Keywords
Health policies; Health professionals; Public health; Health service; Primary health care
Introduction
This literature based discussion analyses the effects of Ottawa Charter upon public health. It focuses on some of its key purpose and current state of public health and discusses its implications reducing in inequalities in health amongst populations, mainly in developed nations but also briefly analyses the implications upon developing ones. The review is not very exhaustive in its entirety therefore any judgement about public health implementation or service delivery which must be based on other extensive evidences.
Background
The need to improve public health and promote equity has been the focus of World health organisation for a long period of time. In some countries such United Kingdom, reorientation of health services to improve public health could be traced as far as 1975. A period at which the National Health Service started shifting from disease treatment oriented to health promotion and protection [1,2].
Using what was termed the “Crossman Formula” to reduce inequalities in health in UK, the key focus was allocation of funds to regional authorities based on the principles of equal access to health care based on health needs [3,4]. However, to address the potential health risks, the UK government commissioned what was specific study to analyse the extent of inequalities in health in 1980 of what became known as Black Report 1980. The report suggested that there was a large and high level of inequalities in health across the population [3,5]. Although the introduction of the National Health Service in United Kingdom in 1948 was meant to reduce such inequalities, the gap between the rich and poor appears to be increasing with significant [6]. Worldwide, the notion of ‘health care for all’ addressing social inequalities in health amongst population dates back as far as 1978, following Alma-Ata conference in primary health care [7]. There are views that conference was the foundation for Ottawa charter as its key features formed the basis for improving public health worldwide [4].
Nevertheless, it is now almost 31 years since the International Communities convened a meaningful and serious public health meeting on the 21st November 1986 in Canadian City to address actual and potential public health challenges referred to as the Ottawa Charter “a charter for action to achieve health for All by the year 2000 and beyond”. The key drivers for the conference was a need to define and adopt a robust public health strategies capable of meeting ever-changing public health needs of communities around the world [8,9]. As such, the leaders agreed to set specific target of achieving health for all by the year 2000 and beyond as a baseline. Although the main focal, point during the meeting was on industrialised nation, there was a need to ensure that developing nations as well were supported and encouraged to meet the set target, mainly to improve public health, the key foundation had already been laid down during Alma-Ata agreement [2].
Since public health goals could not be achieved without understanding key terms or references, hence health promotion was defined as health improving activities aimed at supporting or enabling population either as individual or communities to increase control over and improve their health [8,10]. This definition implies that through health promotion approach, individuals can achieve complete physical, mental and social; well-being, which is the basis for WHO’s definition of health. As DoH [11] points out, for population to realise their aspirations, satisfy their health needs and change or cope with their changing environments, they need to be healthy. Therefore, one of best way to enhancing their health is to adopt effective and realistic health public health approach.
As such, there was acknowledgement that for the leaders to achieve desired goals. However, achieving health for all is only possible if there is peace worldwide, improved shelter, better education, healthy diet, appropriate income, stable eco-system, sustainable resources, enhanced social justice and equity [8,12]”.
In addition, effective public health can only be achieved where there are appropriate public health policies supported by fair and just political commitments that encourage and support health and equity amongst all population [8]; Marmot [5]. As DoH [12] points out, although genetic factors have contributed to ill health amongst societies, it is also clear that some of the most contemporary health risks have been linked to other factors such as social, economic as well as environmental that individuals have no control over. The need to develop Ottawa charter was not only motivated by desire to enhance health of communities by world leaders but also to reduce socio-economic gap that existed amongst population with nations or between countries [13]. Hence, charter mainly focused on the ever-increasing threats from harmful products, resource depletion, unhealthy living standards as well as environmental health risks [14]. It was perceived that by focusing on these key issues, the inequalities in health could be reduced. Effective public health policies are more likely to contribute to reduced health risks associated with poor nutrition and other ill health. As such, commitment to effective health promotion and improved public health was seen as key approach to ensure that each and every country have citizens capable of fulfilling their potentials and aspirations free from burden of diseases and disabilities [15].
However, in order to achieve effective health promotion or public health capable of supporting producing and enterprising population, there are key prerequisite that must be met by any government, as such, these we set as follows: peace, shelter, education food income stable eco-system, sustainable resources, social justice and equity [5,2]. In an attempt to highlight health inequalities [5], stipulates that while significant attention has been on increasing knowledge and adoption of capitalism within most countries, there seem to be unequal distribution of resources, which have contributed to disparities amongst majority of population [1].
In his report providing an outline of new evidence on health inequalities in the European Union (EU) and the policy response at EU and national level to health inequalities since 2009, Marmot [5] states that there are significant health inequalities between and within EU member states. In terms of inequalities amongst EU, the report makes some comparison to those reported in 2006. Marmot [5], further argues that although some indicators of inequalities within EU countries appeared to have decreased, there are still significant levels of variations, with some appearing to be increasing [16].
Methodology
Literature search
In order to address identify the most relevant evidences, a search term “Ottawa charter. Inequalities in health/population” was used to locate the most relevant data, from databases such as PubMed, CINAHL and Cochrane. Further search searches were conducted using government websites such as Public Health England, National Institute for Clinical Excellence (NICE), World Health Organisation, UNESCO and UNAIDs. The databases and websites generated vast number of data, which were later analysed into detail to ascertain their relevancies to the topic area (Figure 1).
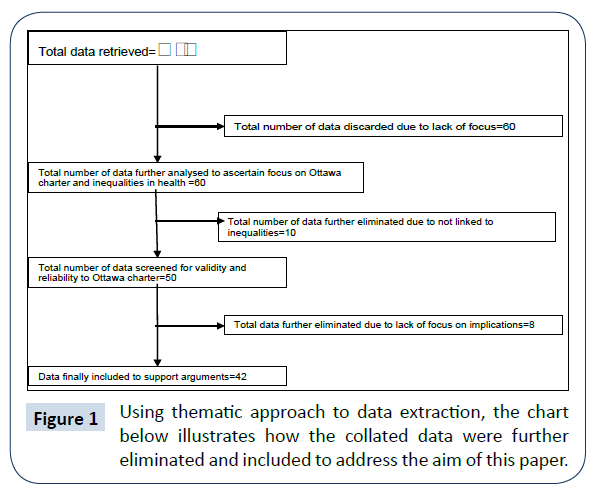
Figure 1: Using thematic approach to data extraction, the chart below illustrates how the collated data were further eliminated and included to address the aim of this paper.
Discussion
According to Marmot [5], there are indications that in 2010, socio-economic variations amongst member states of European Union (EU) have improved by 10% for women compared to 3% for men. However, the European Public Health Association (EUPHA) [17,18], argues that this could be due to enhanced or effective infant care, particular those aged 0-15 years as well as improved management of pregnancies by professionals. Evidences suggest that inequalities in particular infant mortality within EU from 2000 to 2010 improved by 26%, with significant progress for reduced mortality between 2005 to 2010, a period at which inequalities was reported to have reduced by 19% [19,20].
Despite reports of improved health status of nations in particular western Europe, in some cases there have been no significant improvement in health inequalities especially countries such as Belgium, France and Hungary. In these countries, regional inequalities have increased [21]. Whilst EUPHA [18], suggests that the Ottawa charter declaration has impacted upon public health. EUPHA [18] details that the charter has acted as catalyst for better public health outcome. EUPHA [18] further claims the Charter acknowledged the role of health promotion as basis for improving public health public health and there have been improvement in public health in areas where this has been implemented effectively. However, EUPHA [18] acknowledges that even in most countries, there are indications the charter has been either abandoned or not implemented at all. In such cases, there are clear and distinctive socio-economic gap between populations whether developed or developing countries. Similarly, DoH [22] that although there are some improvements in health, majority of world population experience inequalities in health. The key contributing factor is unfair distribution of resources. In attempt to revitalise Ottawa charter, in 2008, the World Health Organization Commission on Social Determinants of Health (CSDH) pointed out that some of the key precursor for inequalities in health include, poor living conditions, lack of power, money and resources [14,23]; since social and economic inequalities underpin determinants of health and wellbeing of population, the focus must be to eradicate the root causes of inequalities [18].
According to WHO [23], lack of focusing on social-economic as the key to improve public health by world leaders means that majority of world leaders mean that despite the Ottawa Charter, majority of the population have not experienced enhanced health status. In fact, there continues to be severe risks of ill health either due to man-made or natural events even though effective public health policies could be developed and implemented [2].
Similarly, Lawn [24] there are indications that mortalities such infant, is improving in some developing countries, it appears there is less focus on health needs of older adults. Lawn [24], further argues that developed nations have shifted from health for all agenda to focusing on urgent issues such as, youth, maternal and child health, reproductive health, the provision of safe water and sanitation, reduction of malnutrition and infectious diseases such as malaria [2]. This has contributed to poor or lack of developing and adopting effective public health policies that was agreed to be the main focus of the Ottawa Charter. Whether this is due to poor public health policies, lack of effective and appropriate resources is not clear. Nevertheless, it is evident that lack of clear focus on “health for all” has contributed to inequalities in health in many developing nations [25,26]. However, it is reasonable to argue that unlike developed countries, health care is not free at the point of delivery. Therefore, unless individuals have finance capacity to meet the cost of their care, they are more likely to have poor health outcomes. As such, the notion of health for all by the year 2000 as set out in the Ottawa charter might be difficult to achieve in such circumstances [27]. Furthermore, while in developed nations the focus is on non-communicable diseases, supported by advanced medical technologies and innovations, such technologies hardly exist in developing nation [24]. This has contributed to discrimination and neglect and poor access to health declared by the charter. According to United Nations [27], health disparities by systematic factors such as, disadvantage, or discriminate against certain social groups, should not be condoned whether in developed or developing nations. However, in situations such those prevailing in developing countries, where combating communicable diseases remain the focus of public health policies, health for all in its entirety might be idealistic than realistic [28].
Moving Ottawa Charter Forward
The fundamental goal for national and international organizations is to improve health of population and reduce inequalities that seem to impact severely upon health. However, it can also be reasoned that socio-economic factors as well as health needs of population has changed since the Ottawa declaration [16,29]. It is therefore clear that for any national or international communities to enhance public health; there must be a need to focus on healthy public health policies that address the socio-economic factors that impact upon populations’ health. DoH [12] postulate that, rather than claiming that the existing gaps are due to poverty, public health policies must focus on dealing with key determinants of ill health amongst population or social determinants. According to DoH [12], most of these are due to poor social-economic policies that promote unfair distribution of wealth thereby creating inequalities [20].
As a result, in order to improve public health in some developed nations, there has been a move towards adoption of public health policies that address social determinants. Concepts such as political science have been integrated into public health policies (Department of Health and Children and the Health Service Executive [15]. In addition, in these countries, there are agreements that effective public health that facilitate reduced socio-economic gap can only prevail where there are supportive environments (Department of Health and Children and the Health Service Executive [15]. Furthermore, in most of these countries, the working conditions favour growth and developments. Whilst in developing countries, the majority of working age groups do work under very poor environments, in addition to job insecurities. As a result, the majority are unable to meet their basic health needs [30].
While there has been some development worldwide since declaration, in some continents such as Asia, Middle East, Africa and Far East, inequalities in health remains a huge issue [8]. In such cases, increased industrialisation has led to destructions of health sustaining factors such as community green spaces, safe neighbourhoods and healthy environments [16]; United Nations [27], contributing to more health risks.
In addition, poor work ethics have led to elevated levels of uncertainties amongst working age group in these parts of the world [5,17]. Eriksson and Lindstro [17] further claim that in most cases, some workers in developing countries hardly have legislation that protect their working conditions therefore have increased risks of unfair working terms and conditions.
Health Service Executive [10], therefore public health professionals urges leaders of private as well as non-governmental organizations to advocate for safe working as well as living conditions that are health and wellbeing supportive. All employees must be afforded with enjoyable and fulfilling and employment and working conditions, in addition to being considered as partners. This would lead to higher productivity and improved socio-economic health of population [10,22]. Whilst EUPHA [18] stipulate that it is clear that while socio-economic gaps might be presented as decreasing, particularly in developed countries, there are indications that some communities have lost interest and faith in their leaders thereby disengaging from political processes that shape their daily lives. This is more prominent in countries where the governments had to implement austerities in order to balance the economy where in some cases community facilities and public sectors have experienced reductions in their budgets. In order to move forward, WHO [23] as well as WHO [31] reiterate that effective health strategies must be based civic renewal, which supports the empowerment of communities rather than undermining it [14,32]. According to EUPHA [18], the focus must be to develop public health policies that facilitate development of personal skills through appropriate education for health, and enhancing life skills. While health care professionals must be proactive, base their judgements on evidences, the focus promoting socio-economic policies that deal with reductions of the inequalities [6,21]. Health care services need to be re-oriented to focus on preventing some of the most serious current public health threats such as communicable diseases, unhealthy lifestyles as well as environmental health risks [13,33].
It is clear that the Ottawa Charter’ is an opportunity to improve health worldwide. As such, public health professionals must focus on ensuring that:
• Every individual regardless of where they are born or live have equal access to resources and health. This can be done through improving their daily living conditions: the circumstances where people are born, grow, live and age, create social protection or public health policies supportive of all [13,21].
• Addressing the key contributors to inequitable distribution of power, money and resources, in particular structural factors that might contribute to discrimination against certain groups.
• Acknowledging that health for all is a key to development and prosperity for any nation addressing health inequities on health of population. This can be achieved through training public health professionals to focus on reduction of social determinants of health in addition to increasing public knowledge about the social determinants of health [2,13].
Conclusion
While governments have a duty to develop public health policies, it is the duty of public health professionals either as civil servants or private sectors to advocate for fair and just public health policies that not only favours parts of communities but all regardless of background. Advocacy must be based on credible and valid evidence-based that promote trust and support public [34]. This might require involving other stakeholders in decision-making and processes so that each party feels a sense of belonging and work towards one goal. That overall goal must be to reduce inequalities in health as stipulated by Ottawa Charter in 1986 to achieve health for all through reduction of inequalities in health.
References
- Bambra C, Smith KE, Garthwaite K, Joyce KE, Hunter DJ (2010) A labour of sisyphus? Public policy and health inequalities research from the black and Acheson reports to the Marmot review. J Epidemiol Community Health 65: 399-406.
- https://whqlibdoc.who.int/hq/2017/WHO_IER_CSDH_08.1_eng.pdf
- https://allcatsrgrey.org.uk/wp/wpfb-file/cherp142_economics_health_inequality_nhs-pdf/
- Mackenbach JP (2010) Can we reduce health inequalities? An analysis of the English strategy (1997-2010). J Epidemiol Community Health 65: 568-575.
- Marmot M (2010) Fair society, healthy lives the Marmot review, strategic review of health inequalities in England post-2010, HMSO.
- Hacking J, Muller S, Buchan I (2011) Trends in mortality from 1965 to 2008 across the english north-south divide: comparative observational study. BMJ 342: 7794.
- https://www.who.int/publications/almaata_declaration_en.pdf
- https://www.hse.ie/eng/staff/HR/Policies,_Procedures_and_Guidelines/Integrated_Employee_Wellbeing_and_Welfare_Strategy_.pdf
- Department of Health (2009) Tackling health inequalities: 10 years on a review of developments in tackling health inequalities in England over the last 10 years. Department of Health, London.
- https://www.publichealth.ie/healthinequalities/policy
- https://www.dohc.ie/publications/pdf/en_mens_health_policy.pdf?
- Department of Health (2008) Health inequalities: progress and next steps. Department of Health, London.
- Lomazzi M (2016) A global charter for the public’s health-the public health system: role, functions, competencies and education requirements. Eur J Public Health 26: 210-212.
- Mcqueen DV, De Salazar L (2011) Health promotion, the Ottawa Charter and ‘developing personal skills’: a compact history of 25 years. Health Promot Int 2: ii194-ii201.
- https://www.hse.ie/eng/services/Publications/Your_Service,_Your_Say_Consumer_Affairs/ Strategy/Service_User_Involvement.html
- https://lsbu.rl.talis.com/items/745D50CF-647D-0388-0032-23AB33A46970.html
- Eriksson M, Lindstro BM (2008) Debate: a salutogenic interpretation of the Ottawa char. Health Promot Int 23: 190-199.
- European Public Health Association (EUPHA) (2016) The Vienna declaration, Vienna.
- https://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_R10-en.pdf?ua=1.
- https://dera.ioe.ac.uk/11036/
- Halpin HH, Morales-Suárez-Varela MM, Martin-Moreno JM (2010) Chronic disease prevention and the new public health. Public Health Rev 32: 120-154.
- https://www.getirelandactive.ie/pdfs/GIA_GUIDE.pdf.
- https://www.who.int/healthpromotion/conferences/9gchp/shanghai-declaration-zero- draft.pdf
- Lawn J (2010) Are the millennium development goals on target? BMJ 341: 1136.
- Murray CJL, Michaud CM, McKenna MT, Marks JS (1998) US patterns of mortality by county and race: 1965-1994. Harvard center for population and development Studies, Cambridge, p: 98.
- Marmot M (2005) Social determinants of health inequalities. The Lancet 365: 1099-1104.
- United Nations (2007) World population prospects: the 2006 revision. United Nations department of Economic and Social Affairs: Population Division, NY, USA.
- Omran AR (2005) The epidemiological transition: a theory of the epidemiology of population change. Milbank Q 83: 731-757.
- House of Commons Health Committee (2009) Health inequalities third report of session 2008–2009; HMSO.
- Diethelm P, McKee M (2009) Denialism: what is it and how should scientists respond? Eur J Public Health 19: 2-4.
- World Health Organzation (2009) Milestones in health promotion statements from global conferences. World Health Oganization, Geneva, p: 42.
- https://www.economics-ejournal.org/economics/discussionpapers/2014-45
- https://www.lenus.ie/hse/bitstream/10147/97291/1/NewTobaccoControlPlan.pdf
- Rajaratnam JK, Marcus JR, Levin-Rector A, Chalupka AN, Wang H, et al. (2010) Worldwide mortality in men and women aged 15-59 years from 1970 to 2010: a systematic analysis. Lancet 375: 1704-1720.

