Keywords
Antitubercular Agents; Isoniazid; Rifampin; Tuberculosis; Pulmonary
INTRODUCTION
Despite all the efforts made to combat pulmonary tuberculosis it remains a severe health problem in many countries across the world, particularly owing to the increasing occurrence of a multi-drug-resistant form of the disease [1-3]. Following the expansion of the EU in 2004 and 2007, the eastern border of the European Union (EU) comprises 10 countries. On the east these countries border on nations with high tuberculosis notification rates. It is even feared that tuberculosis may be crossing borders at the eastern fringe of the EU [4]. Now more than ever, it is important to investigate not only the efficacy of standard treatments for tuberculosis but also their adverse effects.
Isoniazid and rifampicin have been used for several decades in the treatment of pulmonary tuberculosis. It has long been known that both of these drugs can lead to acute pancreatitis, and the first reports of this druginduced pancreatitis appeared in 1973 for rifampicin [5] and in 1994 for isoniazid [6]. Reviews of drug-induced pancreatitis generally just summarize case reports on a number of medications reported to have led to one or more cases of acute pancreatitis [7-11]. In determining whether drug-induced acute pancreatitis is uncommon or commonplace, epidemiological studies must establish just how high the risk is for a given agent [12].
PATIENTS AND METHODS
This retrospective study comprises 280 patients treated for pulmonary tuberculosis at Donetsk City Antitubercular Hospital (Ukraine) between 2009 and 2014. There were 192 (69%) men and 88 (31%) women with a mean age of 35.4 ± 3.8 years (range 18-65 years). Patients with previous acute pancreatitis or known chronic pancreatitis were excluded. As well as being asked about their medical history, with particular reference to previous diseases and current abdominal pain, after commencement of antitubercular therapy all patients underwent a physical examination with regard to abdominal pain, determination of pancreatic isoamylase (BIO-1A-Test Kit, Pliva-Lachema Diagnostika, Czech Republic; normal >90 U/l) and lipase (Beckman Coulter, USA; normal >67 U/l), and pancreatic sonography. The sonographic examination was carried out using a state-of-the-art digital device with multi-frequency sensors (ApliomMx, Toshiba, Japan). The following findings were regarded as evidence of acute pancreatitis: total or partial enlargement of the gland, blurred and irregular margins, decreased and irregular echogenicity, and peripancreatic fluid collections.
Isoniazid and rifampicin was prescribed according to the Ministry of Health of Ukraine standards for the treatment of tuberculosis according to the body weight of the patient: ≤ 74 kg 300 mg, 75–89 kg 400 mg and ≥ 90 kg 500 mg per day and ≤ 74 kg 600 mg and ≥ 75 kg 750 mg per day, respectively.
Three combinations of drugs were used for acute treatment of the tuberculosis:
Combination 1: Isoniazid, rifampicin, pyrazinamide, ethambutol (106 patients)
Combination 2: Isoniazid, rifampicin, pyrazinamide, streptomycin (14 patients)
Combination 3: In the case of resistance to first-line drugs: kanamycin, moxifloxacin, ethionamide, ethambutol, pyrazinamide (57 patients)
Two combinations of drugs were used for maintenance therapy:
Combination 4: Isoniazid, rifampicin (75 patients)
Combination 5: In the case of resistance to first-line drugs: ethionamide, moxifloxacin, pyrazinamide, ethambutol (28 patients)
Pancreatic involvement was defined as follows:
1. Definite acute pancreatitis: threefold or higher elevation of pancreatic isoamylase and lipase plus presence of ultrasound changes indicative of acute pancreatitis with or without abdominal pain (Group A)
2. Probable acute pancreatitis: threefold or higher elevation of pancreatic isoamylase or lipase plus either ultrasonography changes indicative of acute pancreatitis present or abdominal pain but with normal ultrasonography (groups C and E plus patients in group B, D and F with abdominal pain)
3. Enzyme elevation: any elevation of pancreatic isoamylase and/or lipase, but no abdominal pain and normal appearance of the pancreas on ultrasonography patients in Group B, D and F without abdominal pain
4. Normal pancreas: no enzyme elevation of any kind, normal ultrasound, no abdominal pain (Group H)
Three patients with normal pancreatic enzymes but ultrasonographic findings indicative of pancreatitis were excluded from further analysis due to suspicion of chronic pancreatitis (Group G)
Statistical analysis was performed using Fisher's exact test and logistic regression. Levels of significance are shown in the tables. All p-values were two-sided. P-values <0.05 were considered statistically significant. Analyses were performed with the SAS statistical software (version 9.2).
RESULTS
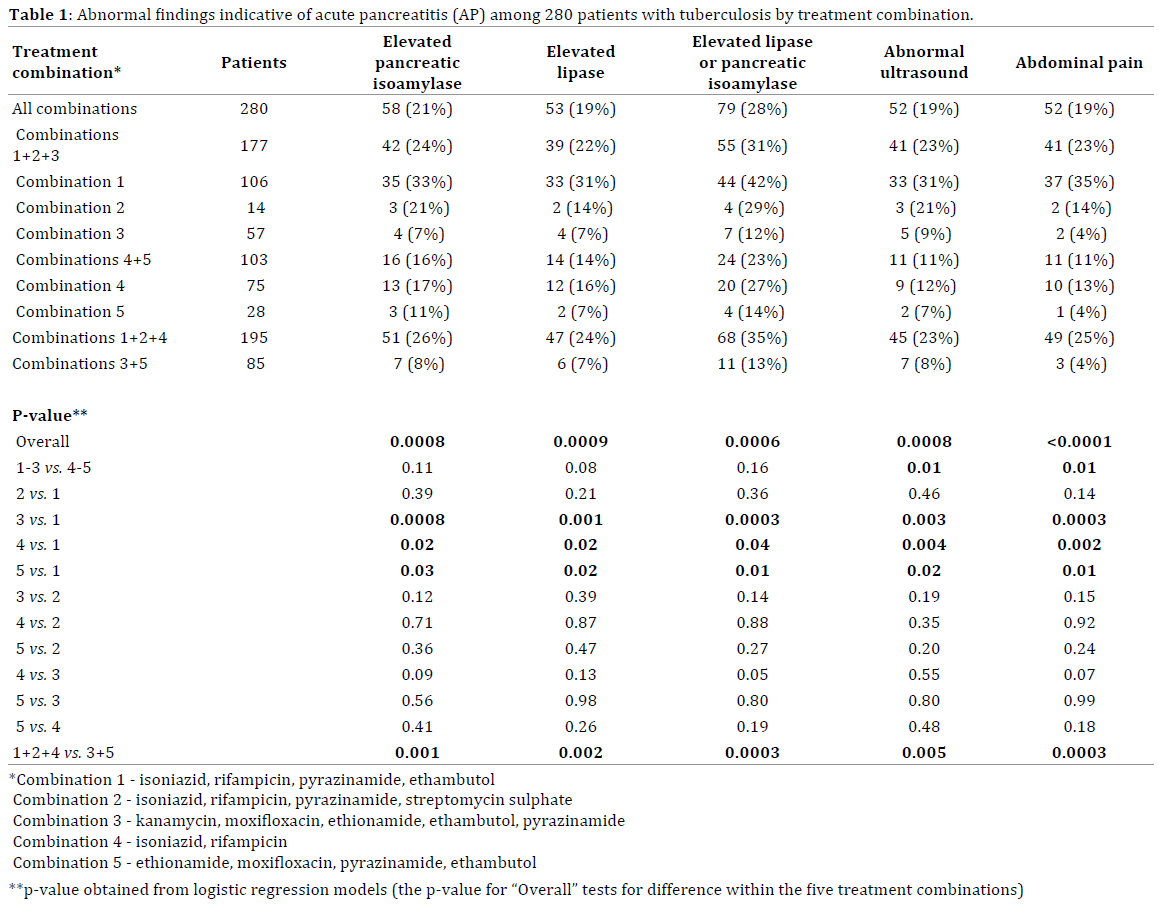
Of the 280 patients, 58 (21%) had elevated pancreatic isoamylase and 53 (19%) had elevated lipase. Overall, one or both of the two enzymes were elevated in 79 patients (28%). Fifty-two (19%) patients had ultrasonographic findings indicative of acute pancreatitis, and 52 (19%) patients had abdominal pain. Altogether, one in every four to five patients displayed potential signs of acute pancreatitis. These changes were significantly more pronounced in those treated with drug combination 1 than in those treated with combinations 3, 4 or 5, but not significantly greater than in those treated with combination 2. There were no significant differences regarding abnormal findings indicative of acute pancreatitis among patients treated with combinations 2, 3, 4 and 5 (Table 1).
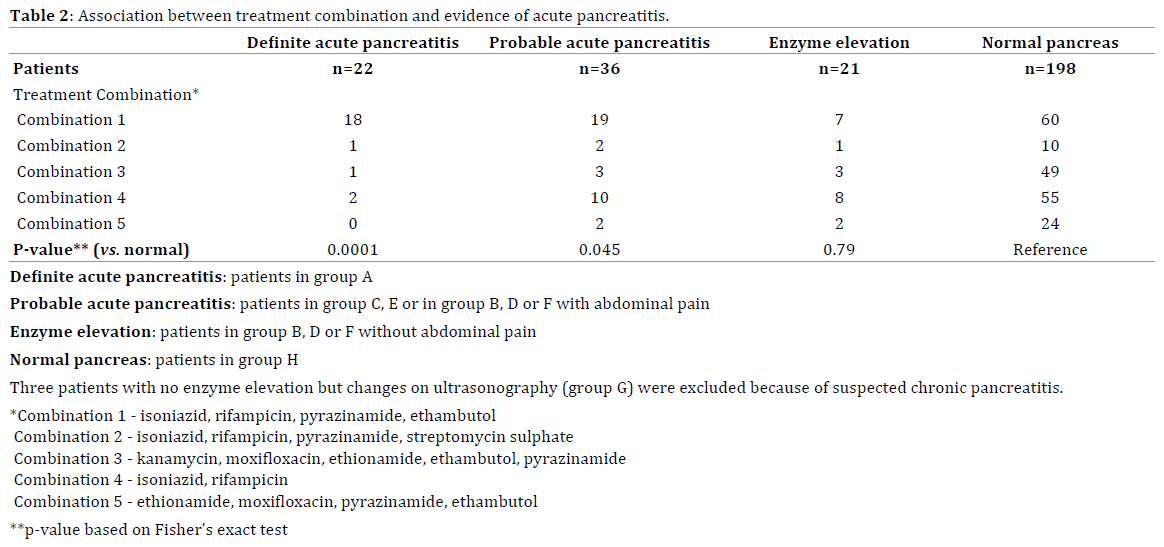
The distribution of treatment combinations differed significantly between Group A (patients with elevated pancreatic isoamylase and lipase plus ultrasonographic changes indicative of acute pancreatitis) and group H (patients in whom all parameters were normal). Groups B, C, D, E, F and G did not differ significantly from group H in this respect.
All in all, 22 (8%) patients had definite acute pancreatitis and 36 (13%) had probable acute pancreatitis. In 21 (8%) cases there was enzyme elevation. In the remaining 198 (71%) patients the pancreatic enzyme levels were in the normal range and ultrasonographic findings were normal. Three of these patients had abdominal pain that could not be attributed to disease of the pancreas. The proportions of patients with definite acute pancreatitis and probable acute pancreatitis varied significantly according to the treatment combination compared to patients with normal pancreas, but not to patients with enzyme elevation (Table 2).
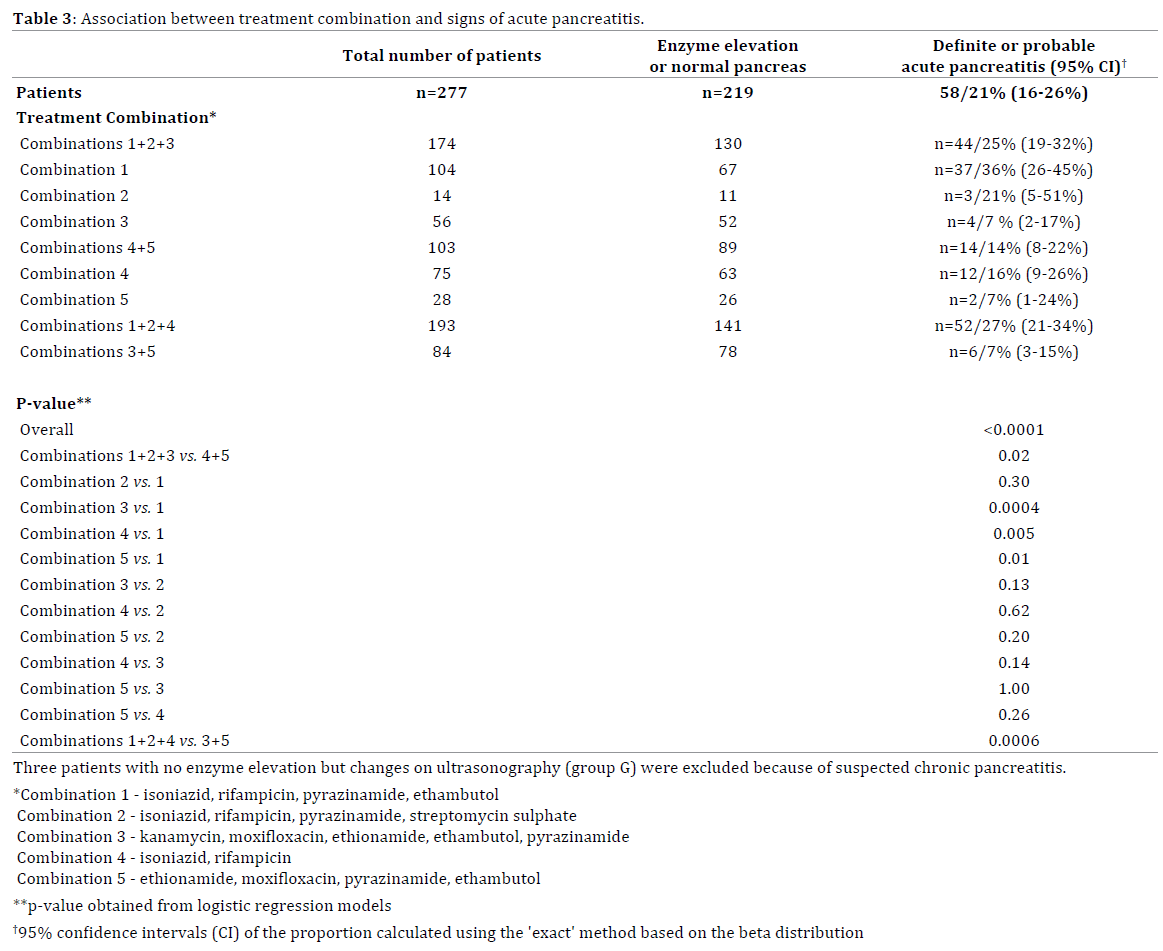
For further analysis patients with definite and probable acute pancreatitis were grouped together and compared to patients with enzyme elevation or no abnormalities (Table 3). The proportion of patients with definite or probable acute pancreatitis varied significantly according to treatment combination (P<0.0001). It was higher in patients treated with combination 1, 2, or 3 (acute therapy) than in those treated with combination 4 or 5 (maintenance therapy; P=0.02), and higher with combination 1 than with combination 3, 4 or 5.
DISCUSSION
Although it has long been known that isoniazid and rifampicin can trigger acute pancreatitis, case reports on this topic are not always covered in reviews on druginduced acute pancreatitis. According to Mallory and Kern [7] there was a proposed association for isoniazid, but evidence was contradictory or inadequate. They did not mention rifampicin at all. Trivedi and Pitchumoni [8] made no mention of isoniazid and assigned rifampicin to their class II, which embraced drugs reported to have caused more than 10 cases of acute pancreatitis. In the case of rifampicin it was 25 patients, but without rechallenge [8]. Badalov et al. [9] did not mention rifampicin but included isoniazid in their class IA (at least one case report with positive rechallenge and exclusion of all other causes of acute pancreatitis). They reported a total of eight cases, four of them confirmed by rechallenge. With one exception, all of these patients had received 300 mg isoniazid per day. The onset of acute pancreatitis after the initiation of isoniazid ranged from 6 hours to 21 days. Onset and rechallenge occurred within the first 6 hours in two patients, and at 5 days and 21 days in the other two rechallenged cases. All patients were male. In their first review of drug-induced acute pancreatitis, Nitsche et al. [10] summarized 26 patients in whom the association of rifampicin with pancreatitis was definite or probable [8, 13] In none of these cases, however, had rechallenge taken place. They did not mention isoniazid. In a second review, the same authors [11] included case reports of druginduced acute pancreatitis published between 2003 and 2011, but had found no new cases. They now described the association of rifampicin with pancreatitis as no more than probable.
The specific risk of pancreatitis associated with an individual drug is difficult to define [12]. The situation is seldom as clear as in the Swedish studies (both population-based case–control studies) that demonstrated a 60% increased risk of acute pancreatitis among current tetracycline users [14] and an increased risk with oral glucocorticoids (or 1.53, 95% CI 1.27–1.84) [15] and a Dutch study (multicentre population-based European casecontrol study) showing an increased risk with angiotensinconverting enzyme (ACE) inhibitors and calcium channel blockers (or 1.5, 95% CI 1.1–2.2; or 1.5, 95% CI 1.1-2.1) [16]. For the clinician, however, drug-induced pancreatitis is a rather uncommon, non-severe event [13], despite the observation that 42% of patients admitted during a first attack of AP had taken pancreatitis-associated drugs [17]. The treating physician should always ask what drugs are being taken and consider discontinuation.
A total of 25 and 11 case reports of acute pancreatitis attributed to rifampicin and isoniazid, respectively, have been published [18]. There is only one study comparable to ours. Mattson [5] investigated patients with newly diagnosed tuberculosis who received rifampicin from 1968 to 1972. Acute pancreatitis occurred in nine (2%) of the 547 patients, and a further six patients (1%) had abdominal symptoms due to elevated amylase that could not be attributed with certainty to acute pancreatitis. An asymptomatic serum amylase elevation was recorded in 20 patients (4%). In comparison, the figures in our study are much higher.
Altogether, 22 (8%) patients had definite acute pancreatitis and 36 (13%) probably had pancreatitis. In 21 (8%) of the patients there was an asymptomatic serum enzyme elevation. Viewing the patients with definite and probable acute pancreatitis together reveals the following (Table 3): definite/probable acute pancreatitis was found much more frequently during acute treatment (44/174, 25%) than during maintenance therapy (14/103, 14%). This difference is significant (P=0.02). The reason is unclear. Definite or probable acute pancreatitis occurred significantly more often with combination 1, which included isoniazid and rifampicin, than with combination 3, which did not contain these drugs (P<0.0001). There was no difference, however, between combination 1 and combination 2 (used in only a small number of patients), which also included isoniazid and rifampicin. In maintenance therapy combination 4, with isoniazid and rifampicin, led to definite or probable acute pancreatitis in 12 cases (16%), in contrast to combination 5, in which only two patients (7%) were affected.
The study features a number of limitations. For instance, we do not know whether the patients who developed definite or probable acute pancreatitis had other potential causes of pancreatitis, e.g. gallstones, alcohol abuse or hypertriglycaemia. On ethical grounds, no rechallenges were performed. Separate testing for isoniazid and rifampicin was not carried out. In fact, this is probably no longer feasible, because nowadays these two drugs are generally given together in the treatment of pulmonary tuberculosis.
Overall, however, definite or probable acute pancreatitis occurs in a very high proportion of patients treated with isoniazid and rifampicin for pulmonary tuberculosis. If a patient reports abdominal symptoms soon after commencement of therapy, the treating clinician must order diagnostic tests for acute pancreatitis. This is particularly important in cases where pancreatitis has previously occurred following treatment for tuberculosis, pulmonary or otherwise. The pancreas does not forget. In one case, acute pancreatitis during administration of isoniazid for genitourinary tuberculosis was followed 12 years later by renewed pancreatitis when the patient received isoniazid again for pulmonary tuberculosis [19].
Conflicting Interest
The authors had no conflicts of interest
References
- Caminero JA. Multidrug-resistant tuberculosis: epidemiology, risk factors and case finding. Int J Tuberc Lung Dis 2010;14:382-390. [PMID: 20202293]
- Hedt BL, van Leth F, Zignol M, Cobelens F, van Gemert W, Nhung NV, Lyepshina S, Egwaga S, Cohen T. Multidrug-resistance among new tuberculosis cases: detecting local variation through lot quality-assurance sampling. Epidemiology 2012;23:293-300. [PMID: 22249242]
- Post FA, Grint D, Werlinrud AM, Panteleev A, Riekstina V, Malashenkov EA, Skrahina A, Duiculescu D, et al. HIV-TB Study Group: Multi-drug-resistant tuberculosis in HIV positive patients in Eastern Europe. J Infect 2014;68:259-263. [PMID: 24247067]
- van der Werf MJ, Hollo V, Noori T. Is tuberculosis crossing borders at the Eastern boundary of the European Union? Eur J Public Health 2013;23:1058-1063. [PMID: 23813718]
- Mattson K. Side effects of rifampicin. A clinical study.Academic Dissertation.Medical Faculty of the University of Helsinki, 1973.
- Rabassa AA, Trey G, Shukla U, Samo T, Anand BS. Isoniazid-induced acute pancreatitis. Ann Intern Med 1994;121:433-434. [PMID: 8053617]
- Mallory A, Kern F Jr. Drug-induced pancreatitis: a critical review. Gastroenterology 1980;78:813-820. [PMID: 6986321]
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis. An update. J Clin Gastroenterol 2005;39:709-716. [PMID: 16082282]
- Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol 2007;5:648-661. [PMID: 17395548]
- Nitsche CJ, Jamieson N, Lerch MM, Mayerle JV. Drug induced pancreatitis. Best Practice Res Clin Gastroenterol 2010;24:143-155. [PMID: 20227028]
- Nitsche C, Maertin S, Schreiber J, Ritter CA, Lerch MM, Mayerle J. Drug-induced pancreatitis. Curr Gastroenterol Rep 2012;14:131-138. [PMID: 22314811]
- Grendell JH. Drug-induced acute pancreatitis: uncommon or commonplace? Am J Gastroenterol 2012;106:2189-2191. [PMID: 22138943]
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut 1995;37:565-567. [PMID: 7489946]
- Ljung R, Lagergren J, Bexelius TS, Mattsson F, Lindblad M. Increased risk of acute pancreatitis among tetracycline users in a Swedish population-based case-control study. Gut 2012;61:873-876. [PMID: 21957155]
- Sadr-Azodi O, Mattsson F, Bexlius TS, Lindblad M, Lagergren J, Ljung R. Association of oral glucocorticoid use with an increased risk of acute pancreatitis: a population-based nested case-control study. JAMA Intern Med 2013;173:444-449. [PMID: 23440105]
- Eland IA, Sundström A, Velo GP, Andersen M, Sturkenboom MJCM, Wiholm B, for the EDIP Study Group of the European Pharmacovigilance Research Group. Antihypertensive medication and the risk of acute pancreatitis: the European case-control study on drug-induced acute pancreatitis (EDIP). Scand J Gastroenterol 2006;41:1484-1490. [PMID: 17101581]
- Spanier BWM, Tuynman HARE, van der Hulst RWM, Dijkgraaf MGW, Bruno MJ, on behalf of the other members of the EARL Study Group: Acute pancreatitis and concomitant use of pancreatitis-associated drugs. Am J Gastroenterol 2011;106:2183-2188. [PMID: 21912439]
- Mattioni S, Zamy M, Mechai F, Raynaud J-J, Chabrol A, Aflalo V, Biour M, Bouchaud O: Isoniazid-induced recurrent pancreatitis. JOP 2012;10:314-316. [PMID: 22572141]
- Chow KM, Szeto CC, Leung CB, Li PKT: Recurrent acute pancreatitis after isoniazid. Netherlands J Med 2004;62:172-174. [PMID: 15366703]

