Marco Del Chiaro1, John Blomberg1, Ralf Segersvärd1, Elena Rangelova1, Christoph Ansorge1 and Caroline Verbeke2
1Division of Surgery, Department of Clinical Science, Intervention and Technology (CLINTEC) and 2Division of
Pathology, Department of Laboratory Medicine, Karolinska Institute, Stockholm, Sweden
- *Corresponding Author:
- Marco Del Chiaro
Division of Surgery, Department of Clinical Science,
Intervention and Technology (CLINTEC), Karolinska Institute,
Stockholm, Sweden
Phone +46858580000
Fax+46858586366
E-mail marco.del-chiaro@karolinska.se
Received September 09th, 2014 – Accepted October 27th, 2014
Context LigaSureTM is considered safe in performing pancreatoduodenectomy (PD). However, no data are available regarding the possible damage of tissues at the resection margins and the impact thereof on histologic margin assessment. Objective This study compares the degree of histologic damage to the resection margins when using LigaSureTM (group 1) or traditional ligature (group 2). Methods Both groups included 8 consecutive patients who underwent PD at Karolinska Institute in December 2013 (group 1) or earlier (group 2) by the same surgeon (MDC). The quality of tissues at the circumferential margins was compared between both groups by scoring for three different kinds of damage: tissue fragmentation, hemorrhage, and cell damage. Results The mean score for fragmentation was 1.3 (group 1) versus 1.7 (group 2; p=0.1). For hemorrhage the mean score was 0.8 (group 1) versus 1.5 (group 2; p=0.04). The mean score for celldamage was 1.4 (group 1) compared to 1.2 (group 2; p=0.1). Conclusions LigaSureTM does not cause tissue damage that could affect histologic margin assessment in PD specimens.
Keywords
Pancreas; Pancreaticoduodenectomy; Reproductive Techniques
INTRODUCTION
In recent years, LigaSureTM has been proposed as a novel, safe and effective device for performing PD [1] that allows reduction of operating time [2], intraoperative bleeding [3] and perioperative costs [4]. However, whether the potential tissue damage caused by radiofrequency tissue fusion [5] can hamper the microscopic evaluation of resection margins has not been studied yet. Resection margin status is a significant prognostic factor in pancreatic cancer that should be routinely evaluated by pathologists [6].
AIM
The aim of this study is to compare the nature and degree of microscopic damage to tissues at the resection margins when using LigaSureTM or traditional ligature for retroperitoneal tissue dissection.
METHODS
The quality of tissues at the “SMA-margin” in terms of histologic readability was compared between PD specimens that were dissected using LigasureTM (group 1) and those in which a traditional dissection technique was used (group 2). Both groups included 8 consecutive patients, who underwent a Whipple’s resection with radical lymphadenectomy (according to the Castelfranco Veneto classification, [7]) in December 2013 (group 1) or earlier (group 2). In case of suspected infiltration of the superior mesenteric/portal vein, vascular resection and reconstruction were performed. All operations were carried out by the same surgeon (MDC) in order to avoid inter individual variability in the surgical dissection technique. All specimens were examined following the institutional standard operating protocol [8]. The quality of the tissues at the margin was evaluated by a dedicated pathologist (CV) who was blinded to the surgical dissection method that had been used. A novel, simple scoring system was applied, which distinguishes between three dissectioninduced changes: tissue fragmentation, hemorrhage and cell damage (i.e. coagulation and crushing artifact) (Figure 1). The severity and extent of changes was scored as: none (0), mild and focal (1), moderate (2), severe and extensive (3).
Figure 1. Tissues at the resection margin are well preserved: a smooth, undisrupted tissue surface, only focal minimal hemorrhage (A) and intact cell
morphology (B) Extensive and severe tissue fragmentation with bleeding (C) and cell damage (D) precludes accurate microscopic assessment of the
resection margin.
STATISTICS
Comparison of the scores was done by Mann- Whitney U-test analysis using graph pad prism software®.
RESULTS
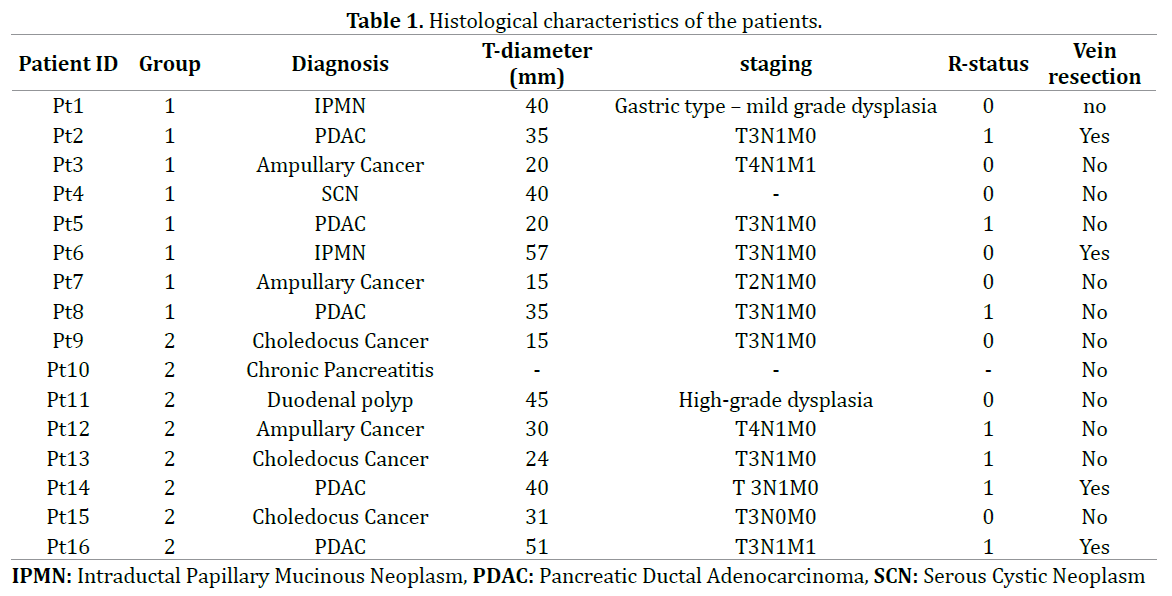
Patients in groups 1 and 2 had the same median age (68 years) at the time of surgery. Resection of the superior mesenteric/portal vein was performed in two patients of each group (25%). Final histology in group 1 showed pancreatic ductal adenocarcinoma (in 3 patients), cystic neoplasia (3), ampullary (2), whereas, group 2 included adenocarcinoma of the common bile duct (3), pancreas (2), ampulla (1) and duodenum (1) as well as chronic pancreatitis (1) (Table 1). The number of slides that were scored in each case was comparable between both groups (mean: 8 vs 8; range: 6-10 vs 6-9; p=0.1). The mean scores for tissue fragmentation (group 1: 1.3, range 1.1-1.7; group 2: 1.7, range 1.1-2.4) and cell damage (group 1: 1.4, range 1.2-2; group 2: 1.2, range 0.7-1.8) were similar (p=0.1). The mean score for hemorrhage at the resection margin was significantly lower in group 1 (0.8, range 0.1-1.8) than in group 2 (1.5, range 0.7-2.3; p=0.04).
Conclusion
The results of this study show that the use of LigaSureTM does not result in cell or tissue damage when compared with conventional technique (selective ligatures). On the contrary, the use of LigaSureTM is associated with significantly less hemorrhage and shows a trend towards less tissue fragmentation and cell damage. Overall, the use of LigaSureTM does not cause damage to the tissues at the dissection margins that could possibly hamper accurate histological margin assessment.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Pointer DT Jr, Slakey LM, Slakey DP. Safety and effectiveness of vesselsealing for dissection during pancreaticoduodenectomy. Am Surg 2013;79: 290-5. [PMID: 23461956]
- Eng OS, Goswami J, Moore D, et al. Safety and efficacy of LigaSureusage in pancreaticoduodenectomy. HPB(Oxford) 2013; 15: 747-52. [PMID: 23782268]
- Belli G, Fantini C, Cicilliano F, et al. Pancreaticoduodenectomyinportal hypertension: use of the Ligasure. J HepatobiliaryPancreat Surg2003; 10: 215-7. [PMID: 14605978]
- Gehig T, Muller-Stich BP, Kenngott H, et al. LigaSureversusconventional dissection technique in pancreaticoduodenectomy: a pilotstudy. Am J Surg 2011; 201: 166-70. [PMID: 20864081]
- Floume T, Syms RR, Darzi AW, Hanna GB. Optical, thermal, andelectrical monitoring of radio-frequency tissue modification. J BiomedOpt 2010; 15: 018003. [PMID: 20210489]
- Jamieson NB, Chan NI, Foulis AK, et al. The prognostic influence ofresection margin clearance following pancreaticoduodenectomyforpancreatic ductal adenocarcinoma. J GastrointestSurg 2013; 17: 511-21. [PMID: 23297028]
- Pedrazzoli S, Beger HG, Obertop H, et al. A surgical and pathologicalbased classification of respective treatment of pancreatic cancer.Summary on an international workshop on surgical procedures inpancreatic cancer. Dig Surg 1999; 16: 337-45.
- Verbeke CS, Leitch D, Menon KV, et al. Redefining the R1 resection inpancreatic cancer. Br J Surg 2006; 93: 1232-7. [PMID: 16804874]


