Keywords
Neoplasms, Cystic, Mucinous, and Serous; Pancreas; General Surgery
INTRODUCTION
Serous cystic neoplasms (SCNs) of the pancreas are wellknown tumours, usually regarded as benign entities exceptionally symptomatic with slow growth and rare malignant potential [1]. SCNs without complication should be followed and not operated. Uncertainty diagnosis is a too frequent surgical indication even though reliable diagnostic criteria have been established [1-7]. In fact, although the current imaging modalities are accurate in recognising the microcystic and honeycomb variants, the less common macrocystic and oligocystic variants are more challenging to diagnose3 because they can be confused with mucinous cystic neoplasms (MCNs) or intraductal papillary mucinous neoplasms (IPMNs) which are considered potentially malignant and in which a pancreatic resection is usually indicated. In their multicentre study of serous cystic neoplasms of the pancreas, in fact, Kimura et al. [3] reported that the preoperative diagnosis did not correctly identify SCNs in 57 (63%) of the 90 resected cases. To our knowledge, the role of a multidisciplinary approach in decision making for pancreatic cystic lesions has not yet been reported in the literature. Fitzgerald et al. [8]. have recently demonstrated that a multidisciplinary pancreatic surgical program increased the quality of care of patients affected by pancreatic ductal adenocarcinoma. The purpose of this study was to evaluate the usefulness of a multidisciplinary team (MDT) approach regarding decision making for the diagnosis and management of pancreatic serous cystic neoplasms.
METHODS
Data regarding 300 patients with pancreatic cystic lesions were collected in a prospective observational database from January 1990 to January 2014. A total of 43 (14.3%) patients with serous cystic neoplasms were extracted from the data base; 10 (23.2%) were followed up, and 33 (76.8%) underwent pancreatic resection. Written informed consent was obtained for each patient. Demographic, clinical, radiological, therapeutic, pathological and followup data were collected for each patient. Since 2005, the patients have been evaluated by a multidisciplinary team while, before 2005, the diagnosis and treatment of these tumours were usually indicated by the gastroenterologist or the surgeon. The multidisciplinary team of our Hospital was involved in the evaluation of all patients affected by pancreatic diseases. The team consists of 15 experienced medical doctors: 4 surgeons, 2 radiologists, 2 endoscopists, 5 gastroenterologists (2 with particular expertise in ultrasonography), 1 oncologist and 1 pathologist. Once a week, a meeting was held, and at least 10 patients affected by pancreatic diseases were evaluated and discussed by the MDT. The minimum number of people required to reach a decision was established as 10, and a decision was reached only when at least 60% of the people present were compliant. After each meeting, a record of the meeting with the decisions taken was available. Finally, each patient was informed by means of a written report regarding the decision reached by the multidisciplinary team. All patients evaluated by the multidisciplinary team (Group 1) were compared with those who were not evaluated by the multidisciplinary team (Group 2) as regards gender, age, symptoms, history of extra-pancreatic malignancy, the need for second level imaging techniques, including endoscopic ultrasound (EUS) plus fine needle aspiration (FNA) or magnetic resonance cholangio-pancreatography (MRCP), radiological diagnosis, imaging pattern of the cystic lesions, tumour site and size of the latero-lateral and cranio-caudal diameters, wall thickness and contrast enhancement, number of cysts, calcification, Wirsung dilatation and type of management (surgery versus surveillance).
Abdominal US and computed tomography (CT) scans were performed for all patients while EUS plus FNA and MRCP were available only after the year 2000. Thus, regarding the radiological diagnosis, all patients were studied utilising abdominal ultrasound and computed tomography. Only after 2000 were second level imaging techniques (EUS plus FNA and MRCP) carried out in doubtful cases. Patients in the surveillance group, potentially fit for surgery, were followed up yearly with abdominal US and CT scans for at least two years and were then re-discussed by the MDT. The patients who underwent surgery were re-discussed by the MDT at discharge from the hospital, but they were not followed up. A laparoscopic distal pancreatectomy was performed for the first time in our Institute at the beginning of the year 2000.
Statistical analysis
All the categorical variables were reported as frequencies and percentages while the continuous variables were reported as medians and ranges. Univariate analysis was carried out using the Fischer exact test and the Mann- Whitney U test. All variables presenting a P value <0.1 in the univariate analysis were included in the multivariate model. Multivariate analysis was carried out using logistic regression. Two-tailed P values less than 0.05 were considered statistically significant. All statistical analyses were carried out running the Statistical Package for Social Science (SPSS, Chicago, IL), version 13.
RESULTS
The characteristics of the 43 patients with SCNs are summarised in Table 1. There were 12 (27.9%) males and 31 (72.1%) females; median age was 66 (28-84) years. Symptoms were present in 19 (44.2%) patients, and there was a history of extrapancreatic malignancy in 10 (23.3%) patients. Second level imaging techniques were carried out in 18 (41.9%) cases and a radiological diagnosis of SCN was made in the majority of cases (29 cases, 67.4%) while, in the remaining 14 (32.6%) cases, various other pancreatic cystic lesions were diagnosed. Regarding the radiological pattern of the cystic lesions, 24 patients had microcystic lesions (55.8 %) and 19 had macrocystic lesions (46.2%). In the majority of cases (55.8%), the lesions were located in the pancreatic head; the median latero-lateral and cranio-caudal diameters were 35 mm and 40 mm, respectively. Wall thickness ≥ 2mm was recorded in 21 (48.8%) lesions. The majority of the tumours contained a multiple number of cysts (37 cases; 86%) and were without calcifications (36 cases; 83.7%), without dilatation of the main pancreatic duct (33 cases; 76.7%) and without CT-scan contrast enhancement (30 cases; 69.8%). Thirtythree (76.7%) patients underwent surgery; 10 (23.3%) were followed-up. Surgical indications were an uncertain diagnosis with malignant tumour in 14 cases (32.6%) and a symptomatic serous cystic tumours in 19 cases (44.2%) (16 recurrent abdominal pain, 3 obstructive jaundice). Left pancreatectomies with or without a splenectomy were performed in 15 (45.4%) cases, of which 5 (33.3%) were carried out using the laparoscopic approach: a pancreaticoduodenectomy in 10 (30.3%), atypical resection in 6 (18.1%), and both total pancreatectomy and palliative procedures in 1 (3.1%) case. Postoperative mortality, morbidity and postoperative pancreatic fistula (POPF) were 3.0% (1/33), 39.4% (13/33) and 15.1% (5/33), respectively. All patients with preoperative diagnosis of asymptomatic serous cystic were followed up. No patients underwent surgery during follow-up.
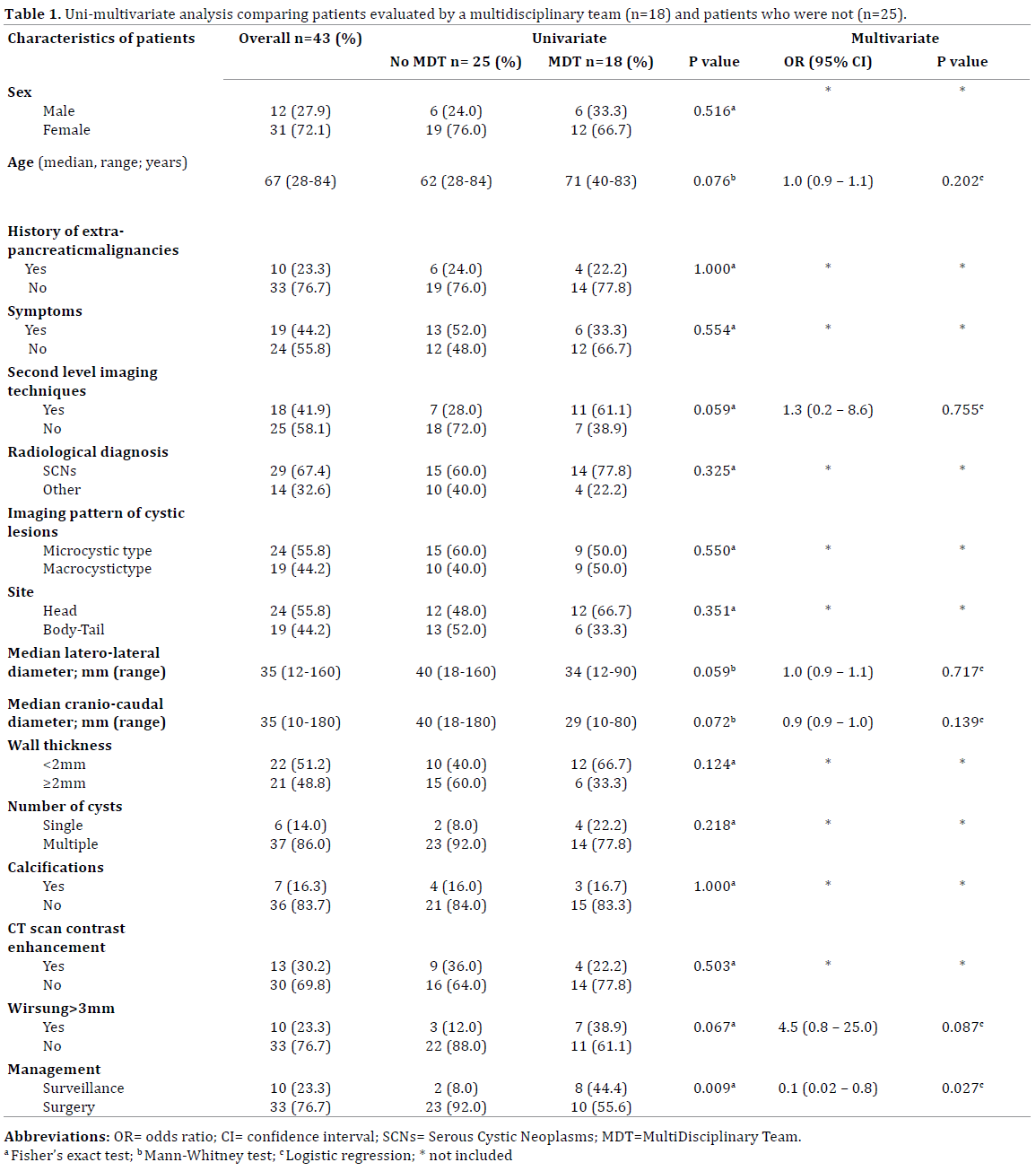
A comparison between patients who underwent MDT evaluation and patients who did not is reported in Table 1. At univariate analysis, the type of management was significantly related to an MDT evaluation (P=0.009). In fact, fewer surgical approaches were carried out in patients who underwent MDT evaluation (n=18) than in patients who did not (n=25) (10/18 cases; 55.6% versus 23/25 cases; 92.0%, respectively). Conversely, surveillance was suggested more frequently in patients who underwent MDT evaluation (8/18 cases; 44.4%) with respect to those who did not (2/25 cases; 8.0%). Age, second level imaging techniques, latero-lateral diameter, cranio-caudal diameter, Wirsung duct size and radiological diagnosis differed between the two groups; however, the differences were not statistically significant. The median age was higher in the MDT group than in the no MDT group (71 versus 62 yrs) (P=0.076); second level imaging techniques were more frequently carried out in the MDT group than in the no MDT group (11/18 cases; 61.1% versus 7/25 cases; 28.0%) (P=0.059). The cystic lesions were greater in size in the no MDT group than in the MDT group (latero-lateral diameter, 40 mm versus 34 mm; cranio-caudal diameter, 40 mm versus 29 mm; P=0.059 and 0.072, respectively). Finally, the Wirsung duct was more frequently dilated (>3mm) in the MDT group than in the no MDT group (7/18 cases; 38.9% versus 3/25 cases, 12.0%; P=0.067). Multivariate analysis strongly confirmed that the only factor significantly related to an MDT evaluation was the type of management, suggesting that MDT evaluation independently reduced the odds of surgery (OR 0.1; 95% CI 0.02-0.8; P=0.027).
DISCUSSION
In 1978, Compagno and Oertel [9] first reported serous cystic neoplasms of the pancreas. According to this report, SCNs appear as multiple (>6), small cysts (<2mm) aggregating to give a honeycomb appearance with an irregular, thin capsule (microcystic SCN). Subsequently, other types of SCNs were recognised. In fact, some SCNs consist of larger cysts (macrocystic SCNs) or are of a noncystic type (solid-type SCNs)[10-12]. In addition, they are usually benign tumours with rare malignant potential even if the prevalence of cancer among serous cystadenomas is reported to be 3%, the first case being reported in the literature in 1989 [13]. Several imaging modalities are available, and the criterion characteristics for the diagnosis of SCNs are the honeycomb appearance and central calcification of the tumour [3, 14-17]. Moreover, these tumours do not communicate with the Wirsung duct, and the carcinoembryonic antigen (CEA) level in the cystic fluid is inferior to 0.5 ng/ml (reference value <5, no smokers; <6.5 smokers) [18, 19]. Kimura et al. have reported that EUS is the best modality for diagnosing the honeycomb appearance, detecting it in 69% of resected cases [3]. This characteristic was detected by MRI (67%), CT scan (55%) and US (58%) of the resected cases. In particular, the honeycomb appearance was seen in 100% of the microcystic type by EUS. Thus, the absence of the honeycomb appearance or central calcification, as happens in macrocystic and noncystic SCNs, will lead to difficulty in the differential diagnosis of SCNs from other pancreatic lesions. However, Kimura et al. have reported that the number of followed-up patients significantly increased from 1990 to 2008 [3]. In fact, during the period between 1990 and 2002, SCNs were always respected; however, since 2003, the number of patients with SCNs who are simply observed has increased, most likely owing to the growing accuracy of the preoperative diagnosis. In our experience, a multidisciplinary team approach has allowed a significant increase in patients who have been followed up (from 8% of the patients who were not evaluated with an MDT approach to 44.4% of the patients with an MDT approach); on the contrary, there has been a significant decrease in those patients who underwent surgery (from 92% of the patients who were not evaluated with an MDT approach to 55.6% of the patients evaluated with an MDT approach). This result was probably due to the composition of the MDT which included experienced and dedicated medical doctors (surgeons, radiologists, endoscopists, gastroenterologists, oncologist and pathologist) capable of recognising the characteristic findings of SCNs. In addition the availability to use second level imaging techniques, as well as MRCP and EUS plus FNA, may allow a better definition of the morphological features of the cystic lesion and properly establish both the absence of communication of the cystic lesions with the Wirsung duct and Wirsung duct size. Finally, the CEA level in the cystic fluid may help the MDT in the diagnosis and the choice of treatment to be carried out. Moreover, it has been considered that, during the MDT period, the higher number of cases followed-up were probably in relation to the smaller size of the lesion that increased the number of incidental SCNs, without surgical indication.
The limitations of the study were the small sample size of the cohort analysed and the retrospective design. In conclusion, despite the limitations of the study, we suggest a multidisciplinary team approach for serous cystic tumours of the pancreas as much as it seems to be useful in recognising patients with a preoperative diagnosis of SCN and in allowing its proper management. However, additional observational, prospective studies with a large cohort of SCNs are needed to verify the usefulness of a multidisciplinary team approach in these lesions.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- El-Hayek KM, Brown N, O'Rourke C, Falk G, Morris-Stiff G, et al. Rate of growth of pancreatic serous cystadenoma as an indication for resection. Surgery 2013; 154: 794-800. [PMID: 24074417]
- Salvia R, Malleo G, Marchegiani G, Pennacchio S, Paiella S, et al. Pancreatic resections for cystic neoplasms: from the surgeon's presumption to the pathologist's reality. Surgery 2012; 152: S135-142. [PMID: 22766364]
- Kimura W, Moriya T, Hirai I, Hanada K, Abe H, et al. Multicenter study of serous cystic neoplasm of the Japan pancreas society. Pancreas 2012; 41: 380-387. [PMID: 22415666]
- Zanini N, Fantini L, Casadei R, Pezzilli R, Santini D, et al. Serous cystic tumors of the pancreas: when to observe and when to operate: a single-center experience. Dig Surg 2008; 25: 233-239. [PMID: 18607110]
- Malleo G, Bassi C, Rossini R, Manfredi R, Butturini G, et al. Growth pattern of serous cystic neoplasms of the pancreas: observational study with long-term magnetic resonance surveillance and recommendations for treatment. 2012; Gut 61: 746-751. [PMID: 21940725]
- Galanis C, Zamani A, Cameron JL, Campbell KA, Lillemoe KD, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J GastrointestSurg 2007; 11: 820-826. [PMID: 17440789]
- Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW, et al. Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg 2005; 242: 413-419. [PMID: 16135927]
- Fitzgerald TL, Seymore NM, Kachare SD, Zervos EE, Wong JH. Measuring the impact of multidisciplinary care on quality for pancreatic surgery: transition to a focused, very high-volume program. Am Surg 2013; 79: 775-780. [PMID: 23896243]
- Compagno J, Oertel JE. Microcystic adenomas of the pancreas (glycogen-rich cystadenomas): a clinicopathologic study of 34 cases. Am J ClinPathol 1978; 69: 289-298. [PMID: 637043]
- Egawa N, Maillet B, Schröder S, Mukai K, Klöppel G. Serous oligocystic and ill-demarcated adenoma of the pancreas: a variant of serous cystic adenoma. Virchows Arch 1994; 424: 13-17. [PMID: 7526946]
- Le Borgne J, de Calan L, Partensky C. Cystadenomas and cystadenocarcinomas of the pancreas: a multiinstitutional retrospective study of 398 cases. French Surgical Association. Ann Surg 1999; 230: 152-161. [PMID: 10450728]
- Casadei R, D'Ambra M, Pezzilli R, Ricci C, Calculli L, et al. Solid serous microcystic tumor of the pancreas. JOP 2008; 9: 538-540. [PMID: 18648150]
- Bramis K, Petrou A, Papalambros A, Manzelli A, Mantonakis E, et al. Serous cystadenocarcinoma of the pancreas: report of a case and management reflections. World J SurgOncol 2012; 10: 51. [PMID: 22400805]
- Antonini F, Fuccio L, Fabbri C, Macarri G, Palazzo L. Management of serous cystic neoplasms of the pancreas. Expert Rev GastroenterolHepatol. [PMID: 24981593]
- Lin XZ, Wu ZY, Li WX, Zhang J, Xu XQ, et al. Differential diagnosis of pancreatic serous oligocystic adenoma and mucinous cystic neoplasm with spectral CT imaging: Initial results. ClinRadiol 2014; 69: 1004- 1010. [PMID: 24919983]
- Chu LC, Singhi AD, Hruban RH, Fishman EK. Characterization of pancreatic serous cystadenoma on dual-phase multidetector computed tomography. Comput Assist Tomogr 2014; 38: 258-263. [PMID: 24625608]
- Robinson SM, Scott J, Oppong KW, White SA. What to do for the incidental pancreatic cystic lesion? SurgOncol 2014; 23: 117-125. [PMID: 24846834]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology 2004; 126: 1330- 1336. [PMID: 15131794]
- Spence RA, Dasari B, Love M, Kelly B, Taylor M. Overview of the investigation and management of cystic neoplasms of the pancreas. Dig Surg 2011; 28: 386-397. [PMID: 22179508]

