Keywords
Cholangiopancreatography, Endoscopic Retrograde; Pancreatic Ducts; Pancreatitis, Alcoholic; Pancreatitis
Abbreviations
APD: accessory pancreatic duct; MPD main pancreatic duct
INTRODUCTION
The anomalies of the pancreatic ducts are not very frequent and, in general, they are divided into three groups: i) independent pancreatic ducts; ii) inversion of the two ducts; and iii) absence of the duct of Santorini. Embryology can be used to explain these anomalies [1, 2].
Two outpouchings from the endodermal lining of the duodenum develop at this time: the ventral pancreas and the dorsal pancreas. The dorsal anlage grows more rapidly and, by the sixth week, it is an elongated nodular structure extending into the dorsal mesentery in which its growth continues. The ventral pancreas remains smaller and is carried away from the duodenum by its connection with the common bile duct. The two primordia are brought into apposition by the uneven growth of the duodenum and they fuse by the seventh week. The tail, body, and part of the head of the pancreas are formed by the dorsal component; the remainder of the head and the uncinate process derive from the ventral pancreas. These primitive relations are still distinguishable in the adult pancreas [3].
The dorsal duct arises directly from the duodenal wall and the ventral duct arises from the common bile duct. On fusion of the ventral and dorsal components, the ventral duct forms an anastomosis with the dorsal one, forming the main pancreatic duct. The proximal end of the dorsal duct becomes the accessory duct in adults and is patent in 70% of the specimens [4].
The common outlet of the bile duct and the pancreatic duct observed in most adults is the result of the common origin of the bile duct and the ventral pancreas.
The duct of Santorini is completely independent of the duct of Wirsung and drains in the duodenum by itself in 10% of the cases. In the other 90%, the duct of Wirsung is the principal excretory route for pancreatic juice. When the duct of Santorini represents the main excretory route of the pancreas, the duct of Wirsung may be wholly absent, have a very small opening into the duodenum, or be a branch of the duct of Santorini without communication with the ampulla of Vater. In rare instances, both openings into the duodenum may be vestigial, with subsequent massive dilatation of the pancreatic duct and obstructive pancreatitis [5, 6].
Many studies have been carried out, mainly of the main pancreatic duct, from the radiographic point of view; however, few studies have examined the accessory pancreatic duct, which exhibits several valuable characteristics for the diagnosis of the pancreatic diseases.
The presence, course and shapes of the accessory pancreatic duct have not been previously studied in patients with chronic pancreatitis. In this study, we evaluated the behavior of the accessory pancreatic duct using endoscopic retrograde cholangiopancreatography (ERCP) in patients with chronic pancreatitis and we compared it with a group of patients having a normal pancreatogram.
MATERIAL AND METHOD
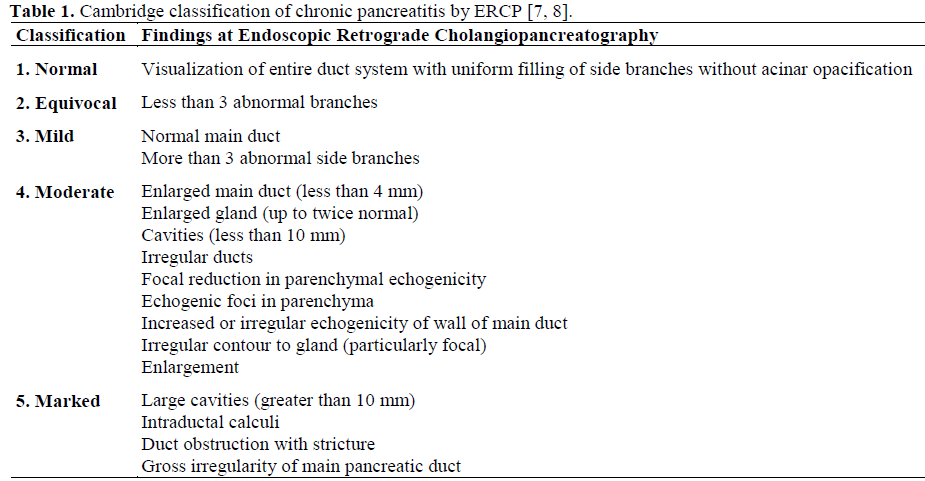
A prospective study was carried out on 157 consecutive patients (79 males and 78 females) who underwent ERCP for suspicion of pancreatobiliary disease in the Department of Endoscopy of the National Institute of Gastroenterology of Havana, Cuba from January 1995 to March 2003. In order to compare the accessory pancreatic duct (APD), ERCP was performed and patients were subdivided into two groups and classified for chronic pancreatitis according to the Cambridge classification (Table 1) [7, 8]: patients with chronic pancreatitis (n=48, 30.6%; 30 males and 18 females; alcoholic: 28, 58.3%; metabolic: 4, 8.3%; idiopathic: 16, 33.3%) and patients with a normal pancreatogram (n=109, 69.4%; 49 males and 60 females). In the series, we did not have patients with pancreas divisum.
All pancreatograms were taken by dye contrast injection through the major duodenal papilla, in the Radiology Department of the National Institute of Gastroenterology in Havana, Cuba. In all cases, the presence of the APD was satisfactorily demonstrated by the outflow of the contrast medium through the minor papilla and radiological images. Patients in which the visualization of the APD was not satisfactory were eliminated from the study.
The following criteria were considered in order to establish the insertion type of the accessory pancreatic duct to the main pancreatic duct (MPD): short insertion (the APD joined the MPD near its first inferior branch (Figure 1), intermediate insertion (the APD joined the MPD between its superior and inferior branches (Figure 2), long insertion (the APD joined the MPD at the neck portion (Figure 3), handle type (the APD ran and arched into the caudal portion of the head of the pancreas) and amputated APD (the flow of the contrast through the APD stopped suddenly). To describe the terminal portion of the APD, we applied the classification used by Kamisawa et al. from Tokyo Metropolitan Komagome Hospital in Japan [9]: stick type (gradual narrowing of the ended portion), branch type (gradual narrowing of the duct which gave off several fine terminal branches), saccular type (saccular termination), spindle type (ampullary termination), Cudgel type (termination was associated with a duct diameter greater than 2 mm (Figure 4), and halfway (“Y” termination).
Figure 1. Accessory pancreatic duct of short insertion
in a patient with chronic pancreatitis.
Figure 2. Accessory pancreatic duct of intermediate
insertion in a patient with a normal pancreatogram.
Figure 3. Accessory pancreatic duct of long insertion
at pancreatic neck level in a patient with a normal
pancreatogram.
Figure 4. The shape of the terminal portion of the
accessory pancreatic duct in patients with chronic
pancreatitis. Cudgel type.
ETHICS
Patients were asked for verbal informed consent to document their clinical data and endoscopic procedures. The study was approved by the local ethics committees of the National Institute of Gastroenterology.
STATISTICS
Data are reported as absolute and relative frequencies. Data were analyzed by means of the Student's t-test and contingency tables (Pearson's, Yates' corrected, and Mantel- Haenszel for linear trend chi-squared tests were applied where appropriate). The significance level of each single frequency vs. the expected one was evaluated by means of the hierarchical log-linear model. Two-tailed P values less than 0.05 were considered statistically significant. The data analysis was performed by running the SPSS/PC+ statistical package on a personal computer.
RESULTS
Table 2 shows the distribution of sex and age in patients with chronic pancreatitis and a normal pancreatogram. A predominance of the male gender was observed (although not reaching statistical significance: P=0.064) in the group of patients with chronic pancreatitis (62.5%) as compared to the control group (45.0%).
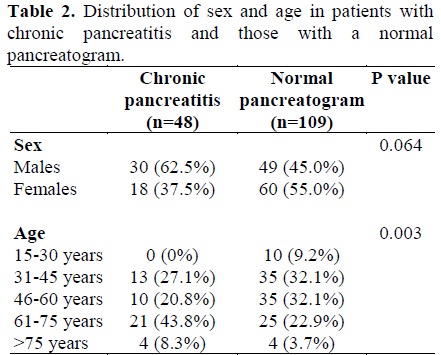
According to age, the majority of patients with chronic pancreatitis were more than 60 years old (52.1%), while in the group of patients with a normal pancreatogram, a high frequency of patients less than or equal to 60 years was observed (73.4%); the difference between two groups was statistically significant (P=0.003).
When comparing the insertion type of APD to MPD (Figure 5), we observed a significant difference (P<0.001) between the two groups. In patients with chronic pancreatitis, the short insertion predominated (31/48, 64.6% vs. 16/109, 14.7% in patients with normal pancreatogram; P=0.007) while in patients with a normal pancreatogram, the intermediate insertion (46/109, 42.2% vs. 8/48, 16.7% in chronic pancreatitis; P=0.054) and the long insertion (41/109, 37.6% vs. 5/48, 10.4% in chronic pancreatitis; P=0.018) prevailed although only the long insertion reached statistical significance. No significant differences in the frequency of handle type insertion were found (6/109, 5.5% in patients with a normal pancreatogram vs. no cases in chronic pancreatitis; P=0.124). Finally, a significant frequency of amputated APD was observed in patients with chronic pancreatitis (4/48, 8.3% vs. no cases in patients with normal pancreatogram; P=0.019).
Figure 5. Insertion type of the accessory pancreatic
duct to the main pancreatic duct in patients with
chronic pancreatitis and in patients with a normal
pancreatogram. (Overall comparison between patients
with chronic pancreatitis and patients with a normal
pancreatogram: P<0.001).
Table 3 shows the correlation between the severity of chronic pancreatitis diagnosed using ERCP (assessed by Cambridge classification) and the insertion type of the APD to the MPD. In all patients, the short insertion prevailed, regardless of the degree of intensity of pancreatitis (P=0.125); however, in patients with marked chronic pancreatitis, a borderline higher frequency of amputated APD was observed (4/18, 22.2% vs. no cases in the 30 mild/moderate chronic pancreatitis; P=0.067).
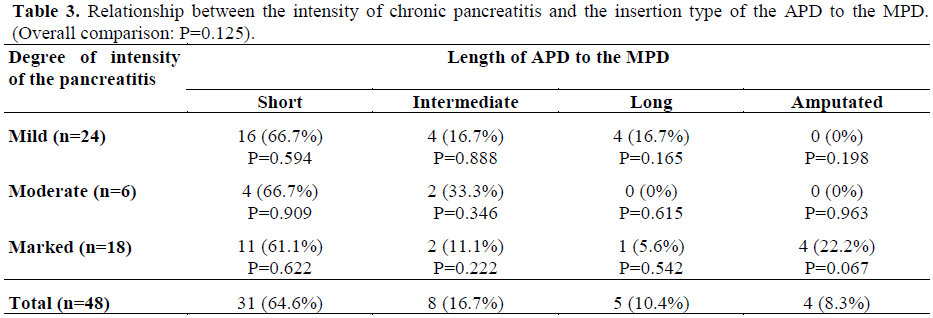
Figure 6 illustrates the distribution of the shape of the terminal portion of the APD in patients with chronic pancreatitis and in patients with a normal pancreatogram (patients with amputated APD were not taken into account). A significant difference was observed between the two groups (P<0.001). In patients with chronic pancreatitis, the Cudgel type prevailed (34/44, 77.3% vs. 15/109, 13.8% in normal pancreatogram patients; P<0.001) while, in patients with normal pancreatogram, the stick shape prevailed (66/109, 60.6% vs. 6/44, 13.6% in patients with chronic pancreatitis; P=0.033).
Figure 6. Terminal portion of the accessory pancreatic
duct in patients with chronic pancreatitis and those
with a normal pancreatogram. (Overall comparison
between patients with chronic pancreatitis and patients
with normal pancreatogram: P<0.001).
When we analyzed the diameter of the APD in the Cudgel type, it was significantly wider in the 34 patients with chronic pancreatitis (3.61±1.30 mm) when compared with that of the 15 patients showing a normal pancreatogram (2.47±0.83 mm) (P<0.001).
DISCUSSION
The presence of the APD was demonstrated by the direct injection of dye contrast into the pancreatic duct of removed and postmortem specimens. ERCP was used in the evaluation of the APD through dye injection into the minor papilla. However, in many cases, the orifice of the minor papilla is very small and the exact evaluation of the APD is practically impossible by this method. In our study, we injected the contrast by ERCP visualizing the contrast outflow through the minor papilla by means of radiographic study.
Our investigation agreed with the literature which reports that chronic pancreatitis affects men more frequently than women. In population studies, males are affected more commonly than females (6.7 versus 3.2 per 100,000 populations) [9].
Sex differences with respect to etiology are also reported in the literature: alcohol-induced illness is more prevalent in males, idiopathic and hyperlipidemic-induced pancreatitis is more prevalent in females, and equal sex ratios are observed in chronic pancreatitis associated with hereditary pancreatitis [10].
The rate of chronic pancreatitis peaks at 45-54 years of age in males and then declines; female rates reach a plateau which remains stable after 35 years of age. The mean age at diagnosis is 46±13 years. In idiopathic chronic pancreatitis, a bimodal age distribution has been reported, designated as early-onset form (median age 19.2 years) and late-onset form (median age 56.2 years) [11, 12]. In our study, the diagnosis of chronic pancreatitis prevailed in older people (over 60 years of age).
In a study of 176 pancreatograms carried out by Dr. Kamisawa, it was found that the insertion type of APD was long in 51 patients (29.0%); intermediate in 75 (42.6%); short in 21 (11.9%) and ansa type in 29 (16.5%) [9]. These results are very similar to our study in which a slight prevalence existed in patients with the intermediate type insertion [13].
When analyzing the insertion type in patients with chronic pancreatitis we observed that the short type prevailed, although similar studies were not found in the literature. We think that the short type insertion could be considered as an anatomic risk factor for the development of chronic pancreatitis since, although the function of the APD is ignored, it could serve as drainage to the MPD, and it would prevent the appearance of chronic pancreatitis by reducing the pressure of the MPD.
Therefore, since the APD is shorter and closer to its outlet in the minor papilla, the possibility of drainage of the pancreatic gland would be limited only to the head; the drainage of the pancreatic secretion coming from the body and the tail would be even more restricted. This would favor a pressure increase inside the MPD, with the resulting unchaining of the physiopathological mechanisms implied in the pathogenesis of chronic pancreatitis, independently of the primary cause [14].
In our investigation, it was demonstrated that only 5 patients (10.4%) with chronic pancreatitis had an APD of long type insertion, supporting the hypothesis that a pancreas is better drained by the long duct, thus helping to decompress the MPD and avoid pancreatic pain and the progression of the disease [15]. This could be related to the role performed by this duct in patients with chronic pancreatitis which is to serve as a second drainage system to the flow of pancreatic juice. This supports our hypothesis that, in patients with chronic pancreatitis, the APD could act as a “security” valve.
In conclusion, in patients with chronic pancreatitis, the short type of insertion of the APD prevailed, suggesting that this is the most frequent type of insertion in this disease. This could be a risk factor to keep in mind when studying patients having clinical suspicion of chronic pancreatitis or at risk of having the disease. We found that the APD of the Cudgel type was enlarged to about twice the normal size in chronic pancreatitis patients as compared to the control group.
Finally, we believe that the APD must be analyzed when performing a cholangiopancreatography diagnosis of chronic pancreatitis and instead of only focusing on the main pancreatic duct or its accessory branches, as reported in many classifications.
References
- Clain JE, Pearson RK. Diagnosis of chronic pancreatitis. Is a gold standard necessary? Surg Clin North Am 1999; 79:829-45. [PMID 10470330]
- Mackie CR, Moossa AR. Surgical anatomy of the pancreas. In: Moossa AR, ed. Tumors of the Pancreas. Baltimore, MD, USA: Williams & Wilkins, 1980.
- Arey LB. Developmental Anatomy: A Textbook and Laboratory Manual of Embryology. 7th ed. Philadelphia, PA, USA: WB Saunders, 1974.
- Patten BM. Human Embriology. 3rd ed. New York, NY, USA: McGraw-Hill, 1968.
- Kleitsch WD. Anatomy of the pancreas: a study with special reference to the duct system. Arch Surg 1955; 71:795-9.
- Go VLW, DiMagno EP. Normal pancreas. In: Gambill EE, ed. Pancreatitis. Saint Louis, MO, USA: The CV Mosby, 1973:7-11.
- Jones SN, Lees WR, Frost RA. Diagnosis and grading of chronic pancreatitis by morphological criteria derived by ultrasound and pancreatography. Clin Radiol 1988; 39: 43-8. [PMID 3276430]
- Axon AT, Classen M, Cotton PB, Cremer M, Freeny PC, Lees WR. Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25:1107-12. [PMID 6479687]
- Kamisawa T, Yuyangt T, Egawa N, Ishiwata JI, Okamoto A. Patency of the accessory pancreatic duct in relation to its course and shape: a dye-injection endoscopic retrograde pancreatography study. Am J Gastroenterol 1998; 93:2135-40. [PMID 9820386]
- Kamisawa T, Yuyangt T, Egawa N, Sasaki N, Ishiwata JI, Okamoto A. New classification for the accessory pancreatic duct by ERP. Dig Endosc 1998; 10:308-11.
- Andersen BN, Pedersen NT, Scheel J, Worning H. Incidence of alcoholic chronic pancreatitis in Copenhagen. Scand J Gastroenterol 1982; 17:247-52. [PMID 7134849]
- Wornig H. Incidence and prevalence of chronic pancreatitis. In: Beger HG, Büchler M, Ditschuneit H, Malfertheiner P, eds. Chronic Pancreatitis. Berlin, Germany: Springer-Verlag, 1990:8-10.
- Sahel J. Endoscopic retrograde pancreatography findings and their grading in chronic pancreatitis. In: Malfertheiner P, Ditschuneit H, eds. Diagnosis Procedures in Pancreatic Disease. Berlin, Germany: Springer-Verlag, 1987:169-174.
- White TT. Surgical anatomy of the pancreas. In: Carey LC, ed. The Pancreas. Saint Louis, MO, USA: The CV Mosby, 1973:4.
- Tanaka S, Nakaizumi A, Ioka T, Oshikawa O, Uehara H, Nakao M, et al. Main pancreatic duct dilatation: a sign of high risk for pancreatic cancer. Jpn J Clin Oncol 2002; 32:407-11. [PMID 12451037]







