Jerko Brzica1, Marjana Jerkovi? Raguž1*, Ivanka Mikuli?2, and Matea Jelavi?3
1Department of Neonatology and Intensive Care Unit, Clinic for Children's Diseases, University Clinical Hospital Mostar, Bosnia and Herzegovina
2Department of Laboratory Medicine, University Clinical Hospital Mostar, Bosnia and Herzegovina
3Faculty of Medicine, University of Mostar, Bosnia and Herzegovina
*Corresponding Author:
Marjana Jerkovi? Raguž
Department of Neonatology and Intensive Care Unit
Clinic for Children's Diseases, University Clinical Hospital Mostar
Bosnia and Herzegovina
Tel: 38763699089
E-mail: marjanajerkovic@yahoo.co.uk
Received Date: Mar 16, 2017 Accepted Date: Mar 27, 2017 Published Date: Mar 31, 2017
Citation: Brzica J, raguz MJ, Mikulic I, et al. Thrombocytopenia: Diagnostic Tool of Neonatal Infection? Gynecol Obstet Case Rep 2016, 3:1.
Objective: To research the occurrence of thrombocytopenia in the newborn and to establish the connection of thrombocytopenia with risk factors.
Materials and methods: The study encompassed 136 newborn, to whom thrombocytopenia diagnosis was confirmed in laboratory test, and who were treated at the neonatal intensive care unit (NICU) at the Clinic for Children’s Diseases at the University Clinical Hospital in Mostar (SKB) in Mostar.
Results: Out of the total number of 1164 newborn who were treated at the NICU during a two-year period, 2013/2014, at the University Clinical Hospital in Mostar, 136 (11.7%) newborn had thrombocytopenia. Risk factors from mother’s side that affected development of thrombocytopenia were medications 53.7%, cigarettes consumption 56.6% and complications at delivery 34.6%. Placental insufficiency occurred in 32.4% newborn. Out of the total number of the newborn with thrombocytopenia, 38.2% suffered from some kind of infection (sepsis, urinary system infection, bacteraemia...), which is one of the main risk factors for development of thrombocytopenia on the side of the newborn. The most frequently isolated cause was Escherichia coli, which was isolated in 19.9% examinees.
Conclusion: This study shows that the most important risk factors for development of thrombocytopenia in the newborn at the NICU are the risk factors on the side of the mother.
Keywords
Newborn; Thrombocytopenia; Pregnancy
Introduction
Thrombocytopenia of the newborn is defined by thrombocytes count under 150 × 109/L, equally in preterm and full-term newborn [1]. About 30% of the newborn at the time of hospitalization at the NICU has one episode of thrombocytopenia [2]. Accelerated consumption of thrombocytes and their sequestration from blood are the main causes of 25% to 35% neonatal thrombocytopenia. Out of all thrombocytopeniae manifested at birth, 15% to 20% are result of transplacental transmission of mother’s antibodies, and disseminated intravascular coagulation, which is responsible for the remaining 10% to 15% cases, almost always occurs in the newborn with poorer clinical status and is connected with prenatal asphyxia and infection [3-5]. The newborn may develop thrombocytopenia due to various neonatal complications, such as: infection, perinatal asphyxia, respiratory distress syndrome, polycythaemia and necrotizing enterocolitis. In such cases, it is justified to treat the underlying condition, and thrombocytopenia only symptomatic. In case that after being cured thrombocyte, number does not elevate, the possibility exists that this is the immune-mediated thrombocytopenia. Necrotizing enterocolitis (NEC) ad sepsis are the main causes of late thrombocytopenia, which in both cases appears about 8 days upon birth. After causal therapy, normalization of thrombocytes value should occur within 5 to 7 days, and if not, that is a warning to the doctor to look for another cause of disease. In majority of sick newborn, despite diagnostic processing, the cause of thrombocytopenia remains unknown [1,6,7]. Transfusion of thrombocytes for now represents the only currently available therapy for most children with thrombocytopenia. Except as therapy indication, thrombocyte transfusion can be administered prophylactically in the newborn who do not bleed, and that actually represents the most common indication for application of thrombocytes transfusion, even though no studies exist that would show whether transfusion lowers the risk of bleeding and improves the outcome of the newborn treatment [7]. A study published in 2012 shows that on global level criteria for thrombocytes transfusion are lowering and application of recombinant thrombopoietin in the newborn who require more frequent application of thrombocyte concentrate is to be considered [2]. On the other hand, complications connected with application of thrombocytes concentrate are insufficiently known. It was proven that out of all blood preparations, risk of infection is the highest precisely in thrombocytes, which, unlike other blood derivatives, are storaged at a temperature of 20°C to 25°C, and by that, they represent the most favorable medium for bacteria development [8].
Materials and Methods
We conducted a retrospective study at the Clinic for Gynecology and Obstetrics and at the NICU at the clinic for children’s diseases of the university clinical hospital Mostar (UHC) during the two-year period of time, 2013 and 2014. The study encompassed 136 newborn with thrombocytopenia. At the Institute for Laboratory Diagnostics at the UHC Mostar the referential interval of thrombocyte values is from 150 to 450 x 109/l. All samples were tested at hematological analysator Sysmex XT 2000i (Sysmex, Canada). Therefore, out of the total of 1164 newborn treated at the NICU at the Clinic for Children’s Diseases of UHC Mostar in the period from January 1st, 2013 to December 31st, 2014, 136 newborn had thrombocyte values <150 x 109/L and were diagnosed with thrombocytopenia. This study excluded newborn and mothers with a diagnosis of autoimmune thrombocytopenia. Data on the mothers were collected from medical documents and health charts of pregnant women during their stay at the Clinic for Gynecology and Obstetrics. Data on the newborn were collected from medical history and protocol-taking of the newborn in the course of hospitalization. To test statistical significance, x2test and Fisher’s exact test were used where necessary. Level of probability p<0.05 was taken as statistically significant.
Results
During the two-year period, 2013/2014, at the NICU of the UHC Mostar the total of 1164 newborn were treated. Out of 1164 newborn, thrombocytopenia was found in 136 examinees (11.7%).
Of the total number of infants with thrombocytopenia 36 of them (26.5%) were born before 37 weeks’ gestational age, 99 of them (72.8%) were born in the period from 37th to 42nd week of gestational age and 1 infant after 42 weeks of gestational age (0.7%) (Figure 1).
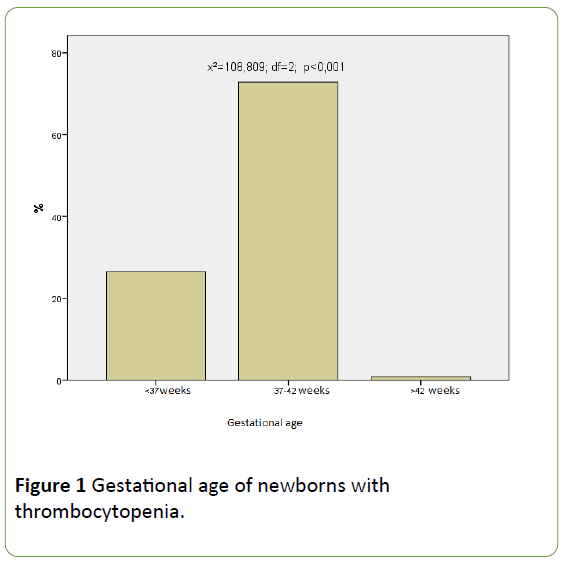
Figure 1: Gestational age of newborns with thrombocytopenia.
Infections risk factor for development of thrombocytopenia was discovered in 38.2% newborn, while 61.8% newborn were without infection. Statistically significantly higher number of children did not have an infection along with thrombocytopenia test result (x2=7.529; df=1; p<0.001) (Figure 2).
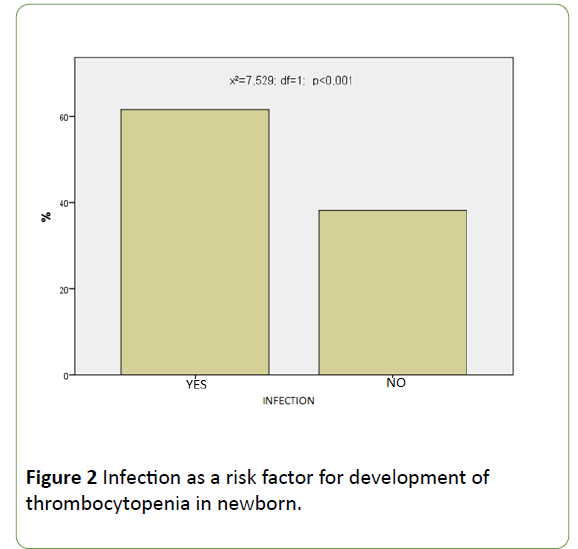
Figure 2: Infection as a risk factor for development of thrombocytopenia in newborn.
One of the risk factors on the side of mother are complications during labor, such as: narrower pelvis, intrauterine infection, bleeding in the third stage of labor and so on. In our study 34.6% mothers had complications during labor, and 65.4% mothers had delivery with a normal course. There is a statistically significant difference between the mothers who had some kind of complication during labor in relation to those mothers who did not have the same complications. (x2=12.971; df=1; p<0.001) (Figure 3).
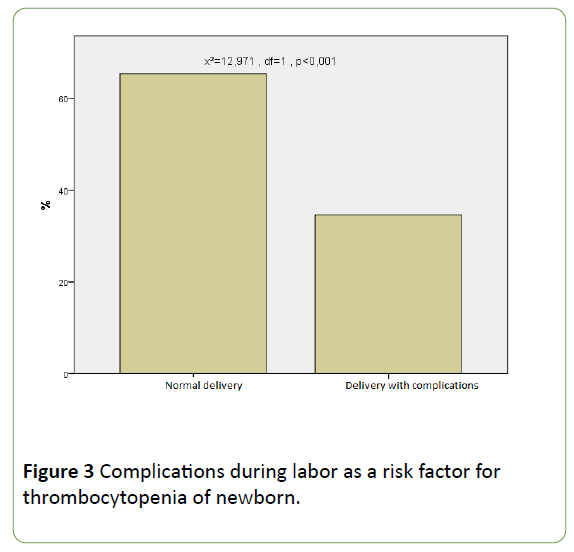
Figure 3: Complications during labor as a risk factor for thrombocytopenia of newborn.
Placental insufficiency was risk factor in 32.4% newborn, while 67.6% newborn did not have placental insufficiency as risk factor. Statistically significantly higher number of children did not have placental insufficiency as risk factor for development of thrombocytopenia. (x2=16.941; df=1; p<0.001).
The most frequently isolated cause in microbiological samples (blood, urine, cerebrospinal fluid, tracheal aspirates) of the newborn hospitalized at the NICU was Escherichia coli (E. coli), which was isolated in 19.9% newborn. On the second place by frequency came Klebsiella pneumoniae (K. pneuminae), which was isolated in 11% newborn hospitalized at the NICU. In 5.9% Enterococcus species was isolated. The remaining causes (Candida albicans, Proteus mirabilis, Serratia marcescens, Staphylococcus aureus) were detected in 19.9% examinees (Table 1).
| Isolated Bacteria as a Cause of Infection |
| |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
| No infection |
59 |
43.4 |
43.4 |
43.4 |
| E. coli |
27 |
19.9 |
19.9 |
63.2 |
| K. pneumoniae |
15 |
11.0 |
11.0 |
74.3 |
| Enterococcus species |
8 |
5.9 |
5.9 |
80.1 |
| Other |
27 |
19.9 |
19.9 |
100.0 |
| Total |
136 |
100.0 |
100.0 |
|
Table 1: Isolated bacteria as a cause of infection of newborn with thrombocytopenia.
Out of the total number of the mothers of the newborn with thrombocytopenia, 56.6% mothers consumed cigarettes during pregnancy and 43.4% mothers did not consume cigarettes during pregnancy. No statistically significant difference was found in the occurrence of thrombocytopenia in the children born by the mothers who consumed cigarettes in relation to children by the mothers who did not consume cigarettes (x2=2.382; df=1; p=0.132).
Discussion
In the study that we conducted for the two-year period, 2013/2014, at the UHC Mostar, it was shown that occurrence of thrombocytopenia in the newborn treated at the NICU was 11.7%, which proves that frequency of thrombocytopenia in our region is still high among the newborn hospitalized at the NICU. A similar study carried out in Indonesia showed that thrombocytopenia in the children hospitalized at the NICU was 12% [9]. On the other hand, a research published in 2009 suggests that thrombocytopenia was confirmed in laboratory test results in 22% to 35% newborn hospitalized at the NICU [10]. The implemented study showed that out of 136 newborn who had thrombocytopenia, 34.6% mothers went through some type of complication during labor, such as: narrower pelvis, intrauterine infection, bleeding in the third stage of labor and so on. Placental insufficiency as risk factor for development of thrombocytopenia in the newborn in our study was found in 32.4% examinees, while some authors reduce the risk of thrombocytopenia development due to placental insufficiency to 1% [11]. In neonatological literature the above is explained by the fact that hypoxia in the newborn triggers abundant erythropoesis, which reduces the amount of progenitor cells needed for differentiation of megakaryocytes into thrombocytes [12]. The study implemented by Aman and Hassan showed that 40.7% newborn had some kind of neonatal infection [13], which is similar to our results, according to which 38.2% newborn had an infection. The mechanism that leads from infection to thrombocytopenia development has not been sufficiently clarified yet, but a research conducted by author Lambert et al. suggests that the answer hides in increased production of thrombocyte factor 4 which is emitted by activated thrombocytes during a septic condition [14]. Gram-negative bacteria E. coli was isolated as the most frequent cause of thrombocytopenia in the newborn in our study (19.9%), which is in accordance with the study by American authors. They point out that, despite the trend of predomination of gram-positive infections at Intensive Care Units of third level, thrombocyte count remains significantly lower in the newborn with gram-negative infections. In spite of prevention and recommendation about damaging effects of cigarette consumption in pregnancy, occurrence of smoking among pregnant women in our study was 56.6%. Despite that, there is no increased incidence of thrombocytopenia in the newborn by the mothers who consumed cigarettes. Taking into consideration a study by a group of authors implemented on a group of 58216 pregnant women who consumed cigarettes, the result of our study is not surprising. It was proven in the above motioned study that in all groups of examined women cigarettes consumption reduced the risk of preeclampsia, which showed to be an important risk factor for development of thrombocytopenia in the newborn in our study.
Conclusion of this Study
It is the better prenatal and antenatal prevention of risk factors in pregnant women is necessary. Apart from that, attention should be paid on the early detection of thrombocytopenia in the newborn hospitalized at the NICU, because development of severe infection and at the same time high mortality in the risky group of the newborn can be prevented.
COI Statement
The manuscript has not been published or submitted for publishing elsewhere, the manuscript has been read and approved by all the authors, and there is no any financial or other conflict of interest.
References
- Mardešić D (2003) Diseases of the blood and blood-forming organs. In: Mardešić, et al. Pediatrics. Zagreb: Mladost 664-683.
- Gupta AK, Kumari S, Singhal A, Bahl A (2012) Neonatal thrombocytopenia and platelets transfusion. Asian J Transfus Sci 6: 161-164.
- Castle V, Andrew M, Kelton J (1986) Frequency and mechanism of neonatal thrombocytopenia. J Pediatr 108: 749-755.
- Sainio S, Jarvenpaa AS, Renlund M (2000) Thrombocytopenia in term infants, a population based study. Obstet Gynecol 95: 441-446.
- Uhrynowska M, Niznikowska-Marks M, Zupanska B (2000) Neonatal and maternal thrombocytopenia: Incidence and immune background. Eur J Haematol 64: 42-46.
- de Alarcon P, Werner W, Robert D (2013) Neonatal haematology pathogenesis, diagnosis and management of hematologic problems. Cambridge: Cambridge University Press.
- Andrew M, Vegh P, Caco C (1993) A randomized, controlled trial of platelet transfusions in thrombocytopenic premature infans. J Pediatr 123: 285-291.
- Stanworth SJ (2012) Thrombocytopenia, bleeding, and use of platelet transfusions in sick neonates. ASH Education Book no. 1512-516.
- Kusamsari N, Rohsiswatmo R, Gatot D (2010) Incidence and risk factors of neonatal thrombocytopenia. Pediatr Indonesia 1: 50-60.
- Baer VL, Lambert DK, Henry E, Christensen RD (2009) Severe thrombocytopenia in the NICU. Pediatrics 124: 1095-100.
- Sola-Visner M, Hannes S, Brown R (2009) New insights into the mechanisms of non-immune thrombo cytopenia in neonates. Semin Perinatol 33: 43-51.
- Aman I, Hassan KA, Ahmad TM (2004) The study of thrombocytopenia in sick neonates. J Coll Physicians Surg Pak 14: 282-285.
- Lambert MP, Rauova L, Bailey M, Sola-Visner MC, Kowalska MA, et al. (2007) Platelet factor 4 is a negative autocrine in vivo regulator of megakaryopoiesis: Clinical and therapeutic implications. Blood 110: 1153-1160.
- Guida JD, Kunig AM, Leef KH, McKenzie SE, Paul DA (2003) Platelet count and sepsis in very low birth weight neonates: Is there an organism-specific response? Pediatrics 111: 1411-1415.

