Keywords
Drug Therapy; Palliative Care; Pancreatic Neoplasms
Abbreviations
FOLFIRI: infusional 5-fluorouracil, irinotecan, folinic acid; FOLFIRINOX 5-fluorouracil, leucovorin, oxaliplatin, and irinotecan; FOLFOX: infusional 5-fluorouracil, oxaliplatin, folinic acid
INTRODUCTION
A regimen combining 5-FU, leucovorin, oxaliplatin, and irinotecan (FOLFIRINOX) is the first therapy to show clinically significant survival advantage over single agent gemcitabine in a randomized study in treatment of metastatic pancreatic adenocarcinoma [1]. The appropriate settings for this regimen are being sorted out by academic and community oncologists. The purpose of this paper is to review multi-drug regimens (3 or more drug combination regimens) under development for treatment of pancreas carcinoma to discuss implications for practice and research of pancreatic cancer treatment.
Multi-Drug Regimens with Randomized Phase III Study Data
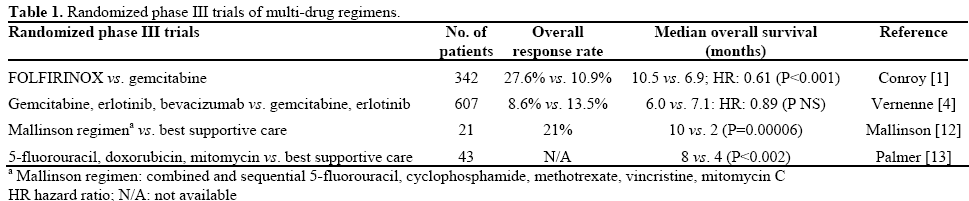
A single arm phase II study tested a feasibility of combining 5-FU, leucovorin, oxaliplatin, and irinotecan (FOLFIRINOX) in treatment of metastatic pancreatic adenocarcinoma. An encouraging signal of activity (26% overall response rate, median overall survival 10.2 months, improved quality of life) generated a hypothesis that FOLFIRINOX may render benefits to metastatic pancreatic adenocarcinoma patients [2]. Then, a randomized phase II study was initiated comparing FOLFIRINOX and gemcitabine as first line treatment of metastatic pancreatic adenocarcinoma patients [3]. The study enrolled chemotherapy naïve patients with good performance status (ECOG 0 or 1) in testing this relatively toxic regimen (grade 3-4 neutropenia, 52%). At the interim analysis of 88 patients treated and 65 evaluable patients, data strongly signaled superiority of FOLFIRINOX over gemcitabine, partial response rates of 38.7% and 11.7%, respectively. Not surprisingly, patients treated with FOLFIRINOX experienced significantly higher rate of grade 3-4 neutropenia and thrombocytopenia [3]. The significant improvement in overall response rate which was the primary endpoint of this study led to the expansion of the trial to a phase III investigation comparing overall survival between FOLFIRINOX and gemcitabine in the first line setting. At the planned interim analysis, the independent data monitoring committee recommended to stop the study when data from 150 evaluable patients showed superiority of FOLFIRINOX to gemcitabine in overall response rate (27.6% vs.10.9%, P=0.0008), median progression free survival (6.4 months vs. 3.4 months; P<0.0001), and median overall survival (11.1 months vs. 6.8 months; HR: 0.61; 95% CI: 0.46-0.81; P<0.001). FOLFIRINOX was considerably more toxic than gemcitabine with most notable difference seen in grade 3-4 neutropenia (47.9% vs.19.2%) and febrile neutropenia (5.7% vs. 0%) [1]. FOLFIRINOX now represents a treatment option for patients with advanced pancreas cancer who has a good performance status.
Gemcitabine and erlotinib combination regimen is an accepted standard of care in treatment of metastatic pancreatic adenocarcinoma following a randomized phase III study showing survival advantage of gemcitabine and erlotinib combination regimen over single agent gemcitabine. Bevacizumab showed promising activity in various cancer types in combination with reference chemotherapy agents hence was added to gemcitabine and erlotinib combination regimen in a randomized placebo (gemcitabine and erlotinib plus placebo) controlled phase III trial in first line setting. Primary endpoint was overall survival, and unlike FOLFIRINOX, patients with Karnofsky performance status of 60% or greater were included in the study. Of 607 evaluable patients for response, there was no statistically significant overall survival improvement by adding bevacizumab to gemcitabine and erlotinib combination regimen although there was a statistically significant improvement in progression free survival with addition of bevacizumab (HR: 0.73; 95% CI: 0.61-0.86; P=0.0002) [4].
In an unplanned subgroup analyses, significant overall survival improvement was noted in patients with tumors located in the tail of the pancreas, elevated baseline C-reactive protein (CRP) and lactate dehydrogenase (LDH). The significance of this post hoc sub-group analysis is largely unknown [4].
There are other multi-drug regimens tested in treatment of pancreatic cancer in small prospective randomized trials. The combination of 5-FU, doxorubicin, and mitomycin and the Mallinson regimen (5-FU, cyclophosphamide, methotrexate, vincristine, mitomycin) were compared with the best supportive care. These small studies suggested that chemotherapy can significantly prolong overall survival compared to “no chemotherapy”. However, these studies do not address value of multi-drug regimens compare to that of single agent gemcitabine (Table 1).
Other Multi-Drug Regimens
Gemcitabine Based
Combination of gemcitabine, docetaxel and capecitabine is based on a novel hypothesis, generated by preclinical studies, which suggested synergistic effects of these three agents by optimizing their administration. This regimen was designed to inhibit MEK-ERK phosphorylation and increase BAX and BAK and also decrease BCL-2 in pancreatic cancer cell lines. A multi-institution retrospective analysis, included 35 metastatic pancreatic adenocarcinoma patients, hinted some activity (overall response rate: 29%), and a prospective phase II study was launched [5].
This single arm phase II study reported data based on 41 patients eligible for assessment. One-year survival rate was 56.0% and 2-year survival rate was 14.6% along with 9 patients (21.9%) who achieved partial responses. The median overall survival was 14.5 months. The regimen showed significant bone marrow toxicity with most common grade 3-4 toxicities being leukopenia (31.6%), neutropenia (29.2%), and thrombocytopenia (12.2%). A randomized phase III trial is needed to further test this regimen [6].
Other Gemcitabine Based Triplet Regimens
There are several gemcitabine based triplet regimens being investigated which are listed in Tables 1 and 2. They are all single arm non-controlled studies (except one study) with small number of patients. Agents used in addition to gemcitabine include oxaliplatin, cisplatin, 5-FU/leucovorin, capecitabine, erlotinib, cetuximab, and bevacizumab in a variety of combinations. Approaches of combining the biologics with nonoverlapping toxicities with traditional cytotoxic agents appear to be a trend; however, all of these regimens and their activity signals ought to be examined further (Table 2).

Non Gemcitabine Based
Unsatisfactory outcomes with various gemcitabine based combination regimens naturally opened up a room for development of non-gemcitabine based combination regimens. FOLFIRINOX, which was discussed earlier, represents the first such regimen that offers survival benefits superior to that of gemcitabine single agent. Irinotecan and docetaxel combination regimen had shown some activity with 9 months median overall survival in a single arm phase II study. Building on this regimen, a prospective randomized study (irinotecan, docetaxel, plus/minus cetuximab) was conducted to confirm the single arm study activity and to examine the feasibility of adding cetuximab. The study failed to meet the pre-specified target of 4 responders in either arm, and addition of cetuximab failed to improve overall survival [7]. Other nongemcitabine based multi-drug regimen included combinations of capecitabine, oxaliplatin, sorafenib, docetaxel, mitomycin, and irinotecan as shown in Table 2, and none of these regimens have adequate data to be used routinely in clinic.
Four Drug Regimen
Gemcitabine also was combined with epirubicin, cisplatin, and 5-FU in a phase II study. In a single arm study, 43 patients with metastatic pancreatic adenocarcinoma were treated, and the study reports overall response rate of 58% and median survival of 11 months. Clinical benefit (pain reduction and improvement of performance status) was achieved in 78% (n=22) of 28 evaluable patients [8]. The combination of gemcitabine, 5-FU/leucovorin, cisplatin, and irinotecan was designed building upon encouraging data of gemcitabine, 5-FU, and cisplatin. A retrospective analysis of 34 patients consecutively treated for metastatic pancreas cancer was conducted. The majority of patients had prior treatment failure with gemcitabine and/or gemcitabine, 5-FU, and cisplatin combination regimen. In this retrospective analysis, 24% of patients had partial response (n=8), and median overall survival for 34 patients was 10.3 months [9].
Discussion
There are many multi-drug regimens investigated in treatment of patients with metastatic pancreatic adenocarcinoma; however, with an exception of FOLFIRINOX, there is no adequate data supporting routine use of multi-drug regimens in treatment of patients with metastatic pancreatic adenocarcinoma. Most multi-drug regimens generally add more toxicity without meaningful survival or clinical benefit. Since FOLFIRINOX will have a role in metastatic pancreatic adenocarcinoma treatment strategy, albeit limited one, discussions are warranted around appropriate use of FOLFIRINOX and other multi-drug regimens currently being developed to safeguard patients and re-think our developmental strategy in this space where progress has been exceptionally slow.
Implications to Practicing Physicians
FOLFIRINOX represents the only combination regimen with statistically and clinically significant survival benefit over gemcitabine. This regimen however should be used with caution due to its relatively high toxicity profile and lack of safety data in patients with ECOG performance status greater than 1. Despite its limitations, FOLFIRINOX offers clinicians and patients an option that does not include gemcitabine or gemcitabine doublets; therefore, its use will grow as clinicians gain more experience. In the absence of phase III data, no other multi-drug regimen should be routinely used outside of clinical trial setting as they expose patients with considerable toxicity without meaningful benefit.
Implications to Investigators
FOLFIRINOX opens a door for seamless transition from gemcitabine based combination strategy which resulted in series of failures. Fluorouracil based regimens such as infusional 5-fluorouracil, oxaliplatin, and folinic acid (FOLFOX) and infusional 5- fluorouracil, irinotecan, and folinic acid (FOLFIRI) have been explored in treatment of metastatic pancreatic adenocarcinoma in second line setting after gemcitabine failure [10]. Natural progression would be testing FOLFOX and FOLFIRI in first line settings. These two regimens, if proven to be effective in first line, would be intriguing backbone therapy for future development of triplets or other multi-drug regimens in pancreas cancer treatment. A successful story of FOLFIRINOX will encourage investigators to explore innovative combination regimens beyond “traditional” backbone agents such as gemcitabine.
FOLFIRINOX is developed specifically for very fit patients with metastatic pancreatic adenocarcinoma due to its toxicity seen throughout it development span. More research is to be conducted to explore other appropriate settings for this regimen. In general, high toxicity profile is considered acceptable in adjuvant setting due to the goal of therapy and better tolerated due to generally better overall status of patients' health. As such, situations where tumor shrinkage or down staging can have a meaningful impact on surgical options would be a reasonable setting for FOLFIRINOX and other future multi-drug regimens.
Future Considerations
One will continue to hit a relatively low ceiling by trying to combine ineffective agents with questionable benefits and substantial toxicities. Efforts to develop novel agents should continue given underwhelming activity of currently available agents. Various iterations of combinations of drugs without a sound rationale will lead to predictable and insignificant advances in the best case scenarios.
Combination regimen being tested should be based on a solid pharmacological rationale. A rigorous preclinical studies and clear evidence of pharmacological synergy should be a prerequisite to a conduct of clinical trials to avoid exposing patients to a potentially detrimental treatment. Similarly, drug-drug interactions must be carefully evaluated in early developmental stage of multi-drug regimens not only to prevent untoward interactions but also to take advantage of potential favorable pharmacokinetic/ pharmacodynamic interactions.
Inefficient and suboptimal conduct of earlier phase II trials were identified as one reason for a high attrition rate of oncology drugs in phase III trials. Taking signals from uncontrolled single arm studies as a “go to phase III” decision is well recognized culprit of such high failure rate of oncology phase III studies [11]. Pancreas cancer studies have not been the exception to this practice and contributed to wasted resources, lost opportunity cost, and exposure of patients to ineffective and potentially harmful regimens. Data from randomized phase II study does not guarantee a success of any phase III trial; however, it will certainly improve probability of success as it was seen in the development of FOLFIRINOX where relatively small randomized phase II data was used to make a successful “go to phase III” decisions.
Conflict of interest
The authors have no potential conflict of interest
References
- T. Conroy FD, M. Ychou, M. Ducreux, O. Bouche, R. Guimbaud, Y. Becouarn, C. Montoto-Grillot, S. Gourgou-Bourgade, A. Adenis, FNCLCC-FFCD PRODIGE Group. Randomized phase III trial comparing FOLFIRINOX (F: 5FU/leucovorin [LV], irinotecan [I], and oxaliplatin [O]) versus gemcitabine (G) as firstline treatment for metastatic pancreatic adenocarcinoma (MPA): Preplanned interim analysis results of the PRODIGE 4/ACCORD 11 trial. J Clin Oncol 28:abstr 4010, 2010
- T. Conroy BP, E. Francois, G. Deplanque, R. Bugat, J.-H. Jacob, U. Stein, S. Nasca, E. Magherini, J.-P. Metges; Ctr Alexis Vautrin, Vandoeuvre-Les Nancy, France. Final results of folfirinox: A triple combination of 5-FU/leucovorin (5-FU/LV), irinotecan (I) and oxaliplatin (O)] as first-line chemotherapy in advanced pancreatic adenocarcinoma (APA). Proc Am Soc Clin Oncol 22, 2003
- M. Ychou FD, R. Guimbaud, M. Ducreux, O. Bouché, Y. Bécouarn, A. Adenis, C. Montoto-Grillot, E. Luporsi, T. Conroy Randomized phase II trial comparing folfirinox (5FU/leucovorin [LV], irinotecan [I] and oxaliplatin [O]) vs. gemcitabine (G) as firstline treatment for metastatic pancreatic adenocarcinoma (MPA). First results of the ACCORD 11 trial. Journal of Clinical Oncology, 2007 ASCO Annual Meeting Proceedings Part I 25:4516, 2007
- Vervenne W BJ, Humblet Y, Gill S, Moore MJ, Van Laethem J, et al. A randomized, double-blind, placebo (P) controlled, multicenter phase III trial to evaluate the efficacy and safety of adding bevacizumab (B) to erlotinib (E) and gemcitabine (G) in patients (pts) with metastatic pancreatic cancer. J Clin Oncol 26:abstract 4507, 2008
- Fine RL, Fogelman DR, Schreibman SM, et al. The gemcitabine, docetaxel, and capecitabine (GTX) regimen for metastatic pancreatic cancer: a retrospective analysis. Cancer Chemother Pharmacol 61:167-75, 2008
- R. L. Fine GM, W. Sherman, K. Chu, M. Maurer, J. Chabot, I. Postolov, J. Prowda, S. Schreibman, J. Levitz Phase II trial of GTX chemotherapy in metastatic pancreatic cancer. J Clin Oncol 27:abstract 4623, 2009
- B. A. Burtness MEP, J. D. Berlin, D. K. Liles, A. E. Chapman, E. P. Mitchell, A. B. Benson Phase II ECOG trial of irinotecan/docetaxel with or without cetuximab in metastatic pancreatic cancer: Updated survival and CA19-9 results. J Clin Oncol 26:abstr 4642, 2008
- Reni M, Passoni P, Panucci MG, et al Definitive results of a phase II trial of cisplatin, epirubicin, continuous-infusion fluorouracil, and gemcitabine in stage IV pancreatic adenocarcinoma. J Clin Oncol 19:2679-86, 2001
- Kozuch P, Grossbard ML, Barzdins A, et al Irinotecan combined with gemcitabine, 5-fluorouracil, leucovorin, and cisplatin (G-FLIP) is an effective and noncrossresistant treatment for chemotherapy refractory metastatic pancreatic cancer. Oncologist 6:488-95, 2001
- Yoo C, Hwang JY, Kim JE, et al A randomised phase II study of modified FOLFIRI.3 vs. modified FOLFOX as second-line therapy in patients with gemcitabine-refractory advanced pancreatic cancer. Br J Cancer 101:1658-63, 2009
- Sharma MR, Maitland ML, Ratain MJ Other paradigms: better treatments are identified by better trials: the value of randomized phase II studies. Cancer J 15:426-30, 2009
- Mallinson CN, Rake MO, Cocking JB, et al Chemotherapy in pancreatic cancer: results of a controlled, prospective, randomised, multicentre trial. Br Med J 281:1589-91, 1980
- Palmer KR, Kerr M, Knowles G, et al Chemotherapy prolongs survival in inoperable pancreatic carcinoma. Br J Surg 81:882-5, 1994
- H. L. Kindler KAB, H. S. Hochster, G. Friberg, K. Micetich, G. Locker, M. Kozloff, M. Moore, W. Sun, E. E. Vokes A randomized phase II study of bevacizumab (B) and gemcitabine (G) plus cetuximab (C) or erlotinib (E) in patients (pts) with advanced pancreatic cancer (PC): A preliminary analysis Journal of Clinical Oncology, 2006 ASCO Annual Meeting Proceedings (Post-Meeting Edition 24:4040, 2006
- F. Kullmann SH, M. Dollinger, J. Harder, M. Fuchs, H. Messmann, J. Trojan, E. Gaebele, A. Hinke, E. Endlicher Cetuximab plus gemcitabine/oxaliplatin (GEMOXCET) in 1st line metastatic pancreatic cancer. First results from a multicenter phase II study. 2007 Gastrointestinal Cancers Symposium General Poster Session C 2007
- Correale P, Montagnani F, Miano S, Sciandivasci A, Pascucci A, Petrioli R, Testi W, Tanzini G, Francini G. Biweekly triple combination chemotherapy with gemcitabine, oxaliplatin, levofolinic acid and 5-fluorouracil (GOLF) is a safe and active treatment for patients with inoperable pancreatic cancer. J Chemother. 2008 Feb;20(1):119-25.
- Garnier C RC, Chirpaz E et al Phase II study of a combination with leucovorin (LV), 5-FU bolus and infusion (FU), gemcitabine and oxaliplatin (FOLFU GEMOX regimen) in locally advanced (LA) and metastatic (M) pancreatic carcinoma (APC). Proc Am Soc Clin Oncol 20, 2001
- Oh D LK, Lee K, Sohn C, Park Y, Zang D, et al. A phase II trial of erlotinib in combination with gemcitabine and capecitabine in previously untreated metastatic/recurrent pancreatic cancer: Combined analysis with translational research. J Clin Oncol 27:abstract 4607, 2009
- Kozuch P AM, Homel P et al. Biweekly sequential gemcitabine, 5-FU (5-fluorouracil), LV (leucovorin), and cisplatin (GFP): a highly active novel combination for metastatic adenocarcinoma of the exocrine pancreas (MPAC). Proc Am Soc Clin Oncol 20, 2001
- Lubner SJ SW, Mulkerin D, Holen KD, Seo S, Lo Conte NK. Phase II study of oxaliplatin, high-dose capecitabine, and sorafenib in patients with advanced pancreatic cancer. J Clin Oncol 28:4143, 2010
- Reni M, Panucci MG, Passoni P, et al Salvage chemotherapy with mitomycin, docetaxel, and irinotecan (MDI regimen) in metastatic pancreatic adenocarcinoma: a phase I and II trial. Cancer Invest 22:688-96, 2004

