series. This sensitivity was considered too low, and is a common weakness of most scoring system. We therefore chose a mMEWS > 1 which had a reasonable accuracy compared to a mMEWS ≥1.625 but with a much higher sensitivity of 90-95%, and also did not deteriorate over 72 hours (Table 2) .
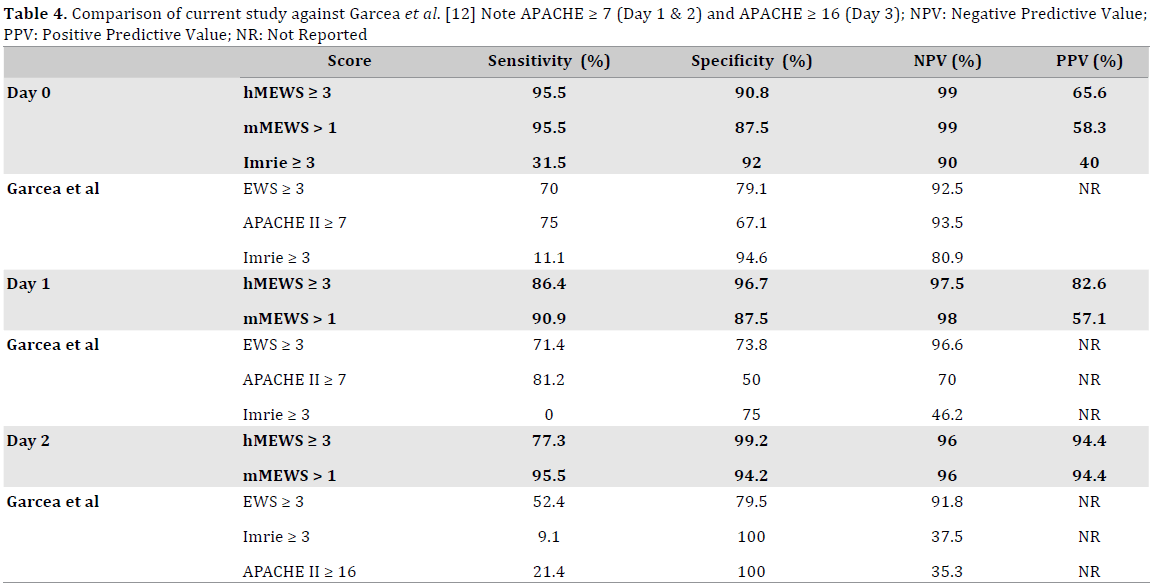
The accuracy of hMEWS ≥3 or mMEWS >1 compares favourably with APACHE-II in terms of sensitivity (70- 80%), specificity (62-76%), NPV (82-90%) and PPV (40- 71%) [1, 19]. Several studies have demonstrated that an increase in NPV is often accompanied by a corresponding decrease in PPV. For APACHE-II, it has been shown that the NPV can be increased to 92% by modifying cut-off scores, however this leads to a decrease in PPV to 67% [22, 24]. Similar or lower PPV values are seen with Imrie and Ranson scores (Table 3) with PPV occasionally as low as 18-60% [21], which again favours MEWS. As mentioned previously, the predictive values of hMEWS and mMEWS also increase during the course of the hospital stay, and this most likely reflects the ongoing physiological stress and progressive SIRS which are not always seen early on biochemical screens. The only other bedside scoring system, the EWS, has not been directly compared to MEWS in the setting of AP, however, comparison with existing studies would suggest comparable accuracies, with MEWS being less labour intensive [11, 12] (Table 4).
The MEWS failed to predict SAP in 3/22 patients. One patient had a stable pancreatico-pleural fistula and the second died from cholangitis and renal failure. The third patient was clinically well with a low MEWS until day 5 when a sudden increase in MEWS corresponded with the identification of a psoas abscess on a CT scan. He underwent laparoscopic drainage but died from sepsis soon after. The first patient (pancreatico-pleural fistula) and third patient (psoas abscess) had Imrie scores <3 and would not have been diagnosed as SAP using other physiological scoring systems although the third patient may have been diagnosed with psoas abscess earlier using CT scoring systems. The second patient with cholangitis was haemofiltrated but the MEWS does not have a separate consideration for dealing with dialysis/filtration patients, and urine output had been labeled as adequate based on filtration outputs.
Conversely, MEWS was high in 5.8% (7/120) patients with mild pancreatitis. This elevated MEWS was due to ongoing infection (4 biliary, 1 respiratory), not SIRS, but this did not fulfill Atlanta definition of organ failure. The remaining 2 patients with gallstone pancreatitis scored highly due to a persistent tachycardia without further complications. hMEWS and mMEWS each independently predicted mortality in 67% (4/6) but did not predict deterioration of pneumonia on admission, and could not predict pneumonia in the remaining patients who only developed clinical signs on day 4. As such, a raised MEWS should not be considered always a progression of pancreatitis alone, but equally a marker of other disease development, especially in a nonspecialised general medical setting.
It is important to consider other new scoring systems have been developed to overcome complicated traditional scoring systems such as the APACHE II. These include: Pancreatitis Outcome Prediction (POP) [25]; Multiple Organ Dysfunction Score (MODS) [26]; Logistic Organ Dysfunction Score (LODS) [27]; Sequential Organ Failure Assessment (SOFA) [9]; and Bedside Index for Severity in acute Pancreatitis (BISAP)[17]. These scores have been reported to be equivalent to APACHE II in predicting mortality in the ICU setting [19, 24, 28]. However, they are labour-intensive and more suited for the high dependency setting, as they are less frequently repeatable, and hence not always suitable for monitoring fluctuating disease. As such, they may be useful for those with proven SAP but not as a prognostic screening tool.
MEWS is suitable for all pancreatitis patients as a routine screening tool on a general surgical ward and can easily be reassessed to reflect changes in clinical course, identifying problems sooner than other methodologies. Resource allocation is also an important consideration. Many of the scoring systems require intensive investigations including haematological, biochemical and radiological. The MEWS is simply dependent on basic physiological assessments and incurs no additional costs.
CONCLUSION
This is the first report on the novel use of MEWS as a prognostic indicator in patients referred with AP. It is inexpensive, accessible, and less invasive than any other scoring system used in AP. The predictive values of MEWS in this study is comparable to that published by other study scoring systems but MEWS is easier to perform and more generally applicable. Further studies are required to validate these findings.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Papachristou GI, Clermont G, Sharma A, Yadav D, Whitcomb DC. Risk
and markers of severe acute pancreatitis. Gastroenterol Clin North Am
2007; 36: 277-296. [PMID: 17533079]
- Harrison DA, D'Amico G, Singer M. Case mix, outcome, and activity
for admissions to UK critical care units with severe acute pancreatitis:
a secondary analysis of the ICNARC Case Mix Programme Database. Crit
Care 2007; 11: S1. [PMID: 18275590]
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a
severity of disease classification system. Crit Care Med 1985; 13: 818-
829. [PMID: 3928249]
- Pavlidis TE, Pavlidis ET, Sakantamis AK. Advances in prognostic
factors in acute pancreatitis: a mini-review. Hepatobiliary Pancreat Dis
Int 2010; 9: 482-486. [PMID: 20943456]
- Bhatia M. Acute pancreatitis as a model of SIRS. Front Biosci
(Landmark Ed) 2009; 14: 2042-2050. [PMID: 19273184]
- Blum T, Maisonneuve P, Lowenfels AB, Lankisch PG. Fatal outcome
in acute pancreatitis: its occurrence and early prediction. Pancreatology
2001; 1: 237-241. [PMID: 12120201]
- Halonen KI, Pettilä V, Leppäniemi AK, Kemppainen EA, Puolakkainen
PA, et al. Multiple organ dysfunction associated with severe acute
pancreatitis. Crit Care Med 2002; 30: 1274-1279. [PMID: 12072681]
- Mofidi R, Duff MD, Wigmore SJ, Madhavan KK, Garden OJ, et al.
Association between early systemic inflammatory response, severity of
multiorgan dysfunction and death in acute pancreatitis. Br J Surg 2006;
93: 738-744. [PMID: 16671062]
- Minne L, Abu-Hanna A, de Jonge E. Evaluation of SOFA-based models
for predicting mortality in the ICU: A systematic review. Crit Care 2008;
12: R161. [PMID: 19091120]
- Rees JE. Early warning scores. World Anaesth 2003; 17: 1-5
- Garcea G, Gouda M, Hebbes C, Ong SL, Neal CP, et al. Predictors of
severity and survival in acute pancreatitis: validation of the efficacy of
early warning scores. Pancreas 2008; 37: e54-61. [PMID: 18815539]
- Garcea G, Jackson B, Pattenden CJ, Sutton CD, Neal CP, et al. Early
warning scores predict outcome in acute pancreatitis. J Gastrointest Surg
2006; 10: 1008-1015. [PMID: 16843871]
- Bradley EL 3rd. A clinically based classification system for acute
pancreatitis. Summary of the International Symposium on Acute
Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993;
128: 586-590. [PMID: 8489394]
- Hong W, Dong L, Huang Q, Wu W, Wu J, et al. Prediction of severe acute
pancreatitis using classification and regression tree analysis. Dig Dis Sci
2011. 56: 3664-3671. [PMID: 21833749]
- Woo SM, Noh MH, Kim BG, Hsing CT, Han JS, et al. Comparison of
serum procalcitonin with Ranson, APACHE-II, Glasgow and Balthazar CT
severity index scores in predicting severity of acute pancreatitis. Korean J
Gastroenterol 2011; 58: 31-37. [PMID: 21778801]
- Dambrauskas Z, Gulbinas A, Pundzius J, Barauskas G. Value of the
different prognostic systems and biological markers for predicting
severity and progression of acute pancreatitis. Scand J Gastroenterol
2010; 45: 959-970. [PMID: 20367283]
- Papachristou GI, Muddana V, Yadav D, O'Connell M, Sanders MK, et al.
Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting
organ failure, complications, and mortality in acute pancreatitis. Am J
Gastroenterol 2010; 105: 435-441. [PMID: 19861954]
- Singh VK, Wu BU, Bollen TL, Repas K, Maurer R, et al. A prospective
evaluation of the bedside index for severity in acute pancreatitis score
in assessing mortality and intermediate markers of severity in acute
pancreatitis. Am J Gastroenterol 2009; 104: 966-971. [PMID: 19293787]
- Juneja D, Gopal PB, Ravula M. Scoring systems in acute pancreatitis:
which one to use in intensive care units? J Crit Care 2010; 25: 358. [PMID:
20149591]
- Fan JY, Huang ZW, Guo J. [Value of four scoring systems for predicting
prognosis of severe acute pancreatitis]. Zhong Xi Yi Jie He Xue Bao 7: 34-
40. [PMID: 19134455]
- Gravante G, Garcea G, Ong SL, Metcalfe MS, Berry DP, et al. Prediction
of mortality in acute pancreatitis: a systematic review of the published
evidence. Pancreatology 2009; 9: 601-614. [PMID: 19657215]
- Mofidi R, Duff MD, Madhavan KK, Garden OJ, Parks RW. Identification
of severe acute pancreatitis using an artificial neural network. Surgery
2007; 141: 59-66. [PMID: 17188168]
- Spitzer AL, Barcia AM, Schell MT, Barber A, Norman J, et al. Applying
Ockham's razor to pancreatitis prognostication: a four-variable predictive
model. Ann Surg 2006; 243: 380-388. [PMID: 16495704]
- Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, et al. The early
prediction of mortality in acute pancreatitis: a large population-based
study. Gut 2008; 57: 1698-1703. [PMID: 18519429]
- Harrison DA, D'Amico G, Singer M. The Pancreatitis Outcome
Prediction (POP) Score: a new prognostic index for patients with
severe acute pancreatitis. Crit Care Med. 2007; 35: 1703-1708. [PMID:
17522578]
- Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, et al.
Multiple organ dysfunction score: a reliable descriptor of a complex
clinical outcome. Crit Care Med 1995; 23: 1638-1652. [PMID: 7587228]
- Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology
Score (SAPS II) based on a European/North American multicenter study.
JAMA 1993; 270: 2957-2963. [PMID: 8254858]
- Mason JM, Babu BI, Bagul A, Siriwardena AK. The performance of
organ dysfunction scores for the early prediction and management of
severity in acute pancreatitis: an exploratory phase diagnostic study.
Pancreas 2010; 39: 1104-1108. [PMID: 20861697]



